
Abstract
Hearing loss is one of the most common chronic health conditions and has important implications for the patient’s quality of life. However, hearing loss is substantially underestimated and under treated. The purpose of this study was to determine the prevalence of sensorineural hearing loss among the workers in a steel rolling mill in Nigeria. Each of the 150 randomly selected subjects had a structured questionnaire administered to them, followed by a full otological examination. Of these, 116 had tympanometry and pure-tone audiometry. Also a noise mapping of their respective work units was done. The workers were exposed to noise levels varying from 49 to 93 dBA. About 28.2% of the 103 who had their audiogram analysed had mild to moderate sensorineural hearing loss in their better ear and 56.8% of them had mild to moderate sensorineural hearing loss in their worse ear. The pure-tone average and the average hearing thresholds at 4 kHz for the groups significantly increased with an increasing noise exposure level. The prevalence of sensorineural hearing loss among the study population is high; and noise exposure is at least contributory. Pre-employment and regular audiometry while on the job is highly recommended.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hearing loss is one of the most common chronic health conditions and has important implications for the patient’s quality of life. However, hearing loss is substantially underestimated and under treated [1, 2].
Exposure to excessive noise is the major avoidable cause of permanent hearing impairment worldwide [3, 4]. Noise induced hearing loss (NIHL) is rated among the top ten work related problems, and as the most prevalent irreversible industrial disease and the biggest compensatable occupational hazard [1, 4, 5].
The WHO program for the prevention of deafness and hearing impairment (PDH) is especially targeted at developing countries where there is a serious lack of accurate population-based data on the prevalence and causes of deafness and hearing impairment, NIHL inclusive [4, 6, 7].
The purpose of this study was to determine the prevalence of sensorineural hearing loss among the noise exposed and the non-noise exposed workers in a steel rolling mill in Nigeria.
Materials and methods
A random sample of 150 steel rolling-mill workers was selected from all sections (including non-production areas) based on a sampling fraction of one fourth, i.e. one of every four workers (workers in each unit were serially numbered and every fourth worker was included in the study). They were initially screened to exclude subjects with pathological external and middle ear as well as those currently working in sections classified as non-noise but who had been exposed to excessive noise in the past.
Each subject had an interview questionnaire administered to obtain their, socio-demographic data and background occupational experience. Then they had an otological examination, including otoscopy using a dry cell operated auroscope to rule out the presence of any significant aural pathological conditions. Through this 34 subjects were excluded from the study: 14 for chronic suppurative otitis media, four for scarred tympanic membrane, four for dull tympanic membrane, three for retracted tympanic membrane and nine for impacted cerumen that could not be immediately evacuated.
The remaining 116 subjects with apparently normal external and middle ears then had tympanometry using impedance audiometer AT 235 employing standard procedure [8].
They also had conventional frequency (0.25–8 kHz) audiometry using a duly calibrated diagnostic audiometer, Danplex AS 67 in a quiet room in the factory clinic (sound level about 36 dBA) [6, 9], employing standard procedure [8]. (For logistic reasons, subjects could not be transferred to our hospital for audiometry in a sound proof booth. Although this is less than optimal, it is acceptable given the measured sound level and a recent observation of the significant agreement between hearing thresholds measured in non-soundproof working environments and soundproof booth [9].) Thirteen other subjects were excluded on grounds of abnormal tympanogram and/or conductive hearing loss. Thus, 103 subjects had their audiogram results analysed.
The current noise exposure of the workers was estimated using sound level meter Testo 815 (Testo GmbH & Co. Lenzkirch, Germany) on a decibel-A (dBA) scale duly calibrated with a sound level meter calibrator, Testo 0554.0009(Testo GmbH & Co. Lenzkirch, Germany) [10, 11] The microphone of the sound level meter was positioned at the ear level of the workers in each unit [12]. Readings were taken when the sound level became steady for at least 10 s. The average of eight essentially constant hourly readings between 9.00 am and 4.00 pm was calculated.
The subjects were divided into four groups based on the average noise levels observed at their worksites (93, 86, 72 and 49 dBA).
Pure-tone average was calculated for frequencies 0.5–4.0 kHz [13] and pure-tone averages were classified into one of the following hearing loss categories: mild 26–40 dBHL, moderate 41–70 dBHL, severe 71–95 dBHL and profound > 95 dBHL [13].
The data generated was analysed using EPI-INFO Version 6.04 computer software. Differences were considered significant when P < 0.05.
The study protocol was approved by our university teaching hospital ethics committee. The consent of the management of the steel rolling mill and individual subject consent were sought and obtained.
