
Abstract
There is growing interest in complementary and alternative medicine (CAM) amongst the general population. Little information is available on CAM use in otolaryngology patients in the UK. Despite concerns over safety, efficacy and cost-effectiveness, CAM use is common amongst ENT patients. Patients perceive these medications as possible boosters to their immune system. It is becoming increasingly important that health care providers in all specialties ask their patients about CAM use and are aware of the implications it carries. The objective is to study the prevalence and pattern of CAM use among adult and paediatric ENT patients in a UK teaching hospital. A cross-sectional study was done by sending anonymous questionnaire to all outpatient and elective inpatients over a 3-month period. Response rate was 73% (1,789/2,440). Prominent demographics: female, married, over-50 s. Sixty percent had used CAM, 35% in last year. Most common herbs: cod liver oil (n = 481), garlic (n = 255), cranberry (n = 224); non-herbal: massage (n = 287), acupuncture (n = 233), aromatherapy (n = 170). Most commonly cited reasons for using CAM: general health, enhanced immunity and prevention/treatment of common illnesses like the common cold, asthma and bodily aches and pains.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The Cochrane Collaboration defines complementary and alternative medicine (CAM) as, “all such practices and ideas which are outside the domain of conventional medicine in several countries and defined by its users as preventing or treating illness, or promoting health and well-being” [1]. In today’s Western societies, this usually translates to anything associated with the words natural or herbal. There is a certain amount of scepticism amongst Western health practitioners towards such remedies, a scepticism which is reflected in the paucity of attention they receive in most medical schools and post-graduate education programmes despite recommendations that familiarisation about their use should be increased amongst health care professionals [2, 3]. This is somewhat ironic when we consider that up to 30% of conventional medicines are themselves derived from plants [4]. Vincristine from periwinkle and digitalis from foxglove are notable examples.
Nonetheless, the use of CAM is on the rise, with an estimated £1.6 billion being spent on it annually in the UK alone [5]. The current UK prevalence of CAM use is reported at 25% and rising, and the number of CAM practitioners is within the region of 50,000 [5]. In one study, 69% of patients admitted to using CAM, 49% of whom had used it within the last year [6]. A systematic review assessing prevalence in 13 countries showed that 31% of cancer patients use some form of CAM [7]. Its use is also prevalent amongst paediatric populations [8]. It is worrying, however, that most patients who admit to taking CAM or administering it to their children fail to reveal this usage to their physicians, and oftentimes use it instead of their conventional prescribed medications [5, 9–12]. This has many implications for safety as many of these alternative remedies have been shown to have a range of side effects and exhibit pharmacodynamics that result in an array of herb–drug interactions [13, 14].
Following several isolated incidents, including one episode of difficult-to-manage epistaxis following concomitant use of aspirin and garlic tablets, the latter which enhanced the anti-platelet effect of the aspirin, it became our belief that many otolaryngology patients were using CAM without our knowledge. We decided to study the prevalence of such usage amongst our patient population, as research done in ENT populations is limited and mostly based in the US. In addition, we felt that that our findings would be translatable to all other specialties, especially following a previously performed pilot on general surgical patients which suggested that the prevalence might be high [6].
Patients and methods
The study was conducted in the Otolaryngology Department of the Aberdeen Royal Infirmary, Aberdeen, Scotland. This is a UK teaching hospital in an urban setting and provides secondary and tertiary healthcare to the population of both the city of Aberdeen and that of the rural Northeast of Scotland, an estimated population number of 500,000.
A cross-sectional questionnaire survey study of 2,440 consecutive patients attending the ENT Department was undertaken over a 14-week period from October 2005 to January 2006. Adult outpatients from the general otolaryngology and head and neck clinics were included in the study as well as adult inpatients admitted for both emergencies and elective surgery. After verbal consent, patients were asked to fill in an anonymous questionnaire with a covering letter attached. This was done before the patient was seen by the otolaryngologist. Invitations were restricted to English-speaking patients, and those aged 16 years and older only. A nurse or investigator was always present to provide explanations if needed.
The questionnaire comprised of a tick list of 49 common herbal preparations and alternative therapies. It also contained a section for demographic data where patients were asked to input their age, sex, marital status and level of education achieved. Ethnicity was not included. Specific enquiry was also made about their reason for attending the clinic, reason for CAM use, opinion on CAM efficacy, GP knowledge of their use of CAM and details on where they had purchased it.
