
Abstract
Endoscopic sinus surgery (ESS) for patients with severe chronic rhinosinusitis (CRS) has become a well-established treatment in cases where medical therapy fails. Even though CRS patients are divided into two subgroups, CRS with nasal polyposis (CRSwNP) and CRS without nasal polyposis (CRSsNP), most studies present only results for the total cohort. This prospective cohort study evaluated the efficacy of ESS on both quality of life and olfactory function measures, in a cohort of Danish CRS patients diagnosed according to the EPOS criteria, with results analysed separately for the CRSwNP and CRSsNP subgroups. All 97 CRS patients who underwent ESS over an 18-month trial period were evaluated preoperative by SNOT-22 score, Sniffin’ Sticks score, modified Lund–Kennedy endoscopic score and Lund–Mackay CT score. Patient outcomes were reevaluated at clinical follow-up 1 and 6 months postoperative. ESS efficiently and immediately improved quality of life for both CRSwNP and CRSsNP patients, with over 50 % reduction in SNOT-22 score 1 month after surgery, which sustained 6 months postoperative. Olfactory function measured by Sniffin’ Sticks score showed overall improvement in both groups. ESS efficiently improved quality of life in both CRSwNP and CRSsNP patients, and surgery lead to an overall improvement in olfactory function. However, a minor proportion of patients experienced deterioration in olfactory function after ESS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic rhinosinusitis (CRS) with or without nasal polyps (CRSwNP/CRSsNP) is a common chronic condition with profound health-related and socio-economic consequences [1]. A large multicentre study based on questionnaires has shown an overall prevalence of CRS at 10.9 % in Europe [2], and in a recent Danish study the CRS prevalence was 8.5 % [3]. The high prevalence of CRS covers a broad spectrum of disease severity. Previous European studies have evaluated the efficacy of endoscopic sinus surgery ESS showing positive effect on patient-reported quality of life measures [4], but also optimization of medical treatment alone has proven effective [5]. In many studies on ESS the inclusion criteria were not well defined, with possible large diversity in terms of sino-nasal illness and severity, previous medical treatment, and the extent of sinus surgery performed. Over the last decade there has been an increasing awareness of clearly defining the various sino-nasal disorders by diagnostic criteria, and subdivision with regard to severity, which serves the purpose of tailoring the treatment to the extent of the disease [6]. ESS for patients with CRS is considered a well-established surgical method in cases where medical therapy fails [6]. Still only few studies gather the results of both quality of life measures and olfactory function after ESS in CRS patients diagnosed according to the criteria of the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) [7, 8], and no studies provide results specific for the CRSsNP subgroup.
The aim of this study was to evaluate the efficacy of ESS on both quality of life and olfactory function measures, in a cohort of Danish CRS patients diagnosed strictly according to EPOS, using the recent objective and subjective measures based on European guidelines [6]. Results were analysed separately for the CRSwNP and CRSsNP subgroups.
Materials and methods
Study design
The study was designed as a prospective cohort study. All patients referred to the department of otorhinolaryngology, Svendborg Hospital, Denmark, for ESS in an 18-month period from June 2012 to November 2013, were evaluated for CRS according to the EPOS criteria. Patients diagnosed with CRS who experienced inadequate response to nasal steroid, were enrolled in the study. Exclusion criteria were age under 15, inability to fill out the questionnaires due to poor language skills, benign or malignant tumour, and patients with gross immunodeficiency, vasculitis, granulomatous disease, cystic fibrosis or known aspirin exacerbated respiratory disease.
The study was designed to be representative of the daily clinical practice in the department, and was therefore a multi-examiner/surgeon study, including four consultants and specialist registrars working under supervision.
Preoperative examination
Preoperatively patients completed the Danish validated version of the sino-nasal outcome test 22 (SNOT-22) questionnaire [9] and items regarding asthma symptoms and smoking habits. The surgeons systematically recorded the relevant sino-nasal medical history, along with a detailed rhinological examination including nasal endoscopy and an olfactory function test, the Sniffin’ Sticks test. Based on the nasal endoscopy a modified Lund–Kennedy endoscopy score (MLK score) was calculated. Lund–Mackay CT score was calculated based on the preoperative computed tomography (CT) scan.
