
Abstract
The larynx is a secondary sex organ, and the hormone dependence of laryngeal carcinomas is considered an interesting matter of speculation. However, while tumors of other secondary sex organs, including the prostate, breast, and endometrium, have been recognized as hormone-dependent cancers, the laryngeal carcinomas are still subject to controversy. In this study, samples from 15 laryngeal carcinomas obtained at the time of surgery were assayed for specific estrogen alpha, progesterone, and androgen receptor expression, both at mRNA and protein levels. Detectable levels of specific estrogen and progesterone receptors, 53.3 and 73.3%, respectively, were found in the tumors. This positive detection by immunohistochemical analysis was higher in tumors than in normal mucosa adjacent to the tumor areas and was correlated with the absence of metastatic lymph nodes. No androgen receptor protein was detected in any sample analyzed, even if quantitative RT-PCR revealed high mRNA levels specific for this receptor. A strict correspondence between protein and mRNA hormone receptor levels was not found. This is in agreement with the transcriptional and protein synthesis mechanisms, and it is also compatible with the complex larynx tumorigenesis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Larynx cancer in Europe accounts for 2–5% of all cancers with about 45,900 new cases in 2006: 42,100 men and 3,800 women. It still represents the second most frequent neoplasm of the respiratory apparatus, secondary to pulmonary carcinoma. Its incidence has increased in the last few decades, and its peak incidence occurs among people in their sixties and seventies. Major risk factors for the development of this tumor are tobacco and alcohol consumption. Relative 5-year survival is about 63% but prognosis varies depending on the anatomical site (glottic cancer has a better prognosis) and the stage. Nearly 95% of all larynx cancers are squamous cell carcinomas.
This cancer has a male to female sex ratio of 11:1 in Europe, one of the highest among all cancer sites [1, 2]. It should be noted that the difference in susceptibility to larynx cancer based on gender has remained unchanged through the years in spite of the increasing tobacco and alcohol consumption among women [3–5].
The larynx is considered a secondary sexual organ. It is influenced by sexual hormones, not only during puberty but also during adulthood as it is subject to laryngeal epithelial layer modifications, cartilage metaplasia, and morphostructural changes [1, 5–7]. These considerations, in association with the peculiar epidemiological connotations, imply that endocrine factors can be involved in the carcinogenesis process, in particular the receptor status for sex hormones including estrogen, androgen, and progesterone receptors [7]. Even though a number of researchers have provided evidence in the last 20 years that sex hormone receptors are expressed in laryngeal carcinomas, the presently performed overall studies about the presence and the functional role of these receptors are, nevertheless, controversial.
In order to contribute to the gathered information about this issue, we present a perspective study on 15 patients with larynx cancer. The expression of estrogen receptor alpha (ERα), progesterone receptor (PR), and androgen receptor (AR) was analyzed at both protein and mRNA levels by immunocytochemistry and quantitative RT-PCR, respectively. The data obtained from neoplastic tissues were compared with those obtained from normal mucosa adjacent to the tumor areas. In addition, a correlation between the expression levels of these receptors and lymph node status was performed.
Materials and methods
Tissue specimens
Laryngeal cancer tissues were collected from 15 patients according to protocols approved by the Committee of Ethics in Research of the University. Surgical samples were collected from laryngeal tumor tissue and control regions (normal laryngeal tissue) of the same patient. Every sample was immediately divided into two parts. One part was fixed in 4–8% buffered formaldehyde and subjected to immunohistochemical analysis. The other part was immediately frozen in liquid nitrogen for RNA analysis.
The clinical data of the patients are reported in Tables 1 and 2.
