
Abstract
The aim of this study was to evaluate the relationship between the maxillary sinus volumes and the nasal septal deviation angles in patients with antrochoanal polyps (ACP). 76 patients who underwent ACP surgery were included in the study. Of those 36 patients who had multislice computed tomography (MSCT) were evaluated to calculate maxillary sinus volume. The records of paranasal MSCT of 36 healthy people without any paranasal sinus diseases or surgery constituted age- and gender-matched healthy controls. Maxillary sinüs volumes and septal deviation angles were calculated using the paranasal MSCT volume-rendering technique. Thirty-six patients in the ACP group were compared with 36 polyp side-matched healthy people. The mean age was 16.6 ± 6.7 years in both groups. Statistically, the mean value of the maxillary sinus volume was significantly higher in the ACP group compared with the ACP side-matched control group (15.1 ± 4.6 versus 12.0 ± 3.5 mm3) (p = 0.002). Furthermore, the mean value of the maxillary sinus volume in the non-polyp side (14.2 ± 4.7 mm3) was statistically higher in the ACP group compared with the side-matched control group volume (11.9 ± 3.8 mm3) (p = 0.024). In addition, Fifty-three of 76 ACP patients had septal deviation. While the septal deviation was on the same side with the ACP in 17 patients, it was on the opposite side in 36 patients. In conclusion, the maxillary sinus volumes increased in ACP patients compared with the healthy control group. Many patients had nasal septal deviation on the opposite side of the ACP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Antrochoanal polyps (ACPs) are benign polypoid lesions that originate in the maxillary sinus and extend into the choana passing through the natural or accessory ostium [1]. They represent approximately 4–6 % of all nasal polyps in the general population and occur most commonly in children and young adults [2, 3]. Furthermore, they rarely originate in the ethmoid sinus, sphenoid sinus, middle turbinate, inferior turbinate, and hard and soft palates [4]. Although some bilateral ACP cases have been reported in the literature, ACP is almost always unilateral [4, 5].
Several mechanisms, such as allergy, chronic inflammation, vasomotor imbalance, the Bernoulli phenomenon, aspirin intolerance, epithelial rupture, cystic fibrosis, and infections have been proposed to explain the etiology of nasal polyps [6]. The most commonly accepted hypothesis is an intramural cyst originating from the maxillary sinus [5, 7]. However, the etiology of ACP is still unknown, and limited studies have been found in the literature.
The aim of this study was to evaluate the relationship between the maxillary sinus volume and septal deviation with ACP etiology.
Materials and methods
Permission of the Local Ethical Committee was obtained. The patient whom were operated due to ACP in our clinic included into study as a ACP group. The records of preoperatively taken paranasal computed tomography of 76 ACP patients were collected retrospectively between 2008 and 2014 at the Radiology Department. 36 patients had thin-slice paranasal CT and 40 patients had no thin-slide paranasal CT in radiology archive. Thin-slice paranasal CT of 36 age- and gender-matched patients without ACP were collected as the control group. The patients without paranasal CT or having maxillofacial trauma, severe chronic sinusitis, or paranasal and/or nasal surgery were excluded from the study. All ACP patients operated via endoscopic approach.
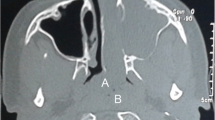
Maxillary sinus volume were calculated from 36 ACP patients and 36 control patients with thin-slice paranasal CT. Multislice computed tomography (MSCT, Philips Brilliance ICT 64; Netherlands, scan setting, 120 kV, 150 mAs), the scan field of view (FOV) was 250 mm (collimation: 64 × 0.625), and an image matrix of 512 × 512 was used. After scanning, the images were reconstructed, and the volumes of the maxillary sinuses were automatically calculated using a volume-rendering technique (VRT) on a workstation (Extended Brilliance Workspace, Philips Medical Systems) (Fig. 1). We calculated the volumes of both sides of the maxillary sinus of all ACP patients and the control group. The maxillary sinus volumes were calculated as mm3. The angle between the linear line drawn from the maxillary spine to the crista galli and the linear line drawn from the crista galli to the most deviated part of the nasal septum was accepted as a deviation angle (Fig. 2). The direction of deviation was described by the convexity of the septal curvature. The patients were divided into three groups according to the measured angle of nasal septal deviation as: mild (<9), moderate (9–15), or severe (15 and up) according to the grading system described by Elahi et al. [8]

The measurement of the maxillary sinus volume on the ACP side and the opposite side with marking in the axial, coronal, and sagittal planes and 3D reconstruction of the right maxillary sinus volume in the same patient

The angle between the linear line drawn from the maxillary spine to the crista galli and the linear line drawn from the crista galli to the most deviated part of the nasal septum
The mean volume of the right maxillary sinus in right ACP patients in the ACP group was matched with the mean volume of the right maxillary sinus of healthy patients in the control group. Correspondingly, the mean volume of the left maxillary sinus in left ACP patients in the study group was matched with the mean volume of the left maxillary sinus of healthy patients in the control group. In addition, the volume of the maxillary sinus on the opposite side of the ACP was compared with side-matched patients in the control group.