Surgery
All patients had ESS performed in general anaesthesia. The extent of surgery was tailored to the extent of disease, but included surgical opening of minimum one sinus.
Postoperative follow-up
After ESS all patients were prescribed nasal steroid treatment and instructed to use this twice daily during follow-up. Clinical follow-up was performed 1 and 6 months after surgery. At 1 month follow-up patients filled out the SNOT-22 questionnaire, and nasal endoscopy with calculation of MLK score was performed. At 6 months follow-up the SNOT-22 score was re-administrated. Further, the MLK score and the Sniffin’ Sticks test were repeated.
Outcome measures
The main outcome measure was the SNOT-22 score and test of olfactory function. The SNOT-22 score is a patient-reported measure of symptom severity and health-related quality of life in sino-nasal conditions. It contains 22 items, and symptom severity is graded 0–5 producing a sum score ranging from 0 to 110, with high scores indicating severe rhinosinusitis-related health burden [10]. The 22 items can be divided into four subscales: rhinological symptoms (q 1–5, 7, 8), ear and facial symptoms (q 9–12), sleep function (q 13–15) and psychological issues (q 17–22) enabling a more detailed analysis of the change in quality of life [11].
Olfactory function was assessed using the Sniffin’ Sticks odour identification test (12 odour kit, Burghart Company, Wedel, Germany) [12–14]. This is a standardised test where 12 scents are individually presented for the patient to identify by multiple choice. A score of 11–12 points is categorised as normal olfactory function. This test was chosen as it is a simple and fast test allowing it to be implemented in the daily clinical practice [12, 13, 15].
The MLK score is a simplified version of the Lund–Kennedy endoscopic scoring system [16, 17], which was original designed for describing endoscopic findings postoperatively after sinus surgery by scoring: polyps, edema, discharge, scaring and crusting. In the MLK score scaring and crusting are omitted, thus the score is calculated by evaluating each side of the nasal cavity for: polyps, edema, and discharge (0, 1 or 2) producing a sum score between 0 and 12 points. In a recent study the MLK score was shown to have the highest inter-rater and test–retest reliability when compared to other endoscopic scoring systems, and was found best suited for clinical practice and research purpose [17].
The Lund–Mackay CT score is a grading system dependent on CT scan findings. This scoring system consists of a scale of 0–2 dependent on the absence, partial or complete opacification of the sinus system and the osteomeatal complex. A maximum score of 24 can be obtained [18–20].
Statistical methods
Statistical analysis was undertaken separately for the CRSwNP and CRSsNP group, including descriptive statistics on patient characteristics and multivariable linear regression on SNOT-22 data to test the influence of possible covariates (sex, age, asthma and smoking). The same was performed with the Sniffin’ Sticks score, MLK score, and Lund–Mackay CT score using ordinal regression analysis. Differences between the preoperative and postoperative outcome measures were analysed using the Wilcoxon signed rank test, while differences between the CRSwNP and CRSsNP groups were analysed by Mann–Withney U test.
Correlations between the objective measures Lund–Mackay CT score and MLK score to the outcome measures SNOT-22 score and Sniffin’ Sticks score were evaluated using Spearman’s rank correlation. p values of <0.05 were considered to be statistically significant. Statistical analysis was performed using Stata version 13.1.
Ethics approval
The study was approved by the Regional Ethics Committee and by the Danish Data Protection Agency, No. 2008-58-0035.
Results
During the 18-month trail period a total of 113 patients met the inclusion criteria. The following patients were excluded: one patient declined to participate in the study; one patient was below the age of 15; four patients due to poor language skills; in one patient histology showed invert papilloma; five patients cancelled their planned operation; one patient had surgery performed elsewhere; three patients were missed at random. Thus, a total of 97 patients (67 males, 30 females) were enrolled in the study and underwent ESS. Ninety-one patients (94 %) participated at 1 month follow-up, and 88 (91 %) participated at 6 months follow-up.
