
Abstract
The objectives of this study were to ascertain the feasibility of transcanal endoscopic underlay myringoplasty using temporalis fascia and compare the results with microscopic myringoplasty. This prospective randomized trial included 60 patients with mucosal chronic otitis media with tympanic membrane perforations of all sizes and locations apart from posteriorly based small or moderate sized perforations. In the endoscopy group, 30 patients underwent exclusive transcanal myringoplasty using tympanomeatal flap elevation with underlay graft placement. In the microscopy group, 30 patients underwent myringoplasty using the postaural approach. Intra-operative variables compared were canalplasty and canal wall curettage for assessment of ossicular status. Graft uptake, hearing outcomes using pure tone audiometry and subjective cosmetic outcomes were assessed 24 weeks post-operatively and compared in the two groups. Resident feedback on the feasibility of endoscopic myringoplasty was obtained using a questionnaire. In the microscopy group, 5/30 patients required canalplasty due to canal overhangs and 4/30 required canal wall curettage for ossicular assessment, whereas none of the patients in the endoscopy group required these procedures. A graft uptake rate of 83.3 % was observed in both groups post-operatively after 24 weeks. Mean air-bone gap pre- and post-operatively in the endoscopy group was 28.5 and 18.13 dB, respectively, whereas these values were 32.4 and 16.9 dB, respectively, in the microscopy group. Subjective cosmetic outcomes were better in the endoscopy group. Resident feedback on endoscopic myringoplasty was positive. Endoscopic myringoplasty appears to be an effective alternative to microscopic myringoplasty and results in excellent hearing with good cosmetic outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The closure of tympanic membrane perforations by myringoplasty is one of the most common surgical procedures performed in an otolaryngology practice. Resident training in otology often begins with tympanoplasty procedures with temporalis fascia as the usual graft material, traditionally performed and taught using an operating microscope, as with most other otological procedures.
Endoscopy has had an increasing role to play in ear surgery, namely, photo documentation of the tympanic membrane [1], cholesteatoma surgery [2–6], surgery of the facial nerve [7] and anatomy of the sinus tympani [8]. Despite the increasing number of publications on the role of endoscopy in the management of otitis media surgery, there has been a scarcity of publications on endoscopic myringoplasty [9–14], with most relying on graft placement without tympanomeatal flap elevation [9–11] in small to medium perforations. There have been very few studies involving direct comparison between endoscopic and microscopic myringoplasty using flap elevation techniques [13, 14].
The effects of incision type in tympanoplasty on cosmesis [15] and the presence of bony canal overhangs necessitating canalplasty [16, 17] have prompted the use of exclusive endoscopic transcanal tympanoplasty in the management of tympanic membrane perforations of different sizes and locations.
The current study was undertaken to compare the microscopic and endoscopic methods of type 1 tympanoplasty directly using temporalis fascia in an underlay placement method. Intraoperative observations made were canal overhangs and canalplasty performed along with the ease of ossicular assessment.
Methods
Ethical considerations
A written informed consent was taken from all patients before surgery explaining the possibility of postaural, endaural or supra-aural hairline incision. Patients planned for endoscopic myringoplasty were informed of the procedure and the possibility of conversion to a postaural approach. Only patients who volunteered were enrolled in the study. Institutional ethics committee clearance was obtained for the study.
The study was conducted at a tertiary care centre between 2010 and 2012 and included 60 patients with mucosal chronic otitis media. Patients with age >12 years having tympanic membrane perforations of any size and location apart from small or moderate posterior-based perforations were included. Posterior small or moderate sized perforations were excluded as these can generally be managed by a transcanal microscopic approach, except for cases with excessive posterior bony overhangs. None of the patients enrolled in the study were found to have bony overhangs obscuring posterior margins of perforation in cases with posterior perforations. Dry ear for a minimum of 4 weeks was considered a prerequisite. Patients with marginal perforations, cholesteatoma or retraction pockets, ossicular discontinuity or fixity, persistent discharge, revision myringoplasties and sensorineural hearing loss were excluded. Patients with marginal perforations, revision tympanoplasties, ossicular discontinuity, significant middle ear mucosal edema or granulations, craniofacial abnormalities and persistently discharging ears are candidates for cartilage tympanoplasty using the composite cartilage-perichondrial graft or palisading technique. Temporalis fascia has a higher re-perforation or retraction rate than cartilage, particularly in this subset of patients. Perichondrium was not used as a primary graft material, being more opaque than temporalis fascia and due to the possibility of being used as a composite graft material with cartilage in case of a re-perforation or retraction.