Data were entered into and analysed using SPSS for Windows version 13.0 and Microsoft Excel 2003. Descriptive statistics were used to explore “ever versus never” use of CAM by demographics including age, sex, marital status and occupation. Fisher’s Exact χ2 tests were used and a P value of <0.05 was considered statistically significant.
Results
Of the 2,440 patients who were interviewed via the questionnaire, 1,789 completed it (73% response rate). Of those who failed to complete the questionnaire, the most common reason cited was lack of time in the clinic. Of the 1,789 patients, 865 (48.4%) were male and 924 (51.6%) were female. The majority of patients (n = 542, 30.3%) were over the age of 60. Most patients (n = 1,002, 56%) gave a marital status of being married. Five hundred and six patients (28.3%) professed to having received no formal education past the basic primary level, while 351 patients (19.6%) had acquired a university education (Table 1).
There was a high prevalence of CAM use. Over 60% of patients (n = 1,079) had used some form of CAM, almost 35% (n = 625) of whom had used it within the past 12 months; only 43.5% (n = 469) had informed their family physician of its use. The majority of patients were using CAM for reasons other than what they had attended the ENT clinic for (n = 883, 81.8%). Approximately 53% (n = 573) of patients believed that CAM was effective and 35% (n = 380) thought that it might be, as opposed to only 8% (n = 86) who doubted its benefits. Over half of the patients (56%, n = 602) said that they would recommend CAM to others. In fact 60% (n = 643) had learnt about CAM from family and friends. Interestingly, 25% (n = 267) had been recommended CAM by a healthcare professional. CAM was by far most readily accessible as an over-the-counter (OTC) medication (n = 774, 72%), with the family physician (n = 124) and the internet (n = 65) also being cited.
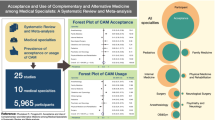
The type of CAM used was broadly divided into two main groups: herbal and non-herbal remedies. Of the herbal remedies, cod liver oil, garlic, cranberry, aloe vera, primrose oil and Echinacea were most commonly used (Fig. 1). Massage, acupuncture, aromatherapy, chiropractic, reflexology and osteopathy were the most common forms of non-herbal CAM used (Fig. 2). Each remedy was used for an array of ailments, but the most commonly cited use was for general health (Tables 2, 3).

Types of herbal CAM used

Types of non-herbal CAM used
Discussion
Interest in CAM has grown in recent years. The prevalence of CAM usage in our population was found to be 61%, similar to national figure of 71% seen in GP practices in the UK [15]. Similarly, our results show that CAM was more likely to be used by highly educated, middle-aged females, a finding which correlates with findings in other recent research [16]. Despite this, the average physician may not be aware of the purpose, side effects and complications that are associated with many of these products. With this in mind, a pharmacopoeia of herbal remedies commonly used in the UK including the known potential side effects, herb–drug interactions and peri-operative precautions is detailed below. This quick reference list and included table (Table 4) should serve to increase awareness about a once covert area of medicine that is becoming increasingly prominent across all surgical specialties.
Cod liver oil
Cod liver oil contains high levels of omega-3 fatty acids, in particular eicosapentaenoic acid (ECA), and very high levels of vitamins A and D. It is used for arthritis, where it has been found useful as an NSAID-sparing supplement, and in the reduction in the incidence of thrombotic cardiovascular disease through its ability to reduce plasma triglyceride levels, blood pressure, platelet aggregation, arrhythmia, and atherogenesis [17–19]. Part of its mechanism of action lies in its effect on adenosine diphosphate-induced platelet aggregation [19]. This action is enhanced in patients taking aspirin [20]. The American Society of Anesthesiology (ASA) therefore recommends that cod liver oil is discontinued pre-operatively 2–3 weeks before surgery [21].
Garlic (Allium sativum)
Garlic is widely used for its cardioprotective qualities, in particular as a remedy against atherosclerosis, hypertension and hypercholesterolemia, though these benefits have recently been debated [22]. Allicin, the active ingredient in garlic, and its transformation products inhibit platelet aggregation and do so in a dose-dependent manner [23]. The anti-platelet effect of ajolene, also found in garlic, may be irreversible and may potentiate the action of other platelet inhibitors such as prostacyclin, indomethacin, and dipyridamole [24]. Because of this potential for irreversible inhibition of platelet function, it is advisable to discontinue the use of garlic at least 7 days prior to surgery, especially if postoperative bleeding is a particular concern or other platelet inhibitors are given [23].
