
Abstract
Follicular dendritic cell sarcomas are unusual, and extranodal origin is extremely rare. The English literature contains only eight cases in which this sarcoma has been presented as a tonsillar mass. We report a new case of follicular dendritic cell sarcoma of the tonsil in a 76 year old woman. The patient underwent diagnostic tonsillectomy for a left tonsillar mass, and follicular dendritic cell sarcoma was diagnosed based on histopathological and immunoperoxidase findings. Postoperative radiotherapy was performed. The patient is alive and disease-free at 4 years of follow-up. Without a high index of suspicion, this entity can easily be missed. We believe that follicular dendritic cell sarcoma should be included in the differential diagnosis for any tonsillar mass.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Follicular dendritic cells, such as interdigitating dendritic cells and Langerhans cells, are non-lymphoid, non-phagocytic accessory cells of the lymphoid system that trap and present antigens and immune complexes. They are normally found in the germinal centers of primary and secondary follicles, and form a tight meshwork with other cells. In routinely prepared sections, these cells feature fibrillary pale cytoplasm, indistinct cell membranes, round nuclei with fine chromatin, and small nucleoli [4]. They may also be multinucleated [8]. Follicular dendritic cells have complement receptors and human leukocyte antigen-DR on their surface, and can be identified immunohistochemically. They are consistently positive for CD21 (C3d receptor), CD35 (C3b receptor), CD23, Ki-M4, Ki-M4p, CNA 42, R4/23, Ki-FDC1p, desmoplakin, and low-affinity growth factor; they are variably positive for vimentin, EMA, S-100 protein, CD68, actin, and leukocyte common antigen [4, 8].
Follicular dendritic cell sarcoma (FDCS) was first described in 1986 by Monda et al., and fewer than 70 cases have been reported. Most documented cases of FDCS have been in lymph nodes; less than one-third have been extranodal [1, 6]. To date, only eight FDCS of the tonsil have been reported in the English literature [1–8].
Case report
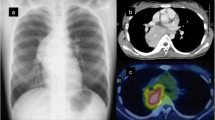
A 76-year-old woman was referred to our otorhinolaryngology department for investigation of a mass in her left tonsil that had been detected during a routine check-up. The patient had been unaware of the mass and had no symptoms. The ENT examination revealed a swollen, enlarged, indurated left tonsil that featured necrotic ulcerative areas and was covered with a grayish–white membrane. The tonsil was not painful to touch and was firm and elastic on palpation. Neck examination revealed no enlarged lymph nodes. Computed tomography revealed a 3.5 × 3.5 × 1.5 cm mass in the left tonsillar fossa. The lesion enhanced with contrast injection. The presumptive diagnosis was tonsillar lymphoma, and diagnostic left tonsillectomy was performed. The right tonsil was not enlarged and was not removed. There was no gross evidence of residual tumor in the left tonsillar fossa after surgery.
Histopathological examination of the removed tonsil revealed that the tonsillar tissue had been totally replaced by infiltrating neoplastic tissue. The tumor was composed of spindle cells arranged in storiform pattern and multinucleate giant cells, and there were areas of coagulation necrosis (Fig. 1). Immunohistochemical staining showed that the tumor cells were positive for CD21 and vimentin, partially positive for CD68 and S-100 protein, and negative for cytokeratin (Fig. 2).

A section of tumor tissue featuring spindle cells forming whorls, multinucleated giant cells and showing areas of coagulation necrosis. An illustration of higher magnification is included. (Hematoxylin and Eosin)

The tumor cells stained positive for CD21
Based on the histopathological and immunohistochemical findings, the patient was diagnosed with FDCS of the tonsil. Examination of the tumor tissue revealed poor prognostic criteria, including high mitotic index, nuclear pleomorphism, and multifocal coagulation necrosis. Subsequent staging with computed tomography of the neck and thorax, abdominal ultrasonography, and bone scanning revealed no regional or distant metastasis. Since resection had achieved only a small tumor-free margin and since this intermediate-grade malignancy is associated with high risk of local recurrence, we prescribed radiotherapy at the primary site as adjunctive therapy. Postoperative Cobalt-60 radiotherapy of 5,000 cGy with 200 cGy fractions delivered over 25 days was applied to the left tonsillar region. The patient is still alive and disease-free 4 years after surgery.