All patients undergo a thorough head and neck examination prior to surgery, including the state of nasal mucosa. Patients with significant nasal mucosal abnormalities in form of allergy, hypertrophy or polyposis are managed medically or surgically prior to ear surgery.
A resident unaware of the otoscopic findings randomly distributed the patients into the endoscopy and microscopy groups, to achieve a 30/30 distribution of cases in each group. Patients >16 years of age were operated under local anaesthesia with neuro-sedation, whereas those younger were operated under general anaesthesia. Patients planned for local anaesthesia were administered 25–50 mg intramuscular promethazine for sedation minutes before surgery. 2 % xylocaine was used with adrenaline concentration of 1:200000 for postaural or supra-aural anaesthesia and 1:100,000 for transcanal injection. Transcanal injections were made in all four quadrants with a 26-gauge needle using an ear speculum and canal skin observed for blanching.
Variables recorded pre-operatively were age and sex of the patient, size and location of the tympanic membrane perforation, presence of bony overhangs obscuring perforation margins, status of the contralateral ear and pure tone audiogram. Intra-operative variables recorded were canalplasty to reduce overhangs and the need for curettage of the postero-superior canal wall for ossicular assessment.
Technique
In the endoscopy group, 0° and 30° 4 mm rigid endoscopes (Karl Storz) were used and the procedure was performed using an exclusive transcanal approach with temporalis fascia harvested from a separate supra-auricular hairline incision. The endoscope was held in the left hand and instruments in the right. No endoscope holder was used. After debridement of the margins, the tympanomeatal flap was elevated depending on the size and location of the perforation.
-
Posterior perforation: 12 to 7′o clock.
-
Moderate central and antero-inferior perforation: 12 to 9′o clock.
-
Subtotal or antero-superior perforation: 12 to 11′o clock.
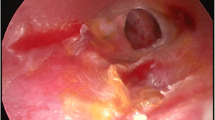
The malleus handle was denuded in perforations encompassing the handle. Incudostapedial joint integrity and mobility were assessed using the 0° and 30° endoscopes successively. A dried fascia graft trimmed to appropriate size was placed in an underlay manner medial to the handle of the malleus. The tip of the umbo was nipped in cases of medialized malleus handle. Graft in all cases was placed medial to umbo, even in cases requiring separation of tympanic membrane remnants from umbo, to prevent graft lateralization. Anterior placement of graft was lateral to bony annulus and medial to fibrous annulus in all cases. No Gelfoam was used in the middle ear. Gelfoam pledgets were placed lateral to the graft with pressure on the anterior canal skin against the bone to prevent anterior blunting (Figs. 1, 2, 3, 4).

Endoscopic image demonstrating large central perforation with anterior tympanosclerotic plaques

Zero degree endoscopic view after elevating fibrous annulus showing chorda tympani and handle of malleus

Panoramic endoscopic view of middle ear after tympanomeatal flap elevation with removal of anterior tympanosclerotic plaques and incidental high jugular bulb

Endoscopic image after final graft placement
Flap elevation and graft placement procedures were similar in the microscopy group. The mastoid periosteum was incised in a rectangular manner creating a flap, which was sutured precisely to ensure appropriate auricular alignment.
Patients were discharged on the following day and recalled for serial post-operative visits on the 10th and 24th day, and at 12 and 24 weeks. Post-operative outcome measures compared were graft uptake rate and hearing status. In addition, feedback was taken from residents under training.
Pure tone thresholds of air conduction, bone conduction and air-bone gaps were calculated as averages at 500, 1,000, 2,000 and 4,000 Hz.
Data were analysed using SPSS (version 16) software with the Student’s t test and Mann–Whitney test.