Cranberry (Vaccinium spp.)
Taken either in its juiced form or as capsules, cranberry is typically used for its anti-adhesion properties against bacterial urinary tract infections. It has been shown to inhibit the attachment of bacteria to the walls of the urethra and bladder [25]. Cranberry also contains anthocyanidin flavonoids which have been shown to induce, inhibit, or act as a substrate for the biosynthesis of several cytochrome P-450 isoenzymes involved in the metabolism of S-warfarin [26]. This is thought to prolong warfarin’s action, thus increasing patient’s bleeding risk. In one recent study, the area under the INR-time curve was shown to be increased by 30% [27]. Though evidence in still inconclusive, the consensus is that careful monitoring of the INR should be exercised in patients taking warfarin and cranberry concurrently.
Echinacea (Echinacea spp.)
Echinacea, a member of the daisy family, is commonly used by patients to boost the immune system and prevent minor illnesses such as the common cold. In a recent meta-analysis [28], Echinacea was found to be beneficial in reducing the incidence and duration of the common cold. In a 2008 report the European Medicines Agency (EMEA) approved the use of dried Echinacea purpurea for respiratory tract infections, including the common cold [29]. The active ingredients are polysaccharides, alkylamides and cichoric acid which act as immunostimulators, enhancing phagocytosis and non-specific T-cell stimulation [30]. It is thought, though not conclusively proven, that this effect may therefore counteract the effect of immunosuppressive drugs [31]. This may have implications for patients awaiting organ transplantation. In contrast, long-term use of 8 weeks or more is associated with immunosuppression which may result in postoperative complications such as poor wound healing and opportunistic infections [23].
Other adverse effects include allergic reactions and it should therefore be used with caution in atopic patients [32]. There has been some concern about its effect on hepatic function as it is a known inhibitor of cytochrome P450 3A4 and sulfotransferase, but conclusive evidence is lacking [31]. Perioperative precautions are thus advised especially in patients in which disruption in hepatic function or blood flow is anticipated, either secondary to anaesthetic administration or manipulation of the liver [23]. The ASA recommend that Echinacea be discontinued 2–3 weeks pre-operatively [21].
St. John’s Wort (Hypericum perforatum)
St. John’s wort is a popular herbal remedy for mood, used mainly for depression, anxiety and insomnia. Its active ingredients are hyperforin and hypericin, which are thought to act as inhibitors of serotonin (5-HT)-uptake and possibly of dopamine, noradrenaline, gamma-aminobutyric acid (GABA) and glutamate [33]. A recent Cochrane review [34] states that preparations of Hypericum were significantly superior to placebo and as similarly effective as standard antidepressants, but with fewer side effects. Known side effects include dry mouth, dizziness, fatigue, constipation, nausea, swelling and rarely, photosensitization [35]. Potentially more dangerous are its known herb–drug interactions, which occur because of its ability to induce liver enzymes [23]. Affected drugs include indinavir, ethinyl estradiol, cyclosporin, digoxin, calcium channel blockers and serotonin receptor antagonists (SSRIs). The latter may result in seretonergic syndrome [35]. In the perioperative setting, alfentanil, midazolam and lidocaine may also be affected, and prolonged postoperative sedation is documented [36]. It is suggested that St. John’s wort be discontinued at least 5 days pre-operatively [21, 23].
Ginkgo (Ginkgo biloba)
Ginkgo is believed to possess nootropic, or memory-enhancing properties, and is used by many for this reason, but also for delay in dementia and concentration, and has also been extensively researched for its role in otolaryngological conditions such as tinnitus and vertigo, and for its effect in peripheral vascular disease and age-related macular degeneration. The compounds believed to be responsible for its pharmacological effects are the terpenoids and flavonoids. Objective evidence for these effects is lacking, and any effect it may have in alleviating tinnitus are thought to be due to a strong placebo effect [37, 38]. Ginkgo appears to alter vasoregulation, act as an antioxidant, modulate neurotransmitter and receptor activity, and inhibit platelet-activating factor [23]. It is the latter that raises the greatest concern for the perioperative period since platelet function may be altered. For this reason, ginkgo should be ceased at least 36 h prior to surgery [21, 23].