Results
One hundred and three workers, 96 (93.2%) males, mainly in the fourth (25.2%) and fifth (58.3%) decades of life were enrolled in this study. About two-thirds of them have tertiary education. Twenty-eight (27.2%) work in the administrative area (average sound level of 49 dBA); 18 (17.5%) in the mechanic/maintenance workshop (72 dBA); 44 (42.7%) mill floor production area (86 dBA); and 13 (12.6%) finishing stage production area (93 dBA). About 90% of the respondents have been working in this factory for 10–29 years (mean 16.0 years ± SD 5.00) and they have spent a mean of 12 years ± SD 6.81 working in their current units (Table 1). All workers except four work for 8 h a day, 5 days of the week.
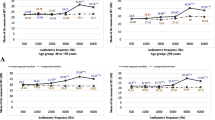
About 28.2% of the 103 who had their audiogram analysed had mild to moderate sensorineural hearing loss in their better ear and 56.8% of them had mild to moderate sensorineural hearing loss in their worse ear (Table 2). The average hearing threshold at 4 kHz for the groups increased with an increasing noise exposure level; so also was the pure-tone average. The relationship were statistically significant (Tables 3, 4)
The pure-tone average of the subjects increased with an increasing length of exposure, except at the extremes that have disproportionately few subjects. The relationship was statistically significant (Table 5).
Also the relationship between the pure-tone average and the awareness of exposure to noise was statistically significant (Table 6).
Discussion
Humans show differing susceptibility to noise damage even under very carefully controlled exposure conditions [14]. This difference in susceptibility may be related to unknown genetic components [14]. At 80 dBA there is no material risk in the vast majority of individuals [15]. At 85 dBA there is a marginal risk with susceptible individuals accruing hearing impairment from a life-time of exposure [15]. Many authorities agree that regulations regarding risk from exposure to noise at work entail action at levels of 85 dBA and above [5, 10, 15]. At 90 dBA and above the risk of NIHL becomes material, with the majority of individuals accruing a significant hearing impairment [15]. Generally, the prevalence of hearing loss increases with an increasing noise level exposure [10, 16, 17].
No one in the study population had a pre-employment pure-tone audiometry to determine his baseline-hearing threshold. This study was the first of such tests for nearly all of them. While the blame for the failure to test their hearing can be laid on the individual workers or their employers, the fact is that there are few facilities and personnel for audiological assessment in our environment. Although, there is a gradual improvement already, NGOs could complement the efforts of the government to establish audiological facilities in developing countries [6].
At the time of this test 28.2% of the study population already had mild to moderate sensorineural hearing loss in their better ear and 56.8% in their worse ear. How much of this is attributable to their present employment is difficult to determine since there was no pre-employment audiometry. Pre-employment medical test is already an entrenched procedure in most organisations. Insistence on the inclusion of pure-tone audiometry is recommended particularly in employments associated with harmful noise. Also regular audiometry screening while on the job, say yearly, is useful in detecting early sensorineural hearing loss so that such workers are quickly reassigned to less hazardous areas or the noise level in the working area can be put under control. In this respect otoacoustic emission measurement is more sensitive than conventional pure-tone audiometry in monitoring employees with early NIHL [18–20]. Also, otoacoustic emission measurements may be useful in differential diagnosis of occupational NIHL from other diseases with cochlear hearing loss such as ototoxicity and presbyacusis with similar audiogram pattern [21].
In this study population there is ample evidence that noise is probably responsible for the high prevalence of sensorineural hearing loss. There was a statistically significant difference in the pure-tone average of the subjects when correlated with the noise level they were exposed to [10, 16, 17, 22]. Also, workers with prolonged stay in their noisy departments had significantly increased pure-tone average [2, 11, 16, 17, 23, 24]. The relationship between awareness of exposure to noise and pure-tone average was statistically significant [10]. Importantly the average threshold at 4 kHz, known to be the most sensitive to noise damage [9–11, 16], increased with higher noise exposure. So, where possible efforts should be made to reduce the noise from factory machines by technological innovation in their manufacturing, regular maintenance, or isolation of these machines from direct human contacts. Also, ear protection from harmful noise should be rigorously pursued.
We can conclude that the prevalence of sensorineural hearing loss is high in our study population and noise exposure is at least contributory. We recommend pre-employment and regular audiometry while on the job with otoacoustic emission measurements where possible. These will become feasible if there is provision of more audiological assessment centres and enforceable legislation to that respect. Also, periodic inspection by occupational hygiene officers to monitor compliance with industrial noise safety standards is advocated. In this way other possible aetiology of sensorineural hearing loss among the population could be identified and managed.