The mean, standard deviation, the lowest and the highest median, rate, and frequency were used as descriptive statistics of data. The distribution of variabilities was controlled by the Kolmogorov–Simirnov test. The independent-samples t test and the paired-sample t test were applied in the analysis of quantitative data and repetitive measurements, respectively. The correlations were evaluated with Pearson correlation analysis, and the Kappa test was also applied for the adjustment. The SPSS 21.0 program was used in the analysis.
Results
A total of 76 patients with ACPs were included in this study, and 36 of them were female (F/M: 36/40). The mean age was 16.6 ± 6.7 (9–35 years). ACPs were on the right side in 37 patients.
Mean maxillary volume of 36 ACP patients whom had thin-slice computed tomography were calculated. While the mean maxillary sinus volume on the polyp side was 15.1 ± 4.6 mm3 in ACP patients, it was 12 ± 3.5 mm3 in the side-matched control group. The mean maxillary sinus volume in ACP patients was significantly higher than those in the control group (p = 0.002). The mean maxillary sinus volume (14.2 ± 4.7 mm3) on the opposite site of the ACP was significantly higher than the mean maxillary sinus volume of the side-matched control group (11.9 ± 3.8 mm3) (p = 0.024). Both side of the mean maxillary sinus volumes were not statistically significant in ACP group (p = 0.947). However, the mean maxillary sinus volumes between the side-matched polyp side and the opposite side were not statistically significant in control group (p = 0.157) (Table 1; Fig. 3).

Box and whisker plot showing the distribution of maxillary volume in the control and ACP groups. Central box rule median; lower and upper box borders first and third quartiles, respectively; whiskers 95 % confidence interval; circles outliers
There were 22 patients with ACP age 13 year or more. While the mean maxillary sinus volume was 16.7 ± 5 mm3 in patients with ACP age 13 years or more, it was 13.5 ± 3.7 mm3 in the polyp-matched side in the control group. The mean maxillary sinus volume in patients with ACP was found to be statistically higher than side-matched patients in the control group (p = 0.042). Although the mean maxillary sinus volume on the non-polyp side in ACP patients was higher (16.5 ± 4.7 mm3) than in the side-matched control group (13.5 ± 4 mm3), no statistically significant difference was found (Table 2).
Fifty-three of 76 ACP patients (69 %) had deviation more than “zero” degree. 15 patients had mild deviation, 27 patients has moderate deviation, 11 patients had severe deviation. While ACPs and septal deviations were on the same side in 32.1 % (17 patients) of cases, they were on the opposite side in 67.9 % of cases (36 patients). There was a negative directional agreement between the septal deviation side and ACP side (p = 0.010, Kappa = −0.346). The mean angle of septal deviation was 10.8° ± 4.4° (5–18), with the median value was 11°.
The deviation side and maxillary sinus volume were compared in 36 ACP patients whose had thin-slice computed tomography. The mean maxillary sinus volume in patients whose ACPs were on the same side of the deviation was 15.1 ± 4.7 mm3 (7.6–25.3 mm3), and it was 15.9 ± 4.5 mm3 (6.5–27.6 mm3) in patients whose ACPs were on the opposite of the deviation. There was no statistically significant difference in maxillary sinus volumes between the septal deviation side and the opposite side in patients with ACPs (p = 0.647). Furthermore, in patients whose ACPs were on the deviation side, there was no statistically significant difference between the polyp side (15.1 ± 4.7 mm3) and the non-polyp side (15.3 ± 5.4 mm3) mean maxillary sinus volumes (p = 0.832). In patients whose ACPs were on the opposite side of the septal deviation, there was no significant difference between the polyp side (15.9 ± 4.5 mm3) and the non-polyp side mean maxillary sinus volume (14.6 ± 4.3 mm3) (p = 0.133) (Table 3).
The relationship between the maxillary sinus volume and the nasal septal deviation grade was evaluated in two groups: ACP ipsilateral to the deviation and ACP contralateral to the deviation. There was no statistically significant correlation between the two groups regarding their maxillary sinus volumes and nasal septal deviation angles (p > 0.05) (Table 4)
Discussion
ACP is composed of a cystic part filling the maxillary sinus and a solid part emerging from the maxillary sinus ostium and extending into the choana [7]. The pathogenesis of ACP is unknown, and its etiology is still unclear. The most wondering issue is about the ACP, while almost all ACPs are unilateral, nasal polyps are bilateral. For this reason, many studies comparing ACPs and bilateral nasal polyposis have been performed to enlighten the etiology of ACPs [9, 10].