A total of 75 (77 %) were preoperatively diagnosed having CRSwNP, and 22 patients (23 %) were diagnosed as CRSsNP. The mean age for the total cohort was 50.5 years, with no significant differences between the two groups. Seventy-one percent of the patients in the CRSwNP group were male, compared to 64 % in the CRPsNP group. In the CRSwNP group 16 % were smokers, 25 % were former smokers, and 28 % had asthma, and in the CRSsNP group 14 % were smokers, 36 % were former smokers and 10 % had asthma. Previous sinus surgery had been performed in 31 % of the patients in the CRSwNP group, whereas only one patient (5 %) in the CRSsNP group had previous sinus surgery. An overview of the surgery performed in this study is given in Table 1. At 6 months follow-up 86 % of the CRSwNP group, and 67 % of the CRSsNP group were continuously in nasal steroid treatment.
Cohort characteristics and results of the study are summarised in Table 2.
Lund–Mackay CT score
The mean Lund–Mackay CT score was 16.4 points in the CRSwNP group. With 71 % of the patients having extensive mucosal swelling (CT score 14–24 points), while 25 % had limited changes (CT score 4–13 points), and 3 % had no significant changes (CT score 0–3 points).
In the CRSsNP group the mean Lund–Mackay CT score was 10.9 points. Thirty-three percent had extensive mucosal swelling (CT score 14–24 points), and the remaining 67 % had limited changes (CT score 4–13 points).
Modified Lund–Kennedy endoscopic score
In the CRSwNP group the preoperative MLK score was 7.9 points. At 1 and 6 months follow-up it was 2.9 and 2.7, respectively. In the CRSsNP group the preoperative MLK score was 4.2 points. At 1 and 6 months follow-up it was 2.0 and 2.1, respectively. The reductions in MLK scores after ESS were statistically significant in both groups.
SNOT-22 score
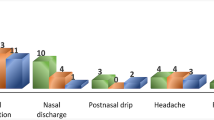
The mean preoperative SNOT-22 score was 43.6 points for both the CRSwNP and CRSsNP group. In the CRSwNP group the four highest rated symptoms were “nasal obstruction”, “need to blow nose”, “loss of smell” and “runny nose”. In the CRSsNP group the four highest rated symptoms were “nasal obstruction”, “post-nasal discharge”, “facial pain”, and “thick nasal discharge”. In the CRSwNP group the SNOT-22 score at 1 month follow-up was 17.3 and at 6 months follow-up 16.6. In the CRSsNP group the SNOT-22 score at 1 month follow-up was 21.0 and at 6 months follow-up 20.1. The reduction in SNOT-22 score after ESS was statistically significant in both groups. The preoperative SNOT-22 score and the change in SNOT-22 score at 6 months follow-up were not significantly related to age, sex, asthma, or smoking status.
At 6 months follow-up there were reductions in mean score for all 22 items that constitute the SNOT-22 score (Figs. 1, 2), with significant reductions in all four subscales (rhinological symptoms, ear and facial symptoms, sleep function and psychological issues) in both the CRSwNP and CRSsNP group.

CRSwNP group, mean scores of each SNOT-22 item, preoperative and at 6 months follow-up

CRSsNP group, mean scores of each SNOT-22 item, preoperative and at 6 months follow-up
Analysing correlations between the SNOT-22 score and the objective findings, we found significant positive correlations between the preoperative SNOT-22 score to both the Lund–Mackay CT score and preoperative MLK score in the CRSwNP group. Performing corresponding correlation analysis on data from the CRSsNP group, no significant correlations were found.
A corresponding positive correlation was found between the SNOT-22 score and the MLK score at 6 months follow-up in the CRSwNP group. The postoperative change in SNOT-22 score was positively correlated to both the Lund–Mackay CT score and preoperative MLK score, as higher preoperative scores predicted larger SNOT-22 reductions at 6 months follow-up in the CRSwNP group. The correlation analysis results are summarised in Table 3.