Results
The mean age of patients in the endoscopy group was 28.30 ± 9.39 years, whereas it was 25.53 ± 8.38 years in the microscopy group (p = 0.571). In the endoscopy group, 50 % of patients were female, whereas 57 % were female in the microscopy group (p = 0.605).
In the endoscopy group, four out of 30 patients (13.33 %) had bilateral disease, whereas 15/30 patients (50 %) had bilateral disease in the microscopy group. All patients with disease in the contralateral ear had tympanic membrane perforation with no evidence of retraction.
No patients in either group were found to have any significant nasal mucosal abnormality.
Table 1 shows the distribution of the size of perforations (SOP) in the endoscopic and microscopic myringoplasty groups. Perforations were defined as small when involving one quadrant, moderate with involvement of two quadrants, large with involvement of three or more quadrants. In the endoscopy group, all small perforations were located in the antero-inferior quadrant. Small perforations in the microscopy group were located one each in the antero-superior and antero-inferior quadrant.
In the endoscopy and microscopy groups, four and five patients had significant canal overhangs, respectively (p = 0.718). The overhangs were most commonly in the antero-inferior and postero-inferior regions. No patient in the endoscopy group required canalplasty and adequate exposure was obtained with the 0° endoscope. All five patients in the microscopy group underwent canalplasty for adequate exposure of the tympanic annulus in its entirety.
The 0° and 30° endoscopes provided an adequate view of the incudostapedial joint complex without the need for any postero-superior canal wall curettage, whereas canal wall curettage was required in four patients in the microscopy group.
In both the endoscopy and microscopy groups, 25/30 (83.3 %) patients had intact and well-healed grafts 24 weeks post-operatively. All patients with significant canal overhangs in either group had intact grafts all throughout the post-operative period. Figure 5 shows the graft uptake in relation to SOP. In the endoscopy group, 4/5 graft defects were small and located in the anterior quadrants with one moderate sized defect. 2/4 graft defects in the endoscopy group were re-perforations following documentation of an intact graft. No spontaneous closure of graft defects was observed in the follow-up period. In the microscopy group, 2/5 patients had complete graft failure with small defects in the other three patients. None of the graft defects in the microscopy group were re-perforations. All small sized graft defects were closed endoscopically by fat grafting. Single case of epithelial pearl was observed anterior to umbo in the endoscopy group, which was excised endoscopically on outpatient basis. No graft lateralization was observed in either group.

Comparison of graft uptake rate with size of perforation for each technique
Table 2 shows the mean air-bone gap pre- and post-operatively in the endoscopy and microscopy groups. The mean air-bone gap decreased by 10.37 dB in the endoscopy group and by 15.5 dB in the microscopy group.
All patients in the endoscopy group reported excellent cosmetic outcomes as the incision scar was well hidden in the hairline. In the microscopy group, 25/30 patients reported excellent cosmetic outcomes and were unaffected by the postaural scar after 24 weeks post-operatively. Five patients in the microscopy group reported their cosmetic outcome as only satisfactory as a result of the incision scar. No patient reported any malalignment of the pinna.
Discussion
Synopsis of key findings
The current study was undertaken to assess the feasibility of endoscopic myringoplasty using the tympanomeatal flap elevation technique and to compare this with the conventional microscopic technique to highlight the advantages and disadvantages and to determine the possibility of incorporating endoscopic myringoplasty in routine otolaryngology training.
Exclusive transcanal endoscopic myringoplasty using temporalis fascia graft provides an excellent alternative to microscopic myringoplasty irrespective of the tympanic membrane perforation size and appears to be user friendly, especially with surgeons familiar with endoscopy.
Comparisons with other studies
In recent times, endoscopes have revolutionized otitis media surgery, playing a significant role in the management of cholesteatoma, sinus tympani disease and facial nerve surgery [2–8]. The prospect of endoscopic myringoplasty and its comparison with the microscopic technique has received relatively little attention [9–14], and has been further confounded by the application of the endoscopic technique to small perforations without tympanomeatal flap elevation [9–11].