Ginseng (Panax ginseng)
This root has been traditionally taken as an aphrodisiac, a natural stimulant, a remedy against diabetes mellitus, a protective agent against stress and as a restorative agent in the body’s homeostasis, when it is labelled an adaptogen. The active ingredients in ginseng are ginsenosides, of which there are several. The most common side effect is insomnia. The main clinical effects of these compounds are a lowering of blood glucose levels in both non-diabetic and type 2 diabetic patients, and a possible anti-platelet effect, an effect that is potentially irreversible due to the compound panaxynol [39–41]. The former effect is analogous to that of adrenal steroid hormones and may cause unintended pre-operative ginseng-induced hypoglycaemia, especially in the non-diabetic, fasted patient. Interaction with warfarin is also probable [42]. For these reasons, ginseng should be discontinued at least 7 days prior to surgery [23].
Valerian (Valeriana officinalis)
Valerian is the most common herb found in herbally based sleeping remedies, as it thought to possess relaxant and anxiolytic properties. It contains many active ingredients, but the sesquiterpenes are responsible for most of its pharmacological effects, the main one being an increase the activity of GABA receptors causing a dose-dependent sedation and hypnosis, a state that can be attenuated by the concomitant use of benzodiazepines and other drugs acting on the GABA receptors [23, 43]. A valerian withdrawal syndrome of delirium and cardiac complications has also been described if it is stopped too abruptly. Tapering off of the dose is thus recommended several weeks before surgery where possible. Otherwise it should be used up to the day of surgery and monitoring should be carried out for possible withdrawal and treated with benzodiazepines if present [44].
Kava (Piper methysticum)
Kava, the dried root of the pepper plant P. methysticum, is another popular sedative and anxiolytic with proven effect in both, albeit small [45]. The active ingredients, the kavalactones, act in a similar manner to valerian by their potentiating effect on GABA receptors. They have also been found to possess some pharmacological activity as antiepileptics and local anaesthetics [46]. Heavy use can cause kava dermopathy, a condition characterised by reversible, scaly cutaneous eruptions, but its potential for addiction is unknown [47]. It has been withdrawn in Canada following reported cases of kava-induced fulminant hepatitis, and has been reported to have caused a coma due to a kava–alprazolam interaction in at least one case [48, 49]. The half-life of kavalactones is only 9 h, and for this reason, it can be discontinued up to 24 h before surgery [23].
Ephedra (Ephedra sinica)
Ephedra, also known as Ma Huang in Chinese medicine, is used to promote weight loss, increase energy, and treat respiratory tract conditions, such as asthma and bronchitis [23]. The active ingredients in ephedra are alkaloids, including ephedrine, pseudoephedrine, norephedrine, methylephedrine, and norpseudoephedrine [50]. Ephedrine is the main active ingredient and acts both as a powerful adrenergic agonist and by causing the release of endogenous norepinephrine, causing tachycardia and an increase in blood pressure and a relaxation of bronchial smooth muscle. These effects are dose-related, and if used in large quantities, may lead to many adverse effects, including fatal neurological and cardiac complications [51]. There have been cases of similar deaths occurring after the use of ephedra in prescribed doses, however [52]. For these reasons, ephedra-containing medicines are currently banned in the US, and are sold as prescription-only medications in the UK. Anaesthetic contraindications to the use of ephedra include ventricular arrhythmias following halothane administration secondary to sensitization of the myocardium to exogenous catecholamines; peri-operative haemodynamic instability secondary to tachyphylaxis and depletion of endogenous catecholamine stores associated with long-term ephedra use [53]. One serious herb–drug interaction is life-threatening hyperpyrexia, hypertension and coma when ephedra is used with monoamine oxidase inhibitors [23]. Given its potential neurological and cardiovascular complications and potential for herb–drug interactions, ephedra should be discontinued at least 24 h before surgery, given its relatively short half-life of 5.6 h [23].
Milk thistle (Silybum marianum)
Milk thistle is used for its alleged protective effects on the liver in conditions such as cirrhosis and hepatitis, and recent experimental and clinical studies suggest that milk thistle extracts may also have anticancer, antidiabetic, and cardioprotective effects [54]. The active ingredient in milk thistle is silymarin, the mechanism of action of which is unclear. It is known to undergo enterohepatic recirculation and is thought to concentrate in hepatocytes and compete with toxins for hepatocyte binding and penetration [55]. It may decrease the trough concentrations of indivar in humans, it interacts with oestrogens and progesterones, and a preliminary study has shown it to reduce the activity of human liver microsomal cytochrome P-450 [56]. Whilst no herb–drug interactions have been discovered to date with milk thistle use, caution is probably advisable given its hepatic effects, and it is recommended that it be discontinued 7 days pre-operatively [21].