Olfactory function
The mean preoperative Sniffin’ Sticks score was 6.4 points in the CRSwNP group and 8.6 points in the CRSsNP group. At 6 months follow-up there was a statistically significant increase in mean Sniffin’ Sticks score to 7.5 points in the CRSwNP group. The CRSsNP group showed a non-significant increase to 9.4 points. The difference in olfaction ability between the CRSwNP and CRSsNP groups measured by Sniffin’ Sticks were statistically significant, both preoperatively and 6 months postoperative. The preoperative Sniffin’ Sticks score and the change in Sniffin’ Sticks score at 6 months follow-up were not significantly related to age, sex, asthma, or smoking status.
Analysing the preoperative Sniffin’ Sticks score in the CRSwNP group, we found significant negative correlations to both the Lund–Mackay CT score and preoperative MLK score. In the CRSsNP group there was a corresponding, but non-significant, tendency between the Sniffin’ Sticks score and the Lund–Mackay CT score, while no correlation was found related to the MLK score.
Analysing the CRSwNP and CRSsNP groups separately there were no significant correlations between the postoperative change in Sniffin’ Sticks score and Lund–Mackay CT score or MLK score. Analysing the whole cohort as one, we found a positive correlation between postoperative change in Sniffin’ Sticks score and the Lund–Mackay CT score. The correlation tendency was found moderate in the CRSsNP group, but weak in the CRSwNP group.
At 6 months follow-up, a negative correlation between the Sniffin’ Sticks score and MLK score was found significant in the CRSwNP group. In the CRSsNP group there was a corresponding, but non-significant tendency.
Another way to analyse the results of the Sniffin’ Sticks test is by using a conservative definition introduced by Pade and Hummel [13]. They defined a change of olfactory function as a change in Sniffin’ Sticks score by 3 or more points. Applying this to data of the CRSwNP group showed that 25 % had improvement, 68 % were unchanged, and 7 % had deterioration in olfactory function 6 months after ESS. In the CRSsNP group 24 % had improvement, 66 % were unchanged, and 10 % had deterioration in olfactory function 6 months after ESS.
Analysing patients preoperative Sniffin’ Sticks scores in relation to their olfactory outcome after ESS, we found that patients who experienced a decrease in Sniffin’ Sticks score, had a significantly higher preoperative Sniffin’ Sticks score, compared to those who improved in Sniffin’ Sticks score after ESS (p < 0.05).
Discussion
This study showed that ESS efficiently improved quality of life for both CRSwNP and CRSsNP patients, and that surgery led to an overall improvement in olfactory function.
Quality of life improvement was not only related to the rhinological symptoms, but was significant for all four subscales of the SNOT-22 test.
In CRSwNP patients we found correlation between the severity of objective findings (Lund–Mackay CT score and MLK score) and the patients quality of life (SNOT-22 score) and olfactory function (Sniffin’ Sticks score), respectively, both preoperative and 6 months postoperative. Furthermore, we found correlation between the severity of preoperative objective findings to the size of quality of life improvement 6 months postoperatively for CRSwNP patients.
Strengths and weakness
This Danish prospective cohort study on ESS is one of few studies that gather complete information on a CRS cohort, with data recorded in accordance to EPOS guidelines and results presented separately for the CRSwNP and CRSsNP subgroups.
It is a study characterised by minimised selection bias by evaluating all patients referred for ESS, strict CRS inclusion criteria according to EPOS, insured prior nasal steroid treatment, use of standardised and validated subjective and objective measures, and a 6-month follow-up including clinical examination with a participant rate above 90 %.
The small CRSsNP group size, a relatively short follow-up and lack of subjective olfactory function evaluation by a visual analogue scale were limitations of the study.
Comparison with other studies
The cohort characteristics in terms of gender distribution, mean age, CRSwNP/CRSsNP-distribution, and proportion of smokers are comparable with other European studies [1, 4, 21, 22]. The asthma prevalence for the whole cohort was 24 %, a result in line with a recent Swedish study reporting an asthma prevalence of 26 % [1]. The asthma prevalence in our cohort was unevenly distributed with 28 % in the CRSwNP group, and only 10 % in the CRSsNP group, confirming the known positive association between asthma and CRSwNP [6, 23, 24], but indicating low to no association to CRSsNP in our cohort [23].