Quantitative RT-PCR
Total RNA from fragments (0.5 mm) of laryngeal tumor and its normal counterpart tissue of the same patient was extracted using Total RNA Isolation System (Promega). Two micrograms of the total RNA was then used for double-stranded cDNA synthesis. It was reverse transcribed with the ImProm-II RT System (Promega). The mRNA of target genes was quantified by real-time PCR using ABI Prism 7700 system and the following TaqMan probes (Applied Biosystems):
-
5′ FAM-ATGATGAAAGGTGGGATACGAAAAG-TAMRA 3′ for ERα
-
5′ FAM-ATCATTGCCAGGTTTTCGAAACTTA-TAMRA 3′ for PR
-
5′ FAM-GGATGACTCTGGGAGCCCGGAAGCT-TAMRA 3′ for AR.
PCR was performed in a final volume of 25 μl. After a 10 min pre-incubation at 95°C, runs corresponded to 40 cycles of 15 s at 95°C (denaturation) and 1 min at 60°C (annealing/elongation). The mRNA levels of target genes were corrected for GAPDH mRNA levels (reference gene) and normalized to a calibrator sample as previously described [8].
Immunohistochemistry
Staining for ERα (clone 6F11, Ventana) and PR (clone 1A6, Ventana) was done on paraffin-embedded sections; immunohistochemical procedures were done with an automatic immunostaining device (Ventana XT Medical System, Tucson, AZ) and Ventana Kits (Strasbourg, France).
Immunohistochemistry of AR was performed as follows: sections of paraffin-tissues were deparaffinized and microwaved for antigen retrieval in Tris–EDTA–citrate pH 7.8. Subsequently, sections were incubated with mouse monoclonal primary antibody (AR clone AR411, DIAPATH), ready to use, at room temperature. Kit EN-VISION (DAKO) was then used for the detection of primary antibody. Staining was completed by incubation with 3,3′-diaminobenzidine as chromogen. The sections were counterstained with ematossilin for 2 min and washed again in PBS 1× (5 min).
Immunostaining was quantified with a Computerized Image Analysis System (Eureka-Menarini), and only cancer cells with distinct nuclear immunostaining for ERα, PR, and AR were recorded as positive.
The specificity of immunolabeling was verified in all experiments by controls in which the specific primary antibody was omitted.
Results
Characterization of the patients
A series of 15 patients was selected (14 men and one woman, average age 64 years, range 34–77 years). Thirteen patients were affected by primary laryngeal carcinoma while two were affected by recurrent laryngeal carcinoma (first treated by radiotherapy). The patients were selected so that we had access to sufficient tumor material for histopathological and biochemical analysis. Ten patients underwent a total laryngectomy and five a partial laryngectomy. Thirteen neck dissections were also performed.
Histological diagnosis of all analyzed samples was squamous cell carcinoma (SCC), predominantly of Grade 2 (moderately differentiated tumor) as reported in Table 1. Four subgroups (Table 2) were defined on the basis of tissue localization: about half of the cases were in the supraglottic area.
Sex hormone receptor expression
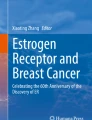
All paraffin-embedded tumors and their normal counterparts were tested for the presence of ERα, PR, and AR by immunocytochemical analysis. In all tumors and all normal tissues, we did not detect any specific nuclear positive staining for AR. On the contrary, ERα and PR proteins were detected at substantial levels. Immunohistochemistry demonstrated a particular nuclear ERα and PR positivity (Fig. 1), although cytoplasmic reaction was also detected at a lower frequency. Notably, the normal counterparts of SCC, obtained during surgery at the periphery of the resections, showed less sex hormone receptor reactivity by immunocytochemical analysis than the tumorous tissue. In fact, as reported in Table 3, the frequency of ERα and PR expression were higher in tumors compared to normal mucosa adjacent to the tumor areas (53.3 vs. 26.7%, and 73.3 vs. 60%, respectively).

