
Abstract
Purpose
Despite the well-known neonatal morbidity risks after elective cesarean deliveries performed before 39 weeks, there are scarce data regarding mortality risks. The objective of this study was to calculate the risk of neonatal mortality after elective repeat cesarean delivery (ERCD) by gestational age.
Methods
The Linked Birth–Infant Death Data Files from the Vital Statistics Data of the Center for Disease Control and Prevention of the U.S. from 2004 to 2008 were analyzed. Only ERCD cases were included. Early death (<7 days), neonatal death (<28 days), and infant death (<1 year) were evaluated. A logistic regression model was used to calculate odds ratios. Cases delivered at 37–41 weeks were studied with 40 weeks as reference.
Results
A total of 483,052 cases were included for analysis. The distribution of rates and odds ratios for infant, neonatal and early death was U-shaped with the nadir at 39 weeks. There was a statistically significant increase in early death at 37 compared to 40 weeks’ gestation [OR (95 %) CI = 1.929(1.172–3.176)]. No statistical increase was found in any of the other mortality risks.
Conclusion
There is an increased risk in early death with ERCD performed at 37 weeks. Our study provides evidence of neonatal harm beyond the reported morbidity risks.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The cesarean delivery rate in the United States has rapidly increased since the 1990s [1], with many of these procedures being both elective and repeat [1, 2]. Optimal timing of elective repeat cesarean delivery (ERCD) is important for the prevention of adverse neonatal outcomes.
Historically, the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine have advocated delaying deliveries until 39 completed weeks’ gestation or beyond [3–6] to decrease the risks of newborn prematurity. The recommendation for delaying ERCD until 39 weeks’ gestation is very well supported by the literature [3–12]. Because of these studies, we know that non-indicated early-term (37 0/7–38 6/7 weeks’ gestation) cesarean deliveries are associated with an increase in adverse neonatal outcomes [8].
Unfortunately, despite current recommendations, early-term cesarean delivery rates continue to be significant in the United States; being approximately 33 % in 2009 [1]. Because of this trend, there is an effort to promote multiple policies to increase awareness on the topic and decrease current rates.
Numerous existing studies focus on maternal or neonatal morbidity and adverse outcomes [8, 13, 14], however, there are few data specifically addressing infant mortality after ERCD according to gestational age. Some of this information is only found within the results of studies whose emphases were morbidity risks. Little research has been done regarding the risk of neonatal death according to gestational age, likely due to the low numbers available for study. Neonatal mortality is an uncommon event, especially in elective procedures, and the number of cases needed to achieve enough power is very high. We wanted to test the hypothesis that an increased risk of neonatal mortality after ERCD exists in earlier gestational ages beyond the well-known morbidity risks in the hopes of using this information to increase awareness and promote public policies for better adherence to guidelines as well as to improve patient care and counseling.
Methods
The Institutional Review Board of Wayne State University/Detroit Medical Center in Detroit, Michigan reviewed and approved the protocol of this study. The design was retrospective, cohort study. The Linked Birth–Infant Death Data Files from the Vital Statistics Data of the Center of Disease Control and Prevention (CDC) of the United States from the years 2004–2008 (the most available data at the time of selecting cases for analysis) were reviewed to examine neonatal and infant death rates.
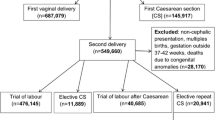
The inclusion criteria used were: cases of singleton deliveries, method of delivery by repeat cesarean, no attempted trial of labor and gestational age at delivery between 37 and 41 weeks. Exclusion criteria were any reported congenital anomalies and risk factors such as diabetes, chronic hypertension and pregnancy-related hypertensive disorders including eclampsia. Since we selected all cases in the window period, power analysis was not necessary. The mortality-related newborn outcomes analyzed were: early death (when the demise occurred at less than 7 days), neonatal death (less than 28 days), and infant death (less than 1 year).