Comfrey (Symphytum spp.)
Comfrey is popular for its alleged ability to accelerate wound, tissue and bone healing, and is typically used as a salve or poultice. The active ingredient thought to enhance this healing is allantoin, a cell proliferant. Several studies suggest that there is evidence for this, especially in reducing post-traumatic myalgia, quickening the rehabilitative process in ankle sprains and easing osteoarthritic pain [57–59]. However, it is also used internally for ailments such as gastric ulcers and skin conditions in the form of a tea. This internal use is potentially harmful as comfrey also contains the pyrrolizidine alkaloids lasiocarpine and symphytine. These compounds and their N-oxides have been shown to be hepatotoxic in humans [60]. Another of these alkaloids, riddelliine, has been found to be carcinogenic in rats [61]. Hepatotoxicity is thought to be caused by comfrey-induced veno-occlusive disease, a result of the biotransformation of these alkaloids by hepatic microsomal enzymes to highly reactive, alkylating pyrroles. The result is a non-thrombotic obliteration of small hepatic veins leading to cirrhosis and eventually liver failure [60]. For this reason, comfrey is banned in Germany and Canada. Because of its effect on the liver, the action of several anaesthetic agents can become unpredictable, and so its use is discouraged altogether [61]. Alternatively, it should be stopped at least 2 weeks prior to surgery.
Saw palmetto (Serenoa repens or Sabal surrulata)
Saw palmetto is mainly used for its effect on urinary flow in benign prostatic hyperplasia (BPH). One systematic review [62] supports this effect, stating that it improves urinary flow in mild to moderate cases of BPH when compared to a placebo, and at least matches the effect of finasteride with fewer of the side effects. Its active ingredients are the sterol components, beta-sitosterol and stigmasterol, which have also been shown to inhibit prostate cancer growth by increasing p53 protein expression and inhibiting carcinoma development by decreasing the expression of proteins p21 and p27 [63]. It is generally considered to be a safe herb with typically mild side effects, including gastrointestinal upset and headache [64]. Intraoperative haemorrhage associated with saw palmetto use has been reported, however, and for this reason the ASA advises that is be discontinued at 2–3 weeks pre-operatively [23, 65].
Green tea (Camellia sinensis)
Green tea is widely used and readily available. It is popularly believed to reduce the risk of heart disease. One review of the literature suggests that green tea, its extract or its purified polyphenol (−)-epigallocatechin-3-gallate (EGCG) may be partially preventative in prostate and breast cancer, and may also reduce the risk of atherosclerosis and neurodegenerative disorders [66]. Recently, however, EGCG has been shown to be potentially hepatotoxic [67]. Green tea is also known to contain carotenoids, tocopherols, vitamin C, certain minerals (Cr, Mn, Se and Zn), and phytochemical compounds. However, one report suggests that it can probably antagonise the effect of warfarin in large quantities as it is a source of vitamin K [68]. It has also been shown in one in vitro study to alter the pharmacodynamics of midazolam, but again, only if ingested in large quantities [69]. It may therefore be concluded that whilst the occasional consumption of green tea may be beneficial, chronic consumption might be associated with suboptimal anticoagulation in patients on warfarin, hepatotoxicity, and may affect the predictability of benzodiazepines such as midazolam, an important effect during anaesthesia. Whilst there is no consensus regarding whether green tea should be ceased or not pre-operatively, it is the opinion of the authors that in patients who consume large amounts of green tea on a regular basis, it should be stopped at least 1 week pre-operatively to prevent complications.
Conclusion
This study highlights the high usage of CAM in ENT patients, a surgical population. It can be postulated that use in other surgical specialties is equally as high. Given the wide array of possible peri-operative complications that can occur with the most popular forms of CAM, it behoves the surgeon and anaesthetist alike to include a full herbal remedy intake history during the pre-operative assessment. In this way, safety during the peri-operative period can be maximized. This study also argues the case for the inclusion of a more robust representation of CAM in the curriculum of both medical schools and post-graduate education programmes.