The preoperative Lund–Mackay CT score of 15.2 points for the whole cohort is among the highest scores reported in comparable studies [4, 21, 25, 26], and along with the preoperative SNOT-22 score of 43.6 points, it indicates that the CRS disease severity of our cohort is at the same level as the above-mentioned studies.
Two patients from the CRSwNP group had no significant changes in the CT. Both fulfilled the EPOS criteria for CRS based on their symptoms and endoscopic findings, having nasal obstruction, facial pain and reduced olfaction of a duration longer than 12 weeks, and nasal polyposis and edema, primary in the middle meatus and concha media, documented by nasal endoscopy. The preoperative CT scan revealed partial opacification of their maxillary sinuses, scoring only two points on the Lund–Mackay CT scoring system. In the work of Hopkins et al. [4] they showed that a substantial part the chronic rhinosinusitis group underwent surgery in absence of significant changes in Lund–Mackay CT score. Results indicating that a part of CRS patients have their disease primarily in the nasal cavity with only sparse involvement of the sinuses.
The results of the study with postoperative reduction in SNOT-22 score of more than 50 % in both the CRSwNP and CRSsNP groups, are in line with a high international standard [4, 25, 27], and confirms the efficacy of ESS on quality of life improvement for patients with severe CRS.
This study protocol had a limited follow-up length of 6 months, and we recognise that a longer follow-up, e.g. 1 year, would have improved the strengths of this study. General procedure in Denmark is that patients are discontinued from postoperative controls at the hospital after a 3- or 6-month postoperative follow-up, and are advised to consult the private otorhinolaryngologist who referred them for surgery in need of further follow-up. As this study design set out to be representative of the daily clinical practice, it did not enable us to add a 1-year clinical follow-up. However, previous long-term studies have documented that the effects of ESS measured after 3–12 months, are likely to be sustained over a 5-year period [28, 29].
The results from the CRSwNP group indicate that the subjective SNOT-22 score and the change in SNOT-22 score after ESS, is proportional to the objective sino-nasal pathology measured by Lund–Mackay CT score and MLK score in this group. Similar correlation estimates were found between Lund–Kennedy endoscopy score and quality of life changes by Mace et al. [30]. Our study was based on a multi-examiner setup, and although the MLK score was recently shown to have the highest test–retest and inter-rater reliability among three existing scoring systems [17], we recognise that some inter-rater variation may exist.
To our knowledge, this is the first study to show positive correlations between the Lund–Mackay CT score and SNOT-22 results. Most previous studies have shown weak to no association between Lund–Mackay CT score and the tested health-related quality of life measures [20, 31–33]. Although the correlation estimates were all moderate to weak, our data confirm the assumption that the quality of life measures are somewhat proportional to the objective sino-nasal pathology in CRSwNP. However, they also indicate that the sino-nasal pathology may only account for a part of the complete disease burden in CRS.
Olfactory function results showed an overall positive effect of ESS, with a statistically significant improvement of Sniffin’ Sticks score in the CRSwNP group, and a positive tendency in the CRSsNP group. A positive olfactory function result of ESS in CRS patients was also confirmed by a recent Greek study [7].
Interpretation of olfactory function change, using only the Sniffin’ Sticks scores as measurement, is somewhat complex. Small changes (e.g. 1–2 points) may have limited clinical relevance. Therefore, we applied the conservative approach introduced by Pade and Hummel [13], defining change in smell perception as a change in Sniffin’ Sticks of three or more points. Thus, our results showed that the majority of CRS patients have unchanged (CRSwNP 68 %/CRSsNP 66 %) or improved (25 %/24 %) smell perception after ESS. However, there is a small group who experienced a deterioration (7 %/10 %) in olfactory function after surgery. Interestingly but also expectedly, such loss of sense of smell was found most frequently in patients with a relatively high preoperative olfactory score. These results are confirmed by previous studies [13, 21].
