
Abstract
Computerised tomography (CT) scans are routinely performed prior to endoscopic sinus surgery (ESS) in order to confirm the diagnosis, assess the response to medical treatment and provide important landmarks for surgery. However, the correlation between the findings of CT scans and the patient’s symptoms remains ambiguous. The objective was to assess the correlation between preoperative symptom scores using the validated Sino-Nasal Assessment Questionnaire and CT scores in patients undergoing ESS. Twenty-two patients who attended otolaryngology clinics with chronic rhinosinusitis (CRS) were prospectively enrolled in the study. All of these patients completed Sinonasal Questionnaires (SNAQ) before they had ESS. Their CT scans were scored blindly by the surgeon and a radiologist following Lund-Mackay grading. Patients with high preoperative SNAQ scores had high or low CT scores. The same applied for patients with low preoperative SNAQ scores. There was no statistically significant correlation between SNAQ and Lund-Mackay scores ( P =0.5). However, there was a very strong correlation ( P <0.001) between the scoring of scans by the surgeon and the radiologist, while there was a moderate degree of discrepancy in the grading of anterior ethmoid sinuses and osteo-meatal complexes. Morbidity of patients with CRS cannot be predicted from the magnitude of changes in their CT scans. Significant inter-rater variability exists in the grading of pathological changes in anterior ethmoid sinus and osteo-meatal complex as recorded in CT scans.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic rhino-sinusitis is a one of the most common reasons for attendance of an Otolaryngology clinic. It has been estimated that 10 to 15% of the population in central Europe is affected annually with CRS [1]. Nasal polyposis, which is very commonly associated with CRS, has an incidence of 33,000 new cases per year in England and Wales [2]. Surgery in the form of ESS is the procedure of choice for patients who fail to respond to medical treatment [3]. A CT scan of the paranasal sinuses is invariably indicated prior to surgery [4]. The importance of CT scanning in CRS lies in demonstrating the extent of disease and any variation from normal anatomy that may predispose to surgical or CRS-related complications [5, 6, 7].
Sino Nasal Questionnaire (SNAQ) form 11 is a recently developed questionnaire comprised of 11 questions, each graded between 0 and 5, which produce a total symptom score ranging between 0 and 80. (Table 1) The difference from the more widely used Sino-Nasal Outcome Test (SNOT 20) questionnaire lies in its ability to assess a wider variety of symptoms and to measure more subtle changes. Both of these features render it more sensitive to change following surgery, as demonstrated by Fahmy et al. [8]. Compared to the General Nasal Patient Inventory (GNPI), another nasal outcome instrument, SNAQ grading is more rhinosinusitis-specific. It gives more prominence to symptoms that characterise rhinosinusitis (such as nasal obstruction) than non-specific symptoms (such as ear fullness/pressure). Also GNPI, comprising 45 items, is too lengthy for the patients to fill, thus resulting in reduced compliance [8, 9].
The Lund-Mackay scoring system [10] is a system of grading changes in CT scans in patients with CRS. It achieves the highest level of both intra- and inter-observer agreement without being time-consuming, when compared with the scoring systems of Jorgensen, May and Levine or Newman [5].
In our study, we evaluated the preoperative symptom scores and CT scans of 22 patients about to undergo ESS for CRS. Our aim was to find out whether any correlation exists between the degree and severity of symptoms as assessed by the SNAQ questionnaire and CT scan changes as graded by the Lund-Mackay scoring system, as well as assess the inter-rater variability in scoring CT scans.
Materials and methods
Twenty-two patients attending the otolaryngology outpatient department and diagnosed with CRS were prospectively invited to participate in this study. Informed consent was obtained in all cases. All the patients were suffering from CRS as confirmed by their history, symptoms, clinical and endoscopic findings. We used the current definition of CRS [4], which is based upon the persistence for more than 12 weeks of two or more major sinus symptoms or at least one major and two minor symptoms. Major criteria include facial pain, nasal congestion, nasal obstruction, hyposmia or anosmia as well as purulence of the nasal cavity on examination. Minor criteria include headache, fever, halitosis, fatigue, dental pain, cough and ear pain or pressure.