Ayache [14] and Harugop et al. [13] used the tympanomeatal flap elevation technique in exclusive transcanal endoscopic myringoplasty with cartilage and temporalis fascia, respectively, and reported satisfactory results.
The panoramic view provided by a 0° rigid endoscope coupled with the addition of angled telescopes provides excellent visualization of the entire tympanic membrane, middle ear and ossicular chain, even in the presence of bony overhangs.
The choice of surgical approach (endomeatal, endaural, postaural) in accordance with the size and location of the perforation has been thoroughly described by Fisch [16], who emphasized the importance of canalplasty in anteriorly based or subtotal perforations. A generous canalplasty not only improves vision of the tympanic annulus in its entirety leading to effective graft placement, but also significantly enhances post-operative graft control and vision [16, 17]. The propensity for extra time consumption, possible flap tears and facial nerve injury [18] often gives rise to reluctance for canalplasty, more so in young surgeons in training.
In the current study, five patients required and underwent canalplasty in the microscopy group. Four patients in the endoscopy group did not require canalplasty despite having significant canal overhang, and overhangs could be negotiated with the 0° endoscope without compromising exposure. It is noteworthy that none of these cases had graft defects in the post-operative period. This is in accordance with the findings of Ayache [14] and Harugop et al. [13] where no patient required canalplasty in endoscopic myringoplasty. Despite these results, it would be premature to avoid canalplasty in all cases with canal overhangs as post-operative vision, cleaning and instrumentation can be hampered.
Four patients in the microscopy group required curettage of the postero-superior canal wall for assessment of the integrity and mobility of the incudostapedial joint complex. The 0° endoscope, however, provided an excellent view of the ossicles without any canal wall curettage.
Graft uptake rates for microscopic myringoplasty using temporalis fascia graft in an underlay technique have been variously described as between 80 and 95 % by various authors [19, 20]. Similar graft uptake rates have been described in endoscopic myringoplasty using temporalis fascia [13]. The graft uptake rate in the current study was 83.3 % in both groups and is in accordance with previous studies. Comparison of graft uptake, however, is questionable as it depends on a host of factors–surgical experience, choice of approach (postaural, endaural, transcanal), eustachian tube function and graft material (cartilage/fascia) [19–21].
In effect, hearing improvement after myringoplasty depends upon graft uptake, residual perforations, graft lateralization or medialization rather than the choice of approach or use of microscope or endoscopes. Endoscopes are merely tools that aid in better visualization, especially in narrow canals and of key structures such as ossicles, and aid in better exposure and graft placement, which ultimately should result in better post-operative graft uptake and hearing results.
The cosmetic outcome was statistically significant with all patients in the endoscopy group reporting excellent results. Five patients (16.67 %) in the microscopy group reported satisfactory results due to scar presence. Coskun et al. [15] and other groups described changes in auriculomastoid angles after endaural and postaural myringoplasties and concluded that the postaural approach resulted in greater alterations in the angle than the endaural approach. In our study, none of the patients operated by the postaural approach reported any misalignment of the pinna.
The questionnaire completed by the residents revealed the willingness of most to become more familiar with endoscopic myringoplasty and to take time to learn the new technique just as with endoscopic sinus surgery. Initial bleeding on flap elevation and consequent endoscope fogging together with the single-handed approach were the most common difficulties encountered by residents. Residents trained in transcanal surgery approached the endoscopic technique with much more enthusiasm.
Limitations and recommendations
Limitations of the present study included the relatively small sample size leading to a lack of generalization of the findings. Further studies incorporating comparisons in the management of exclusively anteriorly based perforations or perforations in canal overhangs may lead to more specific conclusions. Furthermore, the prospect of exclusive transcanal endoscopic canalplasty in severe anterior or inferior bony overhangs seems promising.
Conclusions
Endoscopic myringoplasty is an effective and promising alternative to the traditional microscopic technique using the postaural approach and leads to comparable outcomes in terms of graft uptake and hearing. Canalplasty and postaural incision can be avoided in the absence of major canal overhangs. Finally, the procedure does seem to have a place in resident training and would be accepted with reasonable enthusiasm.