Immunohistochemistry analysis of ERα, PR (D, E, F), and AR (G, H, I) steroid hormone receptors. A sample with predominant expression of ERα and PR in the tumor cells is shown. A, D Normal areas; B, E tumorous areas. No expression of AR is seen in any analyzed samples. In G a tumorous area is reported. The positive control tissue (prostate carcinoma) shows extensive immunostaining for AR (H). Original magnifications: ×20 and ×40. Control experiments carried out with omission of the primary antibody are also reported (C, F, I negative staining controls)
The results of protein expression were then correlated with the levels of mRNA for ERα, PR, and AR. Quantitative real time RT-PCR analysis was performed on the mRNA extracted from samples of fresh frozen normal and neoplastic tissues by using the TaqMan probes specific for ERα, PR, and AR transcripts as reported in the “Materials and methods” section. The sensitivity of the method was such that a very high percentage of transcription was detected in all cases, particularly for ERα and AR (Table 4). As expected, this indicates that a portion of mRNA is not translated into the corresponding protein. Concerning AR, the presence of such elevated mRNA levels without corresponding protein detection is very surprising. The same results were obtained in all five of the repeated experiments, and this is probably due to the altered characteristics of the tumor microenvironment that escape the normal control mechanisms of many molecular events.
In addition, as reported in Table 4, it is of note that in all three cases there were no significant differences at the transcription levels between tumors and their normal counterparts (see a representative plot in Fig. 2), suggesting that in the normal cells surrounding the tumor area, a tumorous behavior may be recognized at molecular levels.

Example of RT-PCR amplification plot monitored in real time. The threshold cycle (Ct) is the first cycle with detectable fluorescence in relation to an internal standard
When hormone receptor positivity was correlated with lymph node status, a significant correlation was detected between pN0 status and the expression of ERα and PR proteins (Fig. 3). In fact, in the ERα-positive or PR-positive cancer groups, the pN0 status was overrepresented.

Correlation between ERα and PR protein expression and lymph node status
Discussion
Currently, prognostic evaluation regarding head and neck squamous cell carcinomas is based mainly on tumor site, clinical stage (including lymph node involvement and the presence of distant metastasis), and histopathologic grade. Considering that laryngeal cancer has different epidemiological connotations between men and women (like incidence and clinical presentation and features), several studies since 1980 have analyzed the role of sex hormone receptors in the complex process of larynx tumorogenesis. Nevertheless, as previously reported, there is still no consensus about the presence and the functional role of these receptors in larynx carcinomas.
Schuller et al. [9] reported the evidence of low concentration levels of androgen and estro-progesterone receptors in laryngeal neoplasms, concluding that larynx cancer may not be considered a hormone-dependent neoplasm. In contrast with this study, Mattox et al. [10] have found positivity for androgens in 91% of the laryngeal neoplastic specimens examined from 23 patients, also recovering high hormonal levels in the lymph node metastases. Moreover, ten patients with advanced disease have been treated with flutamide, a powerful anti-androgenic, without satisfactory results [10]. Virolainen et al. [11] demonstrated the presence of androgen receptors in 31% of the evaluated laryngeal tumoral samples, estrogen receptors in 69%, and progesterone receptors in 53% of the cases without substantial differences between the sexes. Inconclusive results were obtained by Ferguson et al. [12] in 1987 using immunohistochemical analysis and by Vecerina-Volic et al. [13] in the same year, who described high androgen receptor levels represented in women correlated to male receptor levels in laryngeal cancer. Also, Toral et al. [14] considered larynx as an androgen target organ and correlated the larynx carcinomas to the loss of androgen receptors. In 1989, Berg et al. [15] supported the hypothesis of a possible hormonal therapy in the ENT district, describing the presence of progesterone receptors in laryngeal cancers as having similar characteristics to those identified in breast cancer. Other evidence supporting the presence and functionality of steroid hormone receptors, and in agreement with our results, comes from the inhibitory effect of antiestrogens on the growth of squamous-cell carcinoma cell lines from head and neck cancers [16, 17]. This suggests that antihormones such as tamoxifen may have a therapeutic role in laryngeal cancer expressing ER and PR [16, 17]. On the contrary, other research groups obtained the opposite results. Ogretmenoglu and Ayas [18] in 1998 were unable to recognize the clinical importance of estrogen expression in larynx carcinoma. In a more recent paper, Hagedorn and Nerlich [19] have associated the immunohistochemical technique to immunoenzymatic (the EIA) analysis evaluating ER, PR, and AR expression in normal and neoplastic specimens coming from patients affected by larynx carcinoma, demonstrating a complete lack of sex hormone receptors in their analysis. All of these controversial results indicate that growth and differentiation of head and neck squamous cell carcinomas are regulated by several factors and receptors and that a useful unique predictor of tumor aggressiveness has not yet been demonstrated. Nevertheless, the presence of estrogen receptors in a high proportion of laryngeal carcinoma cells suggests that hormonal therapy may be a useful adjunctive therapy in selected patients with cancer of the larynx. Therefore, it becomes imperative for the diagnostic histopathologist to test routinely for the presence of steroid hormone receptors on tumor tissues received in the laboratory. In addition, the employment of quantitative methods, such as those described here, may contribute to the understanding of the molecular mechanisms that sustain a specific larynx cancer phenotype.