Exclusion criteria included history of previous ESS and associated pathology requiring an additional procedure—for example, polypectomy and septoplasty, so as not to contaminate the preoperative symptom assessment. All patients were treated with a steroid nasal spray, with an initial short course of steroid nasal drops and a longer course of antihistamines if there was evidence of allergy. When there was suggestion of an infection (streaming of pus from the middle meatus, mucosal cobble-stoning), antibiotics were added. All patients were followed up in clinics for a period of 3 to 6 months. Non-responders of medical treatment were asked to fill out SNAQ forms and listed for ESS. CT scans of paranasal sinuses were done prior to surgery.
Computerised tomography scans were performed using 5-mm ultra-high-resolution coronal slices using a bone setting, (4,000 width and 350 centre Hounsefield units). All CT scans were scored following the Lund-Mackay system, separately by the surgeon who performed the ESS and one consultant radiologist. At the time of scoring, both raters were blinded to the patients’ SNAQ scores. According to the Lund-Mackay system, each side of the paranasal sinuses (right and left) is scored separately. The ethmoid sinus is divided into anterior and posterior. Score 0 signifies no abnormality, score 1 partial and score 2 total opacification. Osteo-meatal complexes are scored as either 0 (not obstructed) or 2 (obstructed). The total score can range from 0 to 24. All results were analysed using SPSS 10. Pearson correlation coefficients were used to evaluate the correlation between continuous variables.
Results
The mean Sino Nasal Assessment Questionnaire score was 47.2 (standard deviation 9.2, range 25 to 60). The mean Lund-Mackay sinus score as assessed by the surgeon was 15.5 (SD 5.5, range 5 to 24) and as assessed by the radiologist was 13.5 (SD 5.7, range 5 to 24). Thus, the averaged Lund-Mackay sinus score was 14.5 (SD 5.5, range 5.5 to 24).
SNAQ scores and CT scores for individual patients are shown in Table 2. Patients with high SNAQ scores had high or low CT scores and vice versa, while patients with the same SNAQ score had wide differences in their CT scores. For example, patients whose SNAQ scores were more than 50 had their CT scores ranging form 5.5 to 18, while patients with SNAQ scores between 40 to 50 had CT scores that ranged from 7.5 to 24. Patients with low SNAQ scores (25 to 40) had CT scores ranging anywhere from 7 to 22.5. (Fig. 1)

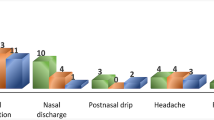
Total (cumulative) score for each sinus as graded by the surgeon and the radiologist using the Lund-Mackay grading system
Statistical analysis confirmed that there was no correlation between SNAQ scores and CT scores (Pearson correlation coefficient 0.152, P =0.5) (Fig. 2)

Patients’ averaged Lund-Mackay scores and SNAQ scores
In contrast to the discrepancy between SNAQ and CT findings, the correlation between the scoring of CT scans by the radiologist and surgeon was very good (Table 3, Fig. 3). Except for the anterior ethmoid (left) and osteo-meatal complex, the scoring by the surgeon was within a maximum three-point difference from the radiologist’s scoring. (except for right sphenoid sinus, which has a difference of five). This excellent inter-rater agreement is confirmed statistically (Pearson correlation coefficient 0.930, P <0.0001). Interestingly, when there was a difference between the two scorings, the surgeon’s grading was generally more pessimistic than the radiologist’s.

Radiologists’ and surgeons’ Lund-Mackay grading of CT scans
Discussion
This study was designed to find out the correlation between patients’ symptoms and their preoperative CT scans’ changes. As one of these is a subjective (symptom score) and the other an objective (CT score) tool to assess CRS, their combination could provide an ideal way to help surgeons understand and grade the disease’s severity in patients and thus to prioritise them for surgery. Previous studies on this subject have failed to arrive at a uniform conclusion. One of these studies has shown that CT scans are more accurate at diagnosing CRS than subjective symptoms [11], while failing to demonstrate any correlation between the two. Similar results have been found in another, earlier study [12]. However, both of these studies suffered from the limitation that symptoms were not assessed using a validated questionnaire. To our knowledge, no correlation study between CT findings and clinical symptoms using the SNAQ questionnaire has been published to date. However, despite our use of a validated, highly sensitive questionnaire, we could not find any correlation between the patients’ subjective symptoms and the CT scans, as graded using the Lund-Mackay scoring system. There was a wide variation of symptom scores for essentially similar stages of disease, as recorded in the scans. This is more true for patients with relatively few findings on the CT scans and L-M scores of less than 10. On the other hand, patients with high scores over 15 tended to display more consistently high symptom scores. This could be a result of different patient reactions and interpretations of symptoms, with different patients showing a higher threshold to pain or other nasal symptoms. However, it also demonstrates that CT scans are inadequate as a sole instrument for the assessment and grading of this complex disease process. Endoscopic findings, the evolution of symptoms and findings over time are probably more accurate ways to assess morbidity and disease activity.