References
Manheimer E, Berman B (2008) Cochrane Complementary Medicine Field. About The Cochrane Collaboration (Fields). Cochrane Collab (2):CE000052
Taylor N, Blackwell A (2008) Complementary and alternative medicine familiarization: what’s happening in medical schools in Wales? Evid Based Complement Altern Med, January 16 (Epub ahead of print)
Referrals to complementary therapists. The British Medical Association, 2006. Available at http://www.bma.org.uk
Kleiner SM (1995) The true nature of herbs. Phys Sports Med 23:13
House of Lords (2000) Complementary and alternative medicine. Select Committee on Sciences and Technology, 6th report. Science and Technology Committee Publications
Shakeel M, Bruce J, Jehan S, McAdam TK, Bruce DM (2008) Use of complementary and alternative medicine by patients admitted to a surgical unit in Scotland. Ann R Coll Surg Engl 90(7):571–576
Ernst E, Cassileth BR (1998) The prevalence of complementary/alternative medicine in cancer: a systematic review. Cancer 83(4):777–782
Shakeel M, Little SA, Bruce J, Ah-See KW (2007) Use of complementary and alternative medicine in pediatric otolaryngology patients attending a tertiary hospital in the UK. Int J Pediatr Otorhinolaryngol 71(11):1725–1730
Jose VW, Bhalla A, Sharma N, Hota D, Sivaprasad S, Pandhi P (2007) Study of association between use of complementary and alternative medicine and the non-compliance with modern medicine in patients presenting to the emergency department. J Postgrad Med 53:96–101
Ernest E (2007) Noncompliance with conventional medicine and the use of complementary/alternative medicine. J Postgrad Med 53:85
Eisenberg DM, Davis RB, Ettner SL (1998) Trends in alternative medicine use in the United States 1990–1997. JAMA 280:1569–1575
Astin JA (1998) Why patients use alternative medicine: results of a national study. JAMA 279(19):1548–1553
Woolf AD (2003) Herbal remedies and children: do they work? Are they harmful? Pediatrics 112:240–246
Hu Z, Yang X, Ho PC, Chan SY, Heng PW, Chan E, Duan W, Koh HL, Zhou S (2005) Herb–drug interactions: a literature review. Drugs 65(9):1239–1282
Featherstone C, Godden D, Gault C, Emslie M, Took-Zozaya M (2003) Prevalence study of concurrent use of complementary and alternative medicine in patients attending primary care services in Scotland. Am J Public Health 93:1080–1082
Bishop FL, Lewith GT (2008) Who uses CAM? A narrative review of demographic characteristics and health factors associated with CAM use. Evid Based Complement Altern Med, March 13 (Epub ahead of print)
Galarraga B, Ho M, Youssef HM, Hill A, McMahon H, Hall C et al (2008) Cod liver oil (n-3 fatty acids) as a non-steroidal anti-inflammatory drug sparing agent in rheumatoid arthritis. Rheumatology (Oxf) 47(5):665–669
Saremi A, Arora R (2008) The utility of omega-3 fatty acids in cardiovascular disease. Am J Ther, December 15 (Epub ahead of print)
Sanders TAB, Oakley FR, Miller GJ, Mitropoulos KA, Crook D, Oliver MF (1997) Influence of n-6 versus n-3 polyunsaturated fatty acids in diets low in saturated fatty acids on plasma lipoproteins and hemostatic factors. Arterioscler Thromb Vasc Biol 17(12):3449–3460
Larson MK, Ashmore JH, Harris KA, Vogelaar JL, Pottala JV, Sprehe M et al (2008) Effects of omega-3 acid ethyl esters and aspirin, alone and in combination, on platelet function in healthy subjects. Thromb Haemost 100(4):634–641
O’Brien D (2002) Notes from the 2001 American Society of Anesthesiologists annual meeting. J Perianesth Nurs 17(2):130–141
Gardner CD, Lawson LD, Block E, Chatterjee LM, Kiazand A, Balise RR et al (2007) Effect of raw garlic vs. commercial garlic supplements on plasma lipid concentrations in adults with moderate hypercholesterolemia: a randomized clinical trial. Arch Intern Med 167(4):346–353
Ang-Lee MK, Moss J, Yuan C (2001) Herbal medicines and perioperative care. JAMA 286:208