We found that the preoperative Sniffin’ Sticks score was negatively correlated to the Lund–Mackay CT score, meaning that patients with high Lund–Mackay CT score had lower olfactory function. This was statistically significant for the CRSwNP group and with the same tendency in the CRSsNP group. A recent European study found that high opacification on CT (defined as Lund–Mackay CT score >7) was associated with larger improvement in Sniffin’ Sticks score after ESS [8]. When analysing our whole cohort as one, we found a positive correlation between the Lund–Mackay CT score and the improvement in Sniffin’ Sticks score 6 months postoperative, a result that could support their findings. Contrary to our expectations, the subgroup analysis showed that this result was primary driven by the tendency in CRSsNP group, while the association was weak in the CRSwNP group.
Conclusion
ESS is an effective treatment for patients with severe CRS, both CRSwNP and CRSsNP, leading to immediate and persistent improvement in quality of life. Smell perception improves in one-fourth of CRS patients after ESS, while for the majority of patients it is unchanged when measured by Sniffin’ Sticks. However, there are some patients who are less likely to benefit from surgery, and unfortunately 7–10 % of the patients may experience deterioration in olfactory function. Thorough consideration before surgical intervention should be given to patients with limited opacification on CT, sparse findings by nasal endoscopy and patients with good olfactory function.
Patients with severe CRSwNP selected for ESS treatment seems to be a well described disease-unit, with consistent epidemiology, reduction in quality of life, and documented effect of ESS across Europe. In patients with severe CRSsNP selected for ESS the disease-unit is less well described. This group is often relatively small in terms of statistical analysis, and cohort characteristics are often overshadowed by merging of data with the CRSwNP group.
This study has shown that the efficacy of ESS in the CRSsNP group is at the same level as for the CRSwNP regarding quality of life improvement and smell perception. Still there is much uncertainty of its association to possible risk factors, other illnesses, and correlations of objective findings to treatment outcomes.
More studies on this subgroup are needed to further uncover this knowledge, important for selection of CRSsNP patients to ESS, and providing them with information of the anticipated outcome of surgery.
References
Sahlstrand-Johnson P, Ohlsson B, Von Buchwald C, Jannert M, Ahlner-Elmqvist M (2011) A multi-centre study on quality of life and absenteeism in patients with CRS referred for endoscopic surgery. Rhinology 49(4):420–428. doi:10.4193/Rhino11.101
Hastan D, Fokkens WJ, Bachert C, Newson RB, Bislimovska J, Bockelbrink A, Bousquet PJ, Brozek G, Bruno A, Dahlen SE, Forsberg B, Gunnbjornsdottir M, Kasper L, Kramer U, Kowalski ML, Lange B, Lundback B, Salagean E, Todo-Bom A, Tomassen P, Toskala E, van Drunen CM, Bousquet J, Zuberbier T, Jarvis D, Burney P (2011) Chronic rhinosinusitis in Europe—an underestimated disease. A GA(2)LEN study. Allergy 66(9):1216–1223. doi:10.1111/j.1398-9995.2011.02646.x
Lange B, Holst R, Thilsing T, Baelum J, Kjeldsen A (2013) Quality of life and associated factors in persons with Chronic Rhinosinusitis in the general population. Clin Otolaryngol Off J ENT-UK Off J Netherlands Soc Oto-Rhino-Laryngol Cervico-Facial Surg. doi:10.1111/coa.12189
Hopkins C, Browne JP, Slack R, Lund V, Topham J, Reeves B, Copley L, Brown P, van der Meulen J (2006) The national comparative audit of surgery for nasal polyposis and chronic rhinosinusitis. Clin Otolaryngol Off J ENT-UK Off J Netherlands Soc Oto-Rhino-Laryngol Cervico-Facial Surg 31(5):390–398. doi:10.1111/j.1749-4486.2006.01275.x