References
Chen B, Fry TL, Fischer ND (1979) Otoscopy and photography: a new method. Ann Otol Rhinol Laryngol 88:771–773
Migirov L, Shapira Y, Hoeowitz Z, Wolf M (2011) Exclusive endoscopic ear surgery for acquired cholesteatoma. Otol Neurotol 32:433–436
Marchioni D, Alicandri-Ciufelli M, Molteni G, Genovese E, Presutti L (2010) Endoscopic tympanoplasty in patients with attic retraction pockets. Laryngoscope 120:1847–1855
Yung MW (1994) The use of rigid endoscopes in cholesteatoma surgery. J Laryngol Otol 108:307–309
Marchioni D, Alicandri-Ciufelli M, Molteni G, Villari D, Monzani D, Presutti L (2011) Ossicular preservation after exclusive endoscopic transcanal tympanoplasty: preliminary experience. Otol Neurotol 32(4):626–631
Marchioni D, Villari D, Alicandri-Ciufelli M, Piccinini A, Presutti L (2011) Endoscopic open technique in patients with middle ear cholesteatoma. Eur Arch Otorhinolaryngol 268(11):1557–1563
Marchioni D, Alicandri-Ciufelli M, Piccinini A, Genovese E, Monzani D, Tarabichi M et al (2011) Surgical anatomy of the transcanal endoscopic approach to the tympanic facial nerve. Laryngoscope 121(7):1563–1571
Abdel Baki F, El Dine MB, El Saiid I, Bakry M (2002) Sinus tympani endoscopic anatomy. Otolaryngol Head Neck Surg 127(3):158–162
El-Guindy A (1992) Endoscopic transcanal myringoplasty. J Laryngol Otol 106:493–495
Yadav SP, Aggarwal N, Julaha M, Goel A (2009) Endoscope-assisted myringoplasty. Singap Med J 50:510–512
Raj A, Meher R (2001) Endoscopic transcanal myringoplasty: a study. Indian J Otolaryngol Head Neck Surg 53:47–49
Karhuketo TS, Ilomaki JH, Puhakka HJ (2001) Tympanoscope-assisted myringoplasty. Otorhinolaryngology 63:353–358
Harugop AS, Mudhol RS, Godhi RA (2008) A comparative study of endoscope assisted myringoplasty and microscope assisted myringoplasty. Indian J Otolaryngol Head Neck Surg 60:298–302
Ayache S (2013) Cartilaginous myringoplasty, the endoscopic transcanal procedure. Eur Arch Otorhinolaryngol 270:853–860
Coskun BU, Cinar U, Seven H, Ugur S, Dadas B (2006) The effects of the incision types in myringoplasty operations on cosmetics. Eur Arch Otorhinolaryngol 263:820–822
Fisch U (2008) Tympanoplasty, mastoidectomy and stapes surgery, 2nd edn. Thieme, New York, pp 8–11
Vijayendra H, Ittop CJ, Sangeetha R (2008) Comparative study of hearing improvement in type 1 tympanoplasty with and without canalplasty. Indian J Otolaryngol Head Neck Surg 60(4):341–344
Adad B, Rasgon BM, Ackerson L (2001) Relationship of the facial nerve to the tympanic annulus: a direct anatomic examination. Laryngoscope 109(8):1189–1192
Vartiainen E, Nuutinen J (1993) Success and pitfalls in myringoplasty: follow-up study of 404 cases. Am J Otol 14(3):301–305
Westerberg J, Harder H, Magnuson B, Westerberg L, Hyden D (2011) Ten year myringoplasty series: does the cause of perforation affect the success rate? J Laryngol Otol 125:126–132
Onal K, Arslanoglu S, Songu M, Demiray U, Demirpehlivan IA (2012) Functional results of temporalis fascia versus cartilage tympanoplasty in patients with bilateral chronic otitis media. J Laryngol Otol 126:22–25
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lade, H., Choudhary, S.R. & Vashishth, A. Endoscopic vs microscopic myringoplasty: a different perspective. Eur Arch Otorhinolaryngol 271, 1897–1902 (2014). https://doi.org/10.1007/s00405-013-2673-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-013-2673-z