Apitz-Castro R, Escalante J, Vargas R, Jain MK (1986) Ajoene, the antiplatelet principle of garlic, synergistically potentiates the antiaggregatory action of prostacyclin, forskolin, indomethacin and dypiridamole on human platelets. Thromb Res 42:303–311
Jepson RG, Craig JC (2008) Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev (1):CD001321. doi:10.1002/14651858.CD001321.pub4
Pham DQ, Pham AQ (2007) Interaction potential between cranberry juice and warfarin. Am J Health Syst Pharm 64(5):490–494
Mohammed Abdul MI, Jiang X, Williams KM, Day RO, Roufogalis BD, Liauw WS et al (2008) Pharmacodynamic interaction of warfarin with cranberry but not with garlic in healthy subjects. Br J Pharmacol 154(8):1691–1700
Shah SA, Sander S, White CM, Rinaldi M, Coleman CI (2007) Evaluation of Echinacea for the prevention and treatment of the common cold: a meta-analysis. Lancet Infect Dis 7(7):473–480
Kreft S (2008) Assessment report on Echinacea purpura (L.) Moench, Herba Recens. EMEA 2008, March 6. ref:EMEA/HMPC/104918/2006
Schoneberger D (1992) The influence of immune stimulating effects of pressed juices from Echinacea purpurea on the course and intensity of the common cold: results of a double-blind clinical trial. Forum Immunol 2:18
Boullata JI, Nace AM (2000) Safety issues with herbal medicine. Pharmacotherapy 20:257–269
Mullins RJ (1998) Echinacea-associated anaphylaxis. Med J Aust 168:170–171
Butterweck V (2003) Mechanism of action of St John’s wort in depression: what is known? CNS Drugs 17(8):539–562
Linde K, Berner MM, Kriston L (2008) St John’s wort for major depression. Cochrane Database Syst Rev (4):CD000448. doi:10.1002/14651858.CD000448.pub3
Ernst E, Rand JI, Barnes J, Stevinson C (1998) Adverse effects profile of the herbal antidepressant St. John’s wort (Hypericum perforatum L.). Eur J Clin Pharmacol 54:589
Crowe S, Keating K (2002) Delayed emergence and St. John’s Wort. Anesthesiology 96:1025
Birks J, Grimley Evans J (2007) Ginkgo biloba for cognitive impairment and dementia. Cochrane Database Syst Rev (2):CD003120. doi:10.1002/14651858.CD003120.pub2
Hilton M, Stuart E (2004) Ginkgo biloba for tinnitus. Cochrane Database Syst Rev (2):CD003852. doi:10.1002/14651858.CD003852.pub2
Vuksan V, Sievenpiper JL, Koo VY et al (2000) American ginseng (Panax quinquefolius L) reduces postprandial glycemia in nondiabetic subjects and subjects with type 2 diabetes mellitus. Arch Intern Med 160:1009–1013
Kuo SC, Teng CM, Lee JC, Ko FN, Chen SC, Wu TS (1990) Antiplatelet components in Panax ginseng. Planta Med 56:164–167
Teng CM, Kuo SC, Ko FN et al (1989) Antiplatelet actions of panaxynol and ginsenosides isolated from ginseng. Biochim Biophys Acta 990:315–320
Janetzky K, Morreale AP (1997) Probable interaction between warfarin and ginseng. Am J Health Syst Pharm 54:692–693
Santos MS, Ferreira F, Cunha AP, Carvalho AP, Ribeiro CF, Macedo T (1994) Synaptosomal GABA release as influenced by valerian root extract-involvement of the GABA carrier. Arch Int Pharmacodyn Ther 327:220–231
Garges HP, Varia I, Doraiswamy PM (1998) Cardiac complications and delirium associated with valerian root withdrawal. JAMA 280:1566–1567
Pittler MH, Ernst E (2003) Kava extract versus placebo for treating anxiety. Cochrane Database Syst Rev (1):CD003383. doi:10.1002/14651858.CD003383
Meyer HJ (1967) Pharmacology of kava. 1. Psychopharmacol Bull 4:10–11
Norton SA, Ruze P (1994) Kava dermopathy. J Am Acad Dermatol 31:89–97
Russman S, Barguil Y, Cabalion P, Kritsanida M, Duhet D, Lauterburg BH (2003) Hepatic injury due to traditional aqueous extracts of kava root in New Caledonia. Eur J Gastroenterol Hepatol 15:1033
Almeida JC, Grimsley EW (1996) Coma from the health food store: interaction between kava and alprazolam. Ann Intern Med 125:940–941
