
Abstract
The g-ratio (estimated by dividing the axon diameter by the myelinated fiber diameter) can be useful to the evaluation of the relationship between nerve conduction velocity and fiber morphology during peripheral nerve regeneration. However, there is little detailed information about the g-ratio of the human recurrent laryngeal nerve (RLN), especially between men and women. The objective of this study was to investigate the g-ratio of the RLN by quantifying histomorphometric data (axon diameter and myelinated fiber diameter) in the RLN of men and women. The RLN was bilaterally studied in human specimens obtained from necropsies (seven men and seven women). The nerves were analyzed using histology, and the morphometric parameters were measured using Image Pro-Plus Software (Image Pro-Plus 6.0; Media Cybernetics, Silver Spring, MD, USA). When compared with the RLN of the women, the parameters of the RLN of the men are significantly larger, as shown by the axon diameter (19.0 %) (P = 0.0001), myelinated fiber diameter (7.1 %) (P = 0.0497), and g-ratio (12.5 %) (P = 0.0005). Our findings demonstrated that there are morphological asymmetries between the g-ratio (degree of the myelination) of the masculine and feminine RLN. These morphological findings are probably related to physiological differences.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The g-ratio (estimated by dividing the axon diameter by the myelinated fiber diameter) [1] is widely utilized as a functional and structural index of optimal axonal myelination. This concept is supported by the observations that during the recovery process from demyelinating disease, central axons undergo an initial period of hyper-remyelination and increased diameters which then eventually revert to the normal g-ratio [2].
In addition, the g-ratio can be useful to the evaluation of the relationship between nerve conduction velocity and fiber morphology during peripheral nerve regeneration [3]. Likewise, countless studies [4, 5] have used the g-ratio as an important parameter for the evaluation of the degree of myelination of the peripheral nerve fibers in studies in the area of microsurgery [6].
Thus, this knowledge could be essential to understanding some important aspects of laryngeal reinnervation (anastomosis techniques), as well as for the physiological understanding of the nerves involved in vocal control. In addition, the most frequent cause of vocal fold paralysis is injury to the recurrent laryngeal nerve (RLN) [7], which can also be reinnervated using anastomosis techniques. This technique provides positive effects on vocal fold paralysis in terms of acoustic, perceptual, electromyographic, and visual outcomes [8].
Given that the success of these reinnervation techniques also depends greatly on understanding the microscopic anatomy of the RLN [9], the data on the g-ratio of the RLN are certainly very important for understanding and improving the techniques used for vocal fold reinnervation. However, there is little detailed information on the g-ratio of the human RLN, especially between men and women.
Thus, the aim of this study was to investigate the g-ratio of the RLN by quantifying histomorphometric data (axon diameter and myelinated fiber diameter) in the RLN of men and women.
Materials and methods
Human tissue
The Research Ethics Committee of our institution approved this research project, under number 17547. All the nerves analyzed were obtained from necropsies of 14 Caucasian subjects who had died suddenly (seven men [age = 71.14 ± 8.07] and seven women [age = 75.71 ± 7.83]) (mean ± standard deviation), from the Department of Forensic Medicine.
Tissue collection
The dissection of the RLN extended deeply toward the point where it entered the larynx (cricothyroid joint). The segments (~10 mm) of RLN used in our histological analysis were obtained 1 cm below the cricothyroid joint, bilaterally. The same procedure was used in a previous study [10].
Histomorphometric analysis
Digitized images of the nerves were obtained using an Olympus BX 50 microscope (4×, 10× and 100×) (Olympus, Japan) coupled to a video camera (Leica DC 300F) interfaced by Leica Image 50 (IM50) software. The images obtained were measured using Image Pro-Plus Software (Image Pro-Plus 6.0; Media Cybernetics, Silver Spring, MD, USA) (IPP 6.0).