Topal et al. [9] found that matrix metalloproteinases (MMP-9) were higher in patients with ACP and nasal polyps compared with the normal nasal mucosa. Min et al. [10] suggested that inflammatory cells and eosinophils were lower in ACP patients than in those with nasal polyposis. Some studies have claimed that ACP could develop from an intramural cyst in the maxillary sinus. Berg et al. [7] reported that there was no histological difference between an intramural cyst and ACP, as the fluid aspirated from the cyst and ACP had the same histology. Chen et al. [11] hypothesized that the development of cystic part of ACP could be caused by aciner mucous gland obstruction during the recovery period of chronic sinusitis. Mahfouz et al. [12] found that the fibroblast growth factor—basic (FGF-b) and that the transforming growth factor beta (TGF-β) levels were higher in ACP patients than in patients with chronic sinusitis or normal healthy nasal mucosa. Sunagawa et al. [13] reported that urokinase-type plasminogen activator (uPA) and inhibitor (uPAI) plays a part in the pathogenesis of ACP. Jang et al. [14] stated that the arachidonic acid metabolites has a role in the pathogenesis of ACP. Cook and Chen [11, 15] reported that allergic diseases could be involved in the etiology of ACP.
In our series, the mean maxillary sinus volume on the ACP side was significantly higher than those in side-matched control patients. Considering only this data, one might think that the maxillary sinus volume could be increased with the effect of ACP. We also compared the mean maxillary sinus volumes between the non-polyp side of patients with ACP and side-matched control group. Statistically, we found that the maxillary sinus volumes were even higher on the non-polyp side in patients with ACP. Therefore, ACP itself did not increase the volume of maxillary sinus, as ACP patients had already higher bilateral maxillary sinus volumes.
The maxillary sinus volume increases rapidly with age until 12 years, and then it slowes down untill early adulthood [16]. As the maxillary sinus volume varies with age, we also analyzed the patients over 13 years of age again to obtain accurate results. We found that the maxillary sinus volumes were higher in ACP patients than in the side-matched control group for patients over 13 years of age. The increased volume on the polyp side was statistically significant. Although the maxillary sinus volumes on the non-polyp side of ACP patients were higher than in the side-matched control group, the difference was not statistically significant. This results again showed that the maxillary sinus volumes were higher in ACP patients than in the control group.
Some studies have revealed the variability of maxillary sinus volumes with nasal septal deviation [17, 18]. Maxillary sinus volumes on the opposite site of the deviation were found to be larger [17, 18]. In our study, increased volumes of maxillary sinuses in ACP patients were thought to confuse us that it could be related to septal deviation. Therefore, we compared the maxillary sinus volumes of ACP patients on the ipsilateral and contralateral side to the deviation and found no statistically significant difference among them. These data showed that increased volumes of maxillary sinuses were not associated with the nasal septal deviation.
Frosini et al. [5] stated that 55 % of patients had septal deviation in their study consisting of 200 cases. Frosini et al. did not comment on the relationship between septal deviation side and its grade or angle. In our study, additionally, we calculated the deviation angles objectively with the help of MSCT. 15 patients had mild deviation, 27 patients have moderate deviation, 11 patients had severe deviation. While ACPs and septal deviations were on the same side in 32.1 % (17 patients) of cases, they were on the opposite side in 67.9 % of cases (36 patients). Furthermore, Frosini et al. claimed that intramural cyst herniated into the nasal cavity from the maxillary sinus due to increased nasal airflow caused by the Bernoulli principle and anatomical disturbances in the nasal cavity. Frosini et al. also reported that inferior turbinate hypertrophy and concha bullosa were frequent in ACP patients. We know that compensatory hypertrophy of the inferior turbinate occured on the opposite side of the deviation [18]. Considering the same mechanism, ACP could develop on the opposite side of the deviation to compensate.
Although ACP was usually found unilaterally, the volumes of maxillary sinuses increased on both side of the nasal cavity in our study. Besides, the reason why ACP was mostly unilateral could be related to that, statistically ACP was found on the contralateral side of the nasal septal deviation. Further investigations about the evaluation of the nasal air flow will be required to enlighten the above-mentioned issues.
Among the limitations of our study, we only measured the nasal air flow with its relation to nasal septal deviation regardless of the evaluation of the nasal turbinates. Furthermore, the nasal air flow resistance could be evaluated with acoustic rhinomanometer in patients with ACP. The results of patients with ACP could be compared with patients with bilateral nasal poliposis. Further prospective studies are required to cover all these limitations in future.