Ragab SM, Lund VJ, Scadding G (2004) Evaluation of the medical and surgical treatment of chronic rhinosinusitis: a prospective, randomised, controlled trial. Laryngoscope 114(5):923–930. doi:10.1097/00005537-200405000-00027
Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alobid I, Baroody F, Cohen N, Cervin A, Douglas R, Gevaert P, Georgalas C, Goossens H, Harvey R, Hellings P, Hopkins C, Jones N, Joos G, Kalogjera L, Kern B, Kowalski M, Price D, Riechelmann H, Schlosser R, Senior B, Thomas M, Toskala E, Voegels R, de Wang Y, Wormald PJ (2012) EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 50(1):1–12. doi:10.4193/Rhino50E2
Katotomichelakis M, Simopoulos E, Tripsianis G, Balatsouras D, Danielides G, Kourousis C, Livaditis M, Danielides V (2014) Predictors of quality of life outcomes in chronic rhinosinusitis after sinus surgery. Euro Arch Oto-Rhino-Laryngol Off J Euro Feder Oto-Rhino-Laryngol Soc (EUFOS): Aff German Soc Oto-Rhino-Laryngol-Head Neck Surg 271(4):733–741. doi:10.1007/s00405-013-2626-6
Minwegen F, Thomas JP, Bernal-Sprekelsen M, Dazert S, Minovi A (2014) Predictive value of disease severity on self-reported rating and quantitative measures of olfactory function outcomes after primary endoscopic sinus surgery. A prospective study. Rhinology 52(4):437–443. doi:10.4193/Rhin14.043
Lange B, Thilsing T, Al-kalemji A, Baelum J, Martinussen T, Kjeldsen A (2011) The Sino-Nasal Outcome Test 22 validated for Danish patients. Dan Med Bull 58(2):A4235
Hopkins C, Gillett S, Slack R, Lund VJ, Browne JP (2009) Psychometric validity of the 22-item Sinonasal Outcome Test. Clin Otolaryngol Off J ENT-UK Off J Netherlands Soc Oto-Rhino-Laryngol Cervico-Facial Surg 34(5):447–454. doi:10.1111/j.1749-4486.2009.01995.x
Browne JP, Hopkins C, Slack R, Cano SJ (2007) The Sino-Nasal Outcome Test (SNOT): can we make it more clinically meaningful? Otolaryngol-Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg 136(5):736–741. doi:10.1016/j.otohns.2007.01.024
Hummel T, Konnerth CG, Rosenheim K, Kobal G (2001) Screening of olfactory function with a four-minute odor identification test: reliability, normative data, and investigations in patients with olfactory loss. Ann Otol Rhinol Laryngol 110(10):976–981
Pade J, Hummel T (2008) Olfactory function following nasal surgery. Laryngoscope 118(7):1260–1264. doi:10.1097/MLG.0b013e318170b5cb
Hummel T, Sekinger B, Wolf SR, Pauli E, Kobal G (1997) ‘Sniffin’ sticks’: olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem Senses 22(1):39–52
Hox V, Bobic S, Callebaux I, Jorissen M, Hellings PW (2010) Nasal obstruction and smell impairment in nasal polyp disease: correlation between objective and subjective parameters. Rhinology 48(4):426–432. doi:10.4193/Rhino10.049
Lund VJ, Kennedy DW (1995) Quantification for staging sinusitis. The Staging and Therapy Group. Ann Otol Rhinol Laryngol Suppl 167:17–21
Psaltis AJ, Li G, Vaezeafshar R, Cho KS, Hwang PH (2014) Modification of the Lund Kennedy endoscopic scoring system improves its reliability and correlation with patient reported outcome measures. Laryngoscope. doi:10.1002/lary.24654
Lund VJ, Kennedy DW (1997) Staging for rhinosinusitis. Otolaryngol-Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg 117(3 Pt 2):S35–S40
Lund VJ, Mackay IS (1993) Staging in rhinosinusitus. Rhinology 31(4):183–184
Hopkins C, Browne JP, Slack R, Lund V, Brown P (2007) The Lund–Mackay staging system for chronic rhinosinusitis: how is it used and what does it predict? Otolaryngol-Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg 137(4):555–561. doi:10.1016/j.otohns.2007.02.004
Briner HR, Jones N, Simmen D (2012) Olfaction after endoscopic sinus surgery: long-term results. Rhinology 50(2):178–184. doi:10.4193/Rhino11.213