Histological and morphometric measurements of the RLN
Based on previous studies [11], the specimens of the RLN were fixed by immersion for 24 h in a modified Karnovsky solution (Sigma Chemical Company, St. Louis, MO, USA). Next, they were bathed in 0.05 mol/L of sodium cacodylate solution, postfixed in 1 % osmium tetroxide (Sigma Chemical Company) for 2 h, dehydrated in an increasing graded series of acetone (Electron Microscopy Sciences, Hatfield, PA, USA), and embedded in epoxy resin (araldite, durcupan; Fluka, Buchs, Switzerland) which was then polymerized at 60 °C. Three semithin cross-sections (1 μm) were obtained using an ultramicrotome (MT 6000-XL; RMC, Tucson, AZ, USA) with intervals of 100 μm and stained with 1 % toluidine blue (Merck, Darmstadt, Germany) in 1 % sodium tetraborate (Ecibra, Curitiba, Brazil).
According to previous protocol [4, 9] of planar morphometry, the axon diameter (μm) and myelinated fiber diameter (μm) were estimated using the measurement tools of the IPP 6.0. The g-ratio (degree of myelination) was calculated by measuring the diameter of axons and dividing by the total diameter of that axon plus the surrounding myelin sheath (myelinated fiber diameter).
Statistical analysis
The statistical analyses were carried out using an independent samples t test (P < 0.05), to compare the different parameters in men and women. All statistical analyses were performed using GraphPad Prism 5.0 software (Graphpad Software, Inc., USA).
Results
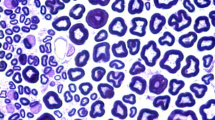
With the use of toluidine blue staining, the measured fibers were seen to have well-defined boundaries. Analysis using toluidine blue staining showed the fibers were well preserved in all specimens and their number was not altered by postmortem dimensional changes (Fig. 1a–d).

Digitized images of the sections of the recurrent laryngeal nerve (RLN) between men (a) and women (c). Higher magnification of the endoneural space of the nerves represented in a and c are shown in b and d, respectively. Note the evident differences in terms of axon diameter. AD axon diameter, FD myelinated fiber diameter, AT adipose tissue, CF collagen fibrils, * axon, + myelin sheath thickness (toluidine blue stain)
The comparison of the morphometric measurements of RLN between men and women shows that, when compared with the RLN of women, the parameters of RLN of men are significantly larger, as shown by the axon diameter (19.0 %), myelinated fiber diameter (7.1 %), and g-ratio (12.5 %) (shown in Table 1) and will be discussed in the next section.
Discussion
The main result found in our study were the smaller g-ratio values of RLN of the women (g-ratio = 0.56). On the other hand, the mean value of the g-ratio was higher in the masculine RLN (g-ratio = 0.64). A lower g-ratio, however, was indicating a higher myelin to axon diameter ratio. This fact is very important as it shows that although the RLN fibers of this sex have a smaller axon diameter, they exhibit a greater degree of the myelination.
These data, at least partially, appear to be consistent with recent descriptions [9] about the g-ratio of the human RLN, especially to the masculine RLN (g-ratio = 0.67); however, this study does not make the comparison between the g-ratio of masculine and feminine RLN.
Recently, an interesting study [2] gathered extensive data about the g-ratio of nerve fibers of different regions of the central nervous system (corpus callosum, spinal cord, optic nerve, superior cerebellar peduncle, anterior commissure, internal capsule, brainstem [g-ratio = 0.72–0.81]) and peripheral (sciatic, sural, saphenous, hypoglossal, facial, splanchnic, vagal, glossopharyngeal, oculomotor, tibial, trochlear, phrenic [g-ratio = 0.47–0.80]). Given these results, and the values shown by our study, it can be assumed that the g-ratio of the RLN (masculine and feminine) shows values similar to other peripheral nerves.
It is known that some peripheral axon g-ratio values tend to be lower than central axon g-ratio values [12]. It is possible that in the peripheral system the space constraint is less of a limiting factor than in the brain, as axonal myelination in the peripheral nervous system tends to be optimized for maximizing conduction velocity so that long projection axons can ensure rapid sensory and motor responses [2]. Thus, the g-ratio may be considered a reflection of the set-point at which the structural and functional organization of individual fibers has achieved a high degree of balance and optimization.
Most myelinated axons in any given animal have the same g-ratio and this value is usually between 0.6 and 0.7. This means that the thickness of the myelin sheath varies according to the diameter of the axon: bigger axons have thicker myelin, and vice versa. The exception to the constant g-ratio rule is seen in axons that have been remyelinated—for example, after peripheral damage and regeneration—in which the sheaths are typically thinner than expected [13].