The data obtained from our experiments show specific staining for ER alpha and PR but not for AR, even if high levels of mRNA for AR were detected. This ERα and PR positivity was significantly associated with the absence of lymph node metastasis. Taken together, the experiments suggest that ERα and PR could mediate estrogen- and progesterone-dependent changes during tumor progression in the larynx, and that their effects may anticipate or replace the action of AR, probably acting in combination with other factors. It is important to emphasize that several investigators employing high-throughput technologies have suggested that specific factors including E-cadherin, focal adhesion kinase (FAK), p53 protein, Ki-67 antigen, stomatin-like protein 2, VEGF, PTTG, stratifin, S100 calcium-binding protein A9, p21-ARC, stathmin, and enolase may play a critical role in the biology of head and neck squamous cell carcinomas [20–25] and may improve our ability to predict the clinical course of these tumors. These new findings will certainly help to increase our understanding of the role of sex hormones in the beginning and in the progression of the larynx tumor by analyzing possible unexplored crosstalk between different signaling pathways.
References
Licitra L, Bernier J, Grandi C, Locati L, Merlano M, Gatta G, Lefebvre JL (2003) Cancer of the larynx. Crit Rev Oncol Hematol 47:65–80
Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P (2007) Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 18:581–592
Andre K, Schraub S, Mercier M, Bontemps P (1995) Role of alcohol and tobacco in the aetiology of head and neck cancer: a case–control study in the Doubs region of France. Eur J Cancer B Oral Oncol 31:301–309
Jaber MA, Porter SR, Gilthorpe MS, Bedi R, Scully C (1999) Risk factors for oral epithelial dysplasia––the role of smoking and alcohol. Oral Oncol 35:151–156
Farshadpour F, Hordijk GJ, Koole R, Slootweg PJ (2007) Non-smoking and non-drinking patients with head and neck squamous cell carcinoma: a distinct population. Oral Dis 13(2):239–243
Vokes EE, Weichselbaum RR, Lippman SM, Hong WK (1993) Head and neck cancer. N Engl J Med 328:184–194
Hagedorn HG, Nerlich AG (2002) Analysis of sex-hormone-receptor expression in laryngeal carcinoma. Eur Arch Otorhinolaryngol 259:205–210
Lambertini E, Penolazzi L, Magaldi S, Giordano S, del Senno L, Piva R (2005) Transcription factor decoy against promoter C of estrogen receptor alpha gene induces a functional ER alpha protein in breast cancer cells. Breast Cancer Res Treat 92(2):125–132
Schuller DE, Abou-Issa H, Parrish R (1984) Estrogen and progesterone receptors in head and neck cancer. Arch Otolaryngol 110:725–727
Mattox DE, Von Hoff DD, McGuire WL (1984) Androgen receptors and antiandrogen therapy for laryngeal carcinoma. Arch Otolaryngol 110:721–724
Virolainen E, Tuohimaa P, Aitasalo K, Kytta J, Vanharanta-Hiltunen R (1986) Steroid hormone receptors in laryngeal carcinoma. Otolaryngol Head Neck Surg 94:512–517
Ferguson BJ, Hudson WR, McCarty KS (1987) Sex steroid receptor distribution in the human larynx and laryngeal carcinoma. Arch Otolaryngol Head Neck Surg 113:1311–1315