References
Borchgrevink H (2003) Does health promotion work in relation to noise? Noise Health 5(18):25–30
Palmer KT, Griffin MJ, Syddall HE, Davis A, Pannett B, Coggon D (2002) Occupational exposure to noise and the attributable burden of hearing impairment in Great Britain. Occup Environ Med 59(9):634–639
Hallberg LR (1996) Occupational hearing loss: coping and family life. Scand Audiol Suppl 43:25–33
Smith AW (1998) The World Health Organisation and the prevention of deafness and hearing impairment caused by noise. Noise Health 1(1):6–12
Brink LL, Talbott EO, Burks JA, Palmer CV (2002) changes over time in audiometric thresholds assembly workers with a hearing conservation program. AIHA J 63(4):482–487
World Health Organisation (1997) Prevention of noise induced hearing loss. Report of a WHO-PDH informal consultation, Geneva, 28–30 Oct 1997. No 3 in the series “Strategies for prevention of deafness and hearing impairment”; WHO|PDH|98.5
Akande TM, Ologe FE (2003) Noise induced hearing loss (NIHL) in the middle belt of Nigeria. Postgraduate Doctor Africa 25(4):81–82
O’connor AF (1997) Examination of the ear In: Kerr AG, Booth JB (eds) Scott Brown’s otolaryngology: otology 6th edn. Butterworth/Heineman, Oxford, pp 3/1/1–3/1/29
Wong TW, Yu TS, Chen WQ, Chiu YL, Wong CN, Wong AH (2003) Agreement between hearing thresholds measured in non-soundproof work environments and a sound proof booth. Occup Environ Med 60(9):667–671
Ahmed HO, Dennis JH, Badran O, Ismaikl M, Ballah SG, Ashoora, Jerwood D (2001) Occupational noise exposure and hearing loss of workers in two plants in Eastern Saudi Arabia. Ann Occup Hyg 45(5):371–380
Nguyen AL, Nguyen TC, Van TL, Hoang MH, Nguyen S, Jonai H, Villanneva MB, Matsuda S, Sotoyama M, Sudo A (1998) Noise levels and hearing ability of female workers in a textile factory in Vietnam. Ind Health 36(1):61–65
Tanaka M, Shimai S, Nakamura K, Takahashi H, Tanaka K (1992) Investigation of noise in a factory. Ann Physiol Anthropol 11(1):21–27
Campbell K (1998) Basic audiologic assessment. In: Dauhaeur J (eds) Essential audiology for physicians. 1st edn. Singular Publishing Ltd, London, pp 1–11
Davis RR, Kozel P, ERway LC (2003) Genetic influences in individual susceptibility to noise: a review. Noise Health 5(20):19–28
Lutman ME (2000) What is the risk of noise-induced hearing loss at 80, 85, 90 dB(A) and above? Occup Med (Lond) 50(4):274–275
Osibogun A, Igweze JA, Adeniran LO (2000) Noise-induced hearing loss among textile workers in Lagos metropolis. Niger Postgrad Med J 7(3):104–111
Shakhatreh FM, Abdul-Baqi KJ, Turk MM (2000) Hearing loss in a textile factory. Saudi Med J 21(1):58–60
Ahias J, Bresloff I (1996) Noise induced temporary otoacontic emission shifts. J Basic Clin Physiol Pharmacol 7(3):221–233
Marshall L, Lapsley Miller JA, Heller LM (2001) Distortion–product otoaconstic emissions as a screening tool for noise induced hearing loss. Noise Health 3(12):43–60
Sliwinska-Kowalska M, Kotylo P (1997) Otoacoutic emission useful in the differential diagnosis of occupational noise-induced hearing loss? Med Pr 48(6):613–620
Zhang Y, Zhang X, Zhu W, Zheng X, Deng X (2004) Distortion product of otoacoustic emissions as a sensitive indicator of hearing loss in pilots. Aviat Space Environ Med 75(1):46–48
Oleru UG (1980) Comparison of the hearing levels of Nigerian textile workers and a control group. Am Ind Hyg Assoc J 41(4):283–287
Oleru UG, Ijaduola GT, Sowho EE (1990) Hearing thresholds in an autoassembly plant: prospects for hearing conservation in a Nigerian factory. Int Arch Occup Environ Health 62(3):199–202
Palmer KT, Griffin MJ, Syddall HE, Davis A, Coggon D (2004) Cigarrette smoking, occupational exposure to noise and self reported hearing difficulties. Occup Environ Med 61(4):340–344
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ologe, F.E., Akande, T.M. & Olajide, T.G. Occupational noise exposure and sensorineural hearing loss among workers of a steel rolling mill. Eur Arch Otorhinolaryngol 263, 618–621 (2006). https://doi.org/10.1007/s00405-006-0043-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-006-0043-9