Rushton was the first to derive an optimal theoretical g-ratio of 0.6. In this classic study, the calculation of g-ratio is based on the speed of fiber conduction [2].
The importance of the axonal diameter for nerve impulse conduction has been classically demonstrated in several studies [14–16] because the conduction velocity is related to the fiber axonal diameter, and increases in these parameters are responsible for increases in the velocity of impulse conduction.
This aspect is of great importance because of the fact that any sexual dimorphism would presumably alter nerve conduction velocity and the electrical signal would cause differences in the firing frequency of the thyroarytenoid muscle fibers and consequently in the rate at which the vocal folds open and close, known as the glottal pulse rate [17].
Although our results show a higher degree of myelination in feminine RLN, our study has provided morphologic evidence to show that the male RLN probably confers a higher electrical conduction rate when compared with that of the females and this can increase the glottal pulse rate in men. Indeed, studies [18] indicate that the glottal pulse rate of the men tends to increase with advancing age, with an evident increase among men between the fifth and eighth decades of life.
This is due to the fact that the axonal diameter and myelinated fiber diameter were larger in men, indicating that men can present a higher conduction velocity in relation to women. Thus, it would seem to be the case that the peripheral nervous structures of men and women may follow slightly different paths to achieve similar levels of function.
Currently, there are no human studies in the literature showing comparative data between the g-ratio of the masculine and feminine RLN. Thus, we believe there is insufficient knowledge about the organization of the g-ratio in the nerve studied here, especially between men and women. In this context, the present study also provides morphometric data on the RLN, which may be essential for understanding and improving the techniques used for vocal fold reinnervation, given that the success of these reinnervation techniques also depends greatly on understanding the histological organization of the RLN [9], and of the skills of any head and neck surgeon with experience in neurorrhaphy [19].
Furthermore, injuries to the RLN, both arising from accidental trauma or surgical procedures, can lead to unilateral or bilateral paralysis of the vocal folds and result in changes in voice, dysphagia and dyspnea [20, 21]; as well as vocal fold paralysis caused by schwannoma in RLN [22]. Therefore, this study shall be important for clinicians, surgeons, and academicians who handle this particular anatomical site.
Previous investigations have shown that the aging process can cause different morphological changes, including a small reduction in fiber density in the RLN [23]. The g-ratio is a morphological parameter that is not deeply associated to small reductions in fiber density and to our knowledge no change in g-ratio are observed during aging. Thus, it is improbable that the aging process will generate significant changes in RLN g-Ratio. Another important point to support the reliability of our results is that, although only older subjects have been used in our study, these subjects belong to the same age group.
We believe that it is improbable, but possible, that future studies could show differences between g-Ratio in different ages, however, at this moment, it is important to consider the difficulty of obtaining specimens from a younger age group (e.g., 20–30 years). Other researchers found the same problem, for example, a previous study into the morphological parameters of laryngeal muscles was performed using subjects with an average age of 70 years for men and 75 years for women [24].
In addition, we emphasize that though our morphological investigation provides innovative and reliable results about the degree of the myelination of the RLN between men and women, it represents the bilateral analysis of only 14 subjects. Thus, we suggest that future studies with larger numbers of subjects will be needed to definitively confirm our findings.
Conclusions
More than a simple morphologic investigation of the RLN, our findings demonstrated that there are morphological asymmetries between the g-ratio (degree of the myelination) of the RLN masculine or feminine. These morphological findings are probably related to physiological differences. Moreover, our results provide baseline normal values for future studies aimed at further elucidating the functional and morphological patterns of the RLN.