Discussion
Although this entity was originally known as “follicular dendritic cell tumor,” Chan et al. [3] proposed the name “follicular dendritic cell sarcoma” to emphasize the clinical behavior of the neoplasm as a sarcoma rather than a lymphoma. FDCS has generally been considered an indolent tumor with low risk for metastasis but a tendency for local recurrence; however, more recent reports indicate that this neoplasm is more aggressive and should be considered at least an intermediate-grade malignancy [1, 3, 7]. The overall rates of recurrence, metastasis, and mortality for cases of FDCS are 43, 24, and 17%, respectively. The common sites of metastasis are the liver, peritoneum, pancreas, lymph nodes and lung [3]. Large tumor size (>6 cm diameter), intra-abdominal location, presence of coagulation necrosis, high mitotic index (>5 mitoses per 10 high-power fields), moderate nuclear pleomorphism, and lack of adjuvant therapy are associated with poor prognosis [3]. FDCS has been linked with Epstein–Barr virus and with hyaline vascular-type Castleman disease, but they are rarely associated with FDCS of the head and neck region [1].
As mentioned, the literature contains only eight cases of FDCS of the tonsil. Three had follow-up periods of 12 months or less, and all three of these patients had small tumors that were treated successfully by surgery alone [1, 7]. Another patient with a small tumor was treated with tonsillectomy alone and was tumor-free after 3 years of follow-up [3]. A fifth case was managed with tonsillectomy and adjuvant radiotherapy, and the patient was disease-free 5 years later [8]. Sixth patient with FDCS of the tonsil and a metastatic lymph node in the neck was treated with tonsillectomy, radical neck dissection, and adjuvant radiotherapy, and this individual was alive with no recurrence after 3 years of follow-up [4]. Seventh case of large FDCS was managed with tonsillectomy followed by postoperative radiotherapy, and the patient had local recurrence and cervical lymph node metastasis 4.5 years later [3]. The eighth patient was treated with tonsillectomy followed by chemotherapy, but was lost to follow-up after chemotherapy was started [3].
The differential diagnosis for FDCS includes ectopic meningioma, interstitial reticulum cell sarcoma, and lymphoepithelial carcinoma. Ectopic meningioma closely mimics FDCS, as both these tumors feature syncytial cells that form whorls and the tumor cells are negative for cytokeratin. However, meningiomas do not contain lymphocytes and are negative for CD21, CD68, and CD35. Interstitial reticulum cell sarcomas have a syncytial cell structure that resembles that of FDCS, but their cells are cytokeratin-positive and are negative for CD21 and CD35. Lymphoepithelial carcinomas also feature syncytial cells, vesicular nuclei containing prominent nucleoli, as well as lymphocytes Thus, these tumors can be misdiagnosed as FDCS, but they are infiltrative as opposed to having pushing borders, and their cells do not form whorls and are cytokeratin-positive.
FDCS should be included in the differential diagnosis for any tonsillar mass. If this tumor is suspected based on histological appearance, it is necessary to do immunohistochemical staining aimed at identifying follicular dendritic cell differentiation. This is vital to avoid misdiagnosis. Correct diagnosis of this neoplasm is extremely important because of the risks of recurrence and metastasis.
References
Biddle DA, Ro JY, Yoon GS, Yong YW, Ayala AG, Ordonez NG, Ro J (2002) Extranodal follicular dendritic cell sarcoma of the head and neck region: three new cases, with a review of the literature. Mod Pathol 15:50–585
Chan JK, Tsang WY, Ng CS, Tang SK, Yu HC, Lee AW (1994) Follicular dendritic cell tumors of the oral cavity. Am J Surg Pathol 18:148–157
Chan JK, Fletcher CD, Nayler SJ, Cooper K (1997) Follicular dendritic cell sarcoma. Clinicopathologic analysis of 17 cases suggesting a malignant potential higher than currently recognized. Cancer 15(79):294–313
Dominguez-Malagon H, Cano-Valdez AM, Mosqueda-Taylor A, Hes O (2004) Follicular dendritic cell sarcoma of the pharyngeal region: histologic, cytologic, immunohistochemical, and ultrastructural study of three cases. Ann Diagn Pathol 8:325–332
Galati LT, Barnes EL, Myers EN (1999) Dendritic cell sarcoma of the thyroid. Head Neck 21:273–275
Monda L, Warnke R, Rosai J (1986) A primary lymph node malignancy with features suggestive of dendritic reticulum cell differentiation. A report of 4 cases. Am J Pathol 122:562–572
Perez-Ordonez B, Erlandson RA, Rosai J (1996) Follicular dendritic cell tumor: report of 13 additional cases of a distinctive entity. Am J Surg Pathol l20:944–955
Tisch M, Hengstermann F, Kraft K, von Hinuber G, Maier H (2003) Follicular dendritic cell sarcoma of the tonsil: report of a rare case. Ear Nose Throat J 82:507–509
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aydin, E., Ozluoglu, L.N., Demirhan, B. et al. Follicular dendritic cell sarcoma of the tonsil: case report. Eur Arch Otorhinolaryngol 263, 1155–1157 (2006). https://doi.org/10.1007/s00405-006-0124-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-006-0124-9