Conclusion
The maxillary sinus volumes increased in ACP patients compared with the healthy control group. Many patients had nasal septal deviation on the opposite side of ACP. Further studies should be required to understand the mechanism of ACP.
References
Hong SK, Min YG, Kim CN, Byun SW (2001) Endoscopic removal of the antral portion of antrochoanal polyp by powered instrumentation. Laryngoscope 111(10):1774–1778
We Heck, Oe Hallberg, Hl Williams (1950) Antrochoanal polyp. AMA Arch Otolaryngol 52(4):538–548
Lee TJ, Huang SF (2006) Endoscopic sinus surgery for antrochoanal polyps in children. Otolaryngol Head Neck Surg 135(5):688–692
Yaman H, Yilmaz S, Karali E, Guclu E, Ozturk O (2010) Evaluation and management of antrochoanal polyps. Clin Exp Otorhinolaryngol 3(2):110–114. doi:10.3342/ceo.2010.3.2.110
Frosini P, Picarella G, De Campora E (2009) Antrochoanal polyp: analysis of 200 cases. Acta Otorhinolaryngol Ital 29(1):21–26
Guven M, Karabay O, Akidil O, Yilmaz MS, Yildirim M (2013) Detection of staphylococcal exotoxins in antrochoanal polyps and chronic rhinosinusitis with nasal polyps. Otolaryngol Head Neck Surg 148(2):302–307. doi:10.1177/0194599812465586 (Epub 2012 Oct 30)
Berg O, Carenfelt C, Silfverswärd C, Sobin A (1988) Origin of the choanal polyp. Arch Otolaryngol Head Neck Surg 114(11):1270–1271
Elahi MM, Frenkiel S, Fageeh N (1997) Paraseptal structural changes and chronic sinus disease in relation to the deviated septum. J Otolaryngol 26:236–240
Topal O, Erbek SS, Kiyici H, Cakmak O (2008) Expression of metalloproteinases MMP-2 and MMP-9 in antrochoanal polyps. Am J Rhinol 22(4):339–342. doi:10.2500/ajr.2008.22.3183
Min YG, Chung JW, Shin JS, Chi JG (1995) Histologic structure of antrochoanal polyps. Acta Otolaryngol 115(4):543–547
Chen JM, Schloss MD, Azouz ME (1989) Antro-choanal polyp: a 10-year retrospective study in the pediatric population with a review of the literature. J Otolaryngol 18(4):168–172 (Review)
Mahfouz ME, Elsheikh MN, Ghoname NF (2006) Molecular profile of the antrochoanal polyp: up-regulation of basic fibroblast growth factor and transforming growth factor beta in maxillary sinus mucosa. Am J Rhinol 20(4):466–470
Sunagawa M, Kinjoh K, Nakamura M, Kosugi T (1999) Urokinase-type plasminogen activator and plasminogen activator inhibitor antigen in tissue extracts of paranasal sinus mucous membranes affected by chronic sinusitis and antrochoanal polyps. Eur Arch Otorhinolaryngol 256(5):237–241
Jang YJ, Rhee CK, Oh CH, Ryoo HG, Kim HG, Ha M (2000) Arachidonic acid metabolites in antrochoanal polyp and nasal polyp associated with chronic paranasal sinusitis. Acta Otolaryngol 120(4):531–534
Cook PR, Davis WE, McDonald R, McKinsey JP (1993) Antrochoanal polyposis: a review of 33 cases. Ear Nose Throat J 72(6):401–402 (404–410)
Lawson W, Patel ZM, Lin FY (2008) The development and pathologic processes that influence maxillary sinus pneumatization. Anat Rec 291:1554–1563
Kapusuz Gencer Z, Ozkiris M, Okur A, Karacavus S, Saydam L (2013) The effect of nasal septal deviation on maxillary sinus volumes and development of maxillary sinusitis. Eur Arch Otorhinolaryngol 270(12):3069–3073. doi:10.1007/s00405-013-2435-y (Epub 2013 Mar 20)
Orhan I, Ormeci T, Aydin S, Altin G, Urger E, Soylu E, Yilmaz F (2014) Morphometric analysis of the maxillary sinus in patients with nasal septum deviation. Eur Arch Otorhinolaryngol 271(4):727–732. doi:10.1007/s00405-013-2617-7
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Aydın, S., Taskin, U., Orhan, I. et al. The analysis of the maxillary sinus volumes and the nasal septal deviation in patients with antrochoanal polyps. Eur Arch Otorhinolaryngol 272, 3347–3352 (2015). https://doi.org/10.1007/s00405-014-3460-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-014-3460-1