References
Naoki K, Masahito M, Masakazu K, Gerald JA, David MF, Takahiko F, Hiromi O, Masato O (2013) Critical role of p38 MAPK for regeneration of the sciatic nerve following crush injury in vivo. J Neuroinflam 10:1. doi:10.1186/1742-2094-10-1
Chomiak T, Hu B (2009) What is the optimal value of the g-ratio for myelinated fibers in the rat CNS? A theoretical approach. PLoS One 4:e7754
Ikeda M, Oka Y (2012) The relationship between nerve conduction velocity and fiber morphology during peripheral nerve regeneration. Brain Behav 2:382–390
Ilha J, Araujo RT, Malysz T, Hermel EE, Rigon P, Xavier LL, Achaval M (2008) Endurance and resistance exercise training programs elicit specific effects on sciatic nerve regeneration after experimental traumatic lesion in rats. Neurorehabil Neural Repair 22:355–366
Kim PD, Hayes A, Amin F, Akelina Y, Hays AP, Rosenwasser MP (2010) Collagen nerve protector in rat sciatic nerve repair: a morphometric and histological analysis. Microsurgery 30:392–396
Isaacs J, Friebe I, Mallu S, Bachman K (2011) Neurotrophic effects of perfluorocarbon emulsion gel: a pilot study. J Brachial Plex Peripher Nerve Inj 6:11. doi:10.1186/1749-7221-6-11
Crumley RL (1994) Unilateral recurrent laryngeal nerve paralysis. J Voice 8:79–83
Aynehchi BB, McCoul ED, Sundaram K (2010) Systematic review of laryngeal reinnervation techniques. Otolaryngol Head Neck Surg 143:749–759
De Campos D, Do Nascimento PS, Ellwanger JH, Gehlen G, Rodrigues MF, Jotz GP, Xavier LL (2012) Histological organization is similar in human vocal muscle and tongue—a study of muscles and nerves. J Voice 26(811):e19–e26
Jotz GP, de Campos D, Rodrigues MF, Xavier LL (2011) Histological asymmetry of the human recurrent laryngeal nerve. J Voice 25:8–14
Tiago RS, Pontes PA, Brasil OO (2008) Quantitative analysis of myelinic fibers in human laryngeal nerves according to age. Braz J Otorhinolaryngol 74:45–52
Chau WK, So KF, Tay D, Dockery P (2000) A morphometric study of optic axons regenerated in a sciatic nerve graft of adult rats. Restor Neurol Neurosci 16:105–116
Sherman DL, Brophy PJ (2005) Mechanisms of axon ensheathment and myelin growth. Nat Rev Neurosci 6:683–690
Goldman L, Albus JS (1968) Computation of impulse conduction in myelinated fibers; theoretical basis of the velocity-diameter relation. Biophys J 8:596–607
Schlaepfer WW, Myers FK (1973) Relationship of myelin internode elongation and growth in the rat sural nerve. J Comp Neurol 147:255–266
Waxman SG (1980) Determinants of conduction velocity in myelinated nerve fibers. Muscle Nerve 3:141–150
Smith DR, Patterson RD (2005) The interaction of glottal-pulse rate and vocal-tract length in judgements of speaker size, sex, and age. J Acoust Soc Am 118:3177–3186
Harnsberger JD, Shirivastav R, Brown WS Jr, Rothman H, Hollien H (2008) Speaking rate and fundamental frequency as speech cues to perceived age. J Voice 22:58–69
Paniello RC (2000) Laryngeal reinnervation with the hypoglossal nerve: II clinical evaluation and early patient experience. Laryngoscope 110:739–748
Khan A, Pearlman RC, Bianchi DA, Hauck KW (1997) Experience with two types of electromyography monitoring electrodes during thyroid surgery. Am J Otolaryngol 18:99–102
Endo K, Okabe Y, Maruyama Y, Tsukatani T, Furukawa M (2007) Bilateral vocal cord paralysis caused by laryngeal mask airway. Am J Otolaryngol 28:126–129
Liu HL, Yu SY, Li GK, Wei WI (2011) Extracranial head and neck Schwannomas: a study of the nerve of origin. Eur Arch Otorhinolaryngol 268:1343–1347
Nakai T, Goto N, Moriyama H, Shiraishi N, Nonakan N (2000) The human recurrent laryngeal nerve during the aging process. Okajimas Folia Anat Jpn 76:363–367
Happak W, Zrunek M, Pechmann U, Streinzer W (1989) Comparative histochemistry of human and sheep laryngeal muscles. Acta Otolaryngol 107:283–288
Acknowledgments
This study was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
de Campos, D., Heck, L., Jotz, G.P. et al. Degree of myelination (g-ratio) of the human recurrent laryngeal nerve. Eur Arch Otorhinolaryngol 271, 1277–1281 (2014). https://doi.org/10.1007/s00405-013-2690-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-013-2690-y