Ehnhage A, Olsson P, Kolbeck KG, Skedinger M, Dahlen B, Alenius M, Stjarne P (2009) Functional endoscopic sinus surgery improved asthma symptoms as well as PEFR and olfaction in patients with nasal polyposis. Allergy 64(5):762–769. doi:10.1111/j.1398-9995.2008.01870.x
Jarvis D, Newson R, Lotvall J, Hastan D, Tomassen P, Keil T, Gjomarkaj M, Forsberg B, Gunnbjornsdottir M, Minov J, Brozek G, Dahlen SE, Toskala E, Kowalski ML, Olze H, Howarth P, Kramer U, Baelum J, Loureiro C, Kasper L, Bousquet PJ, Bousquet J, Bachert C, Fokkens W, Burney P (2012) Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy 67(1):91–98. doi:10.1111/j.1398-9995.2011.02709.x
Hakansson K, Thomsen SF, Konge L, Mortensen J, Backer V, von Buchwald C (2014) A comparative and descriptive study of asthma in chronic rhinosinusitis with nasal polyps. Am J Rhinol Allergy 28(5):383–387. doi:10.2500/ajra.2014.28.4076
Kennedy JL, Hubbard MA, Huyett P, Patrie JT, Borish L, Payne SC (2013) Sino-nasal outcome test (SNOT-22): a predictor of postsurgical improvement in patients with chronic sinusitis. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol 111(4):246–251 e242. doi:10.1016/j.anai.2013.06.033
Smith TL, Litvack JR, Hwang PH, Loehrl TA, Mace JC, Fong KJ, James KE (2010) Determinants of outcomes of sinus surgery: a multi-institutional prospective cohort study. Otolaryngol-Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg 142(1):55–63. doi:10.1016/j.otohns.2009.10.009
Abdalla S, Alreefy H, Hopkins C (2012) Prevalence of sinonasal outcome test (SNOT-22) symptoms in patients undergoing surgery for chronic rhinosinusitis in the England and Wales National prospective audit. Clin Otolaryngol Off J ENT-UK Off J Netherlands Soc Oto-Rhino-Laryngol Cervico-Facial Surg 37(4):276–282. doi:10.1111/j.1749-4486.2012.02527.x
Hopkins C, Slack R, Lund V, Brown P, Copley L, Browne J (2009) Long-term outcomes from the English national comparative audit of surgery for nasal polyposis and chronic rhinosinusitis. Laryngoscope 119(12):2459–2465. doi:10.1002/lary.20653
Rudmik L, Mace J, Soler ZM, Smith TL (2014) Long-term utility outcomes in patients undergoing endoscopic sinus surgery. Laryngoscope 124(1):19–23. doi:10.1002/lary.24135
Mace JC, Michael YL, Carlson NE, Litvack JR, Smith TL (2010) Correlations between endoscopy score and quality of life changes after sinus surgery. Arch Otolaryngol-Head Neck Surg 136(4):340–346. doi:10.1001/archoto.2010.34
Wabnitz DA, Nair S, Wormald PJ (2005) Correlation between preoperative symptom scores, quality-of-life questionnaires, and staging with computed tomography in patients with chronic rhinosinusitis. Am J Rhinol 19(1):91–96
Bhattacharyya N (2006) Radiographic stage fails to predict symptom outcomes after endoscopic sinus surgery for chronic rhinosinusitis. Laryngoscope 116(1):18–22. doi:10.1097/01.mlg.0000192284.22703.04
Basu S, Georgalas C, Kumar BN, Desai S (2005) Correlation between symptoms and radiological findings in patients with chronic rhinosinusitis: an evaluation study using the Sinonasal Assessment Questionnaire and Lund–Mackay grading system. Euro Arch Oto-Rhino-Laryngol Off J Euro Feder Oto-Rhino-Laryngol Soc (EUFOS) Aff German Soc Oto-Rhino-Laryngol Head Neck Surg 262(9):751–754. doi:10.1007/s00405-004-0891-0
Conflict of interest
All authors declare that there exists no conflict of interest for this work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lind, H., Joergensen, G., Lange, B. et al. Efficacy of ESS in chronic rhinosinusitis with and without nasal polyposis: a Danish cohort study. Eur Arch Otorhinolaryngol 273, 911–919 (2016). https://doi.org/10.1007/s00405-015-3667-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-015-3667-9