Another interesting outcome of this study was the comparison of CT scoring between a surgeon and a radiologist following the Lund-Mackay system. Overall, there was quite a good correlation between the grading by the radiologist and the surgeon, with minimal inter-rater variability. It is interesting, however, to note that when there was a difference in their respective grading, the surgeon consistently over-rated the scans, with 15 patients allocated a higher score by a surgeon versus only 2 by a radiologist. Analysing grading by sinuses, we can see that anterior ethmoids, sphenoids, frontal and maxillary sinuses were all overrated by the surgeon. The biggest discrepancy, however, was recorded in the grading of the osteomeatal complex where in many occasions its patency was contested between the surgeon and the radiologist, the radiologist recognizing that it was patent when the surgeon scored it as blocked.
We understand that there were some shortcomings in our study: It was designed as a pilot study, and consequently our study population was rather small. In fact, the number was too small to claim to be a clinical tool to find out the correlation between patients’ symptoms and their preoperative CT scan changes. The average interval of time between the day of CT scan and the day of filling up of SNAQ for any patient was 3 months. To be able to compare the SNAQ-results with the CT scans, both should be correlated in time so that neither of these can be influenced by ongoing intercurrent upper respiratory disease. However, we feel that this pilot work can initiate further studies on this subject, which can help us better understand the complex pathophysiology of CRS.
References
Gravers G, Klemens A (2002) Rhinosinusitis. Current diagnostic and therapeutic aspects. MMW Fortschr Med 144:31–35
Claire Hopkins, John Browne, Robert Slack (2004) The national comparative audit for nasal polyposis and chronic sinusitis. ENT News 12:47–48
Bhattacharya N (1999) Computed tomographic staging and the fate of the dependent sinuses revision endoscopic sinus surgery. Arch Otolaryngol Head Neck Surg 125:994–999
Chow JM, Stankiewicz JA (2002) A diagnostic dilemma for chronic rhinosinusitis: definition accuracy and validity. Am J Rhinol 16:199–202
Gardiner Q, Oluwole M, Russell N, Tan L, White P (1996) A comparison of computerised tomographic staging systems in chronic sinusitis. Clin Otolaryngol 21:91–95
Kennedy DW, Rosenbaum AE, Zinreich SJ (1987) Paranasal sinus CT imaging requirements for endoscopic surgery. Radiology 163:769–775
Cowan IA, Robertson MS, White PS (1991) Limited CT scanning techniques of the paranasal sinuses. J Laryngol Otol 105:20–23
Fahmy FF, McCombe A, Mckiernan DC (2002) Sino nasal outcome questionnaire, a patient focussed, rhinosinusitis specific outcome measure. Rhinology 40:195–197
Fahmy FF, McCombe A (2002) General versus specific sino-nasal outcome measures. Clin Otolaryngol 27:283–284
Lund VJ, Mackay IS (1993) Staging in rhinosinusitis. Rhinology 31:183–184
Chow JM, Stankiewicz JA (2003) Cost analysis in the diagnosis of chronic rhinosinusitis. Am J Rhinol 17:139–142
Diaz-Marchan PJ, Siccard MW, Syewart MG, Piccorillo JF (1999) Severity staging in chronic rhinosinusitis; are CT scan findings related to patient symptoms? Am J Rhinol 13:161–167
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Basu, S., Georgalas, C., Kumar, B.N. et al. Correlation between symptoms and radiological findings in patients with chronic rhinosinusitis: an evaluation study using the Sinonasal Assessment Questionnaire and Lund-Mackay grading system. Eur Arch Otorhinolaryngol 262, 751–754 (2005). https://doi.org/10.1007/s00405-004-0891-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-004-0891-0