Gurley BJ, Gardner SF, Hubbard MA (2000) Content versus label claims in ephedra-containing dietary supplements. Am J Health Syst Pharm 57:963–969
Nightingale SL (1997) From the Food and Drug Administration. JAMA 278:15
Roizen MF (1994) Anesthetic implications of concurrent diseases. In: Miller RD (ed) Anesthesia, 4th edn. Churchill Livingstone, New York, pp 903–1014
Haller C, Benowitz N (2000) Adverse cardiovascular and central nervous system events associated with dietary supplements containing ephedra alkaloids. N Engl J Med 343(25):1833–1838
Tamayo C, Diamond S (2007) Review of clinical trials evaluating safety and efficacy of milk thistle (Silybum marianum [L.] Gaertn.). Integr Cancer Ther 6(2):146–157
Boerth J, Strong KM (2002) The clinical utility of milk thistle (Silybum marianum) in cirrhosis of the liver. J Herb Pharmacother 2(2):11–17
Zuber R, Modriansky M, Dvorak Z, Rohovzky P, Ulrichova J, Simanek V et al (2002) Effect of silybin and its congeners on human liver microsomal cytochrome P450 activities. Phytother Res 16:632–638
Bleakley CM, McDonough SM, MacAuley DC (2008) Some conservative strategies are effective when added to controlled mobilisation with external support after acute ankle sprain: a systematic review. Aust J Physiother 54(1):7–20
Barna M, Kucera A, Hladícova M, Kucera M (2007) Wound healing effects of a Symphytum herb extract cream (Symphytum × uplandicum NYMAN:): results of a randomized, controlled double-blind study. Wien Med Wochenschr 157(21–22):569–574
Grube B, Grünwald J, Krug L, Staiger C (2007) Efficacy of a comfrey root (Symphyti offic. radix) extract ointment in the treatment of patients with painful osteoarthritis of the knee: results of a double-blind, randomised, bicenter, placebo-controlled trial. Phytomedicine 14(1):2–10
Stickel F, Seitz HK (2000) The efficacy and safety of comfrey. Public Health Nutr 3(4A):501–508
Williams L, Chou MW, Yan J, Young JF, Chan PC, Doerge DR (2002) Toxicokinetics of riddelliine, a carcinogenic pyrrolizidine alkaloid, and metabolites in rats and mice. Toxicol Appl Pharmacol 182(2):98–104
Wilt T, Ishani A, MacDonald R (2002) Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev (3):CD001423. doi:10.1002/14651858.CD001423
Scholtysek C, Krukiewicz AA, Alonso JL, Sharma KP, Sharma PC, Goldmann WH (2009) Characterizing components of the saw palmetto berry extract (SPBE) on prostate cancer cell growth and traction. Biochem Biophys Res Commun 379:795–798
Avins AL, Bent S, Staccone S, Badua E, Padula A, Goldberg H et al (2008) A detailed safety assessment of a saw palmetto extract. Complement Ther Med 16(3):147–154
Cheema P, El-Mefty O, Jazieh AR (2001) Intraoperative haemorrhage associated with the use of extract of saw palmetto herb: a case report and review of literature. J Intern Med 250(2):167–169
Clement Y (2009) Can green tea do that? A literature review of the clinical evidence. Prev Med, May 22 (Epub ahead of print)
Mazzanti G, Menniti-Ippolito F, Moro PA, Cassetti F, Raschetti R, Santuccio C et al (2009) Hepatotoxicity from green tea: a review of the literature and two unpublished cases. Eur J Clin Pharmacol 65(4):331–341
Taylor JR, Wilt VM (1999) Probable antagonism of warfarin by green tea. Ann Pharmacother 33(4):426–428
Nishikawa M, Ariyoshi N, Kotani A, Ishii I, Nakamura H, Nakasa H et al (2004) Effects of continuous ingestion of green tea or grape seed extracts on the pharmacokinetics of midazolam. Drug Metab Pharmacokinet 19(4):280–289
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shakeel, M., Trinidade, A. & Ah-See, K.W. Complementary and alternative medicine use by otolaryngology patients: a paradigm for practitioners in all surgical specialties. Eur Arch Otorhinolaryngol 267, 961–971 (2010). https://doi.org/10.1007/s00405-009-1098-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-009-1098-1