Vecerina-Volic S, Romic-Stojkovic R, Krajina Z, Gamulin S (1987) Androgen receptors in normal and neoplastic laryngeal tissue. Arch Otolaryngol Head Neck Surg 113:411–413
Toral I, Ciliv G, Gursel B, Ozdem C (1990) Androgen receptors in laryngeal carcinoma. Eur Arch Otorhinolaryngol 247:244–246
Berg NJ, Colvard DS, Neel HB 3rd, Weiland LH, Spelsberg TC (1989) Progesterone receptors in carcinomas of the upper aerodigestive tract. Otolaryngol Head Neck Surg 101:527–536
Shapira A, Virolainen E, Jameson JJ (1986) Growth inhibition of laryngeal UM-SCC cell lines by tamoxifen. Arch Otolaryngol Head Neck Surg 112:1151–1158
Grenman R, Virolainen E, Shapira A, Carey T (1987) In vitro effects of tamoxifen on UM-SCC head and neck cancer cell lines: correlation with the estrogen and progesterone receptor content. Int J Cancer 39:77–81
Ogretmenoglu O, Ayas K (1998) Laryngeal carcinoma and estrogen receptor analysis in patients after long-term follow-up. Eur Arch Otorhinolaryngol 255:457–461
Hagedorn HG, Nerlich AG (2002) Analysis of sex-hormone-receptor expression in laryngeal carcinoma. Eur Arch Otorhinolaryngol 259:205–210
Pastuszewski W, Dziegiel P, Krecicki T, Podhorska-Okolow M, Ciesielska U, Gorzynska E, Zabel M (2007) Prognostic significance of metallothionein, p53 protein and Ki-67 antigen expression in laryngeal cancer. Anticancer Res 27:335–342
Rodrigo JP, Dominguez F, Suarez V, Canel M, Secades P, Chiara MD (2007) Focal adhesion kinase and E-cadherin as markers for nodal metastasis in laryngeal cancer. Arch Otolaryngol Head Neck Surg 133(2):145–150
Cao WF, Zhang LY, Liu MB, Tang PZ, Liu ZH, Sun BC (2007) Prognostic significance of stomatin-like protein 2 overexpression in laryngeal squamous cell carcinoma: clinical, histologic, and immunohistochemistry analyses with tissue microarray. Hum Pathol 38(5):747–752
Onesto C, Hannoun-Levi JM, Chamorey E, Formento JL, Ramaioli A, Pages G (2006) Vascular endothelial growth factor-A and Poly(A) binding protein-interacting protein 2 expression in human head and neck carcinomas: correlation and prognostic significance. Br J Cancer 94(10):1516–1523
Solbach C, Roller M, Eckerdt F, Peters S, Knecht R (2006) Pituitary tumor-transforming gene expression is a prognostic marker for tumor recurrence in squamous cell carcinoma of the head and neck. BMC Cancer 6:242
Sewell DA, Yuan CX, Robertson E (2007) Proteomic signatures in laryngeal squamous cell carcinoma. ORL J Otorhinolaryngol Relat Spec 69(2):77–84
Acknowledgments
This research was supported by grants from Fondazione Cassa di Risparmio di Ferrara. English revision of the article was carried out by Rebecca K. Swartz.
Author information
Authors and Affiliations
Corresponding author
Additional information
Chiara Bianchini and Elena Torreggiani equally contributed to the paper.
Rights and permissions
About this article
Cite this article
Bianchini, C., Pastore, A., Pelucchi, S. et al. Sex hormone receptor levels in laryngeal carcinoma: a comparison between protein and RNA evaluations. Eur Arch Otorhinolaryngol 265, 1089–1094 (2008). https://doi.org/10.1007/s00405-008-0589-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-008-0589-9