All frequencies were represented in percentages. The rates of mortality-related outcomes were represented in rates per 1000 births. A forward stepwise logistic regression model was performed to calculate the unadjusted odds ratio of mortality-related variables according to gestational age from 37 to 41 weeks, using 40 weeks gestational age at delivery as the reference group. The gestational age of 40 weeks was chosen as reference as this has been traditionally considered “at term”. Standard confounders found in the literature, including variables such as maternal age, maternal race, parity, infant’s gender and year of delivery were used as covariates to calculate adjusted odds ratios. Information regarding BMI was not available in the datasets to be used as a confounder. All of the data were analyzed by a clinical statistician with the use of the statistical package SPSS software version 17.0. A p value of <0.05 with a 95 % confidence interval not crossing one was used to indicate statistical significance.
Results
After inclusion and exclusion criteria were applied, a total of 483,052 cases of ERCD were included for analysis. Of these, 394,885 (81.8 %) were Whites, 59,480 (12.3 %) were Blacks, 2963 (0.61 %) were American–Indians and 25,724 (31 %) were Asians. Regarding the newborn’s gender 51 % were female and 49 % were male.
The number of deliveries according to gestational age is shown on Table 1. From a total of 483,052 deliveries, 171,316 cases (35.5 %) were performed at 39 weeks and 75,950 were performed at 40–41 weeks. Nearly half of all ERCDs, 253,786 cases (48.8 %), were performed before 39 weeks’ gestation.
The rates of infant, neonatal and early death (computed per 1000 live births) are shown in Table 1 and Fig. 1. For the three mortality-related variables analyzed (early, neonatal and infant death) the distribution of the rates by gestational age from 37 to 41 weeks’ gestation are U-shaped, with the nadir at 39 weeks’ gestation (p < 0.05).

Mortality rates (per 1000 births) according to gestational age after elective repeat cesarean delivery divided in infant death, neonatal death and early death
The unadjusted and adjusted odds ratios of the mortality-related outcomes according to gestational age (using 40 weeks’ gestation as a reference) are shown in Table 2. For early neonatal death, the distribution of the Exp (B) values from 37 to 41 weeks’ gestation is U-shaped, with the nadir at 39 weeks. The risk of early death was almost twofold at 37 weeks [OR (95 %) CI = 1.929 (1.172–3.176)] compared to 40 weeks. The other odds ratios compared to 40 weeks were not statistically different.
For neonatal and infant death, the distribution of the exp (B) values from 37 to 41 weeks was also U-shaped, with the nadir at 39 weeks. However, the results were not statistically different. The adjusted odds ratios of all mortality-related outcomes at 37 compared to 40 weeks are shown in Fig. 2.

Adjusted ORs for mortality outcomes at 37 weeks divided by infant mortality, neonatal mortality and early mortality
Discussion
The findings presented show that performing an ERCD at 39 weeks’ gestation is associated with the lowest rates of neonatal mortality. The overall rates are graphically plotted as U-shaped, with the nadir at 39 weeks. These results are consistent with the current prevailing evidence that elective delivery before 39 weeks’ gestation is associated with significant neonatal morbidity [3–6, 8, 13, 14]. In our study, the overall risks are increased most apparently at 37 weeks and were found to be lowest at 39 weeks’ gestation. This finding is consistent with previous studies that suggest 39 weeks to be the optimal time to perform elective delivery procedures [8, 9, 13–15].
Just like previous reports [8, 9, 13], our study showed that nearly 50 % of ERCDs were performed before 39 weeks’ gestation, which demonstrates a lack of adherence to current guidelines. Most importantly, we found a 92.9 % increased risk in early death if ERCD was performed at 37 compared to 40 weeks’ gestation. This finding supports the evidence that performing early-term ERCD not only increases neonatal morbidity risk, but also mortality.
While many studies mention neonatal mortality risks associated with elective procedures, there are very few studies dedicated to it. One of the reasons might be because studying mortality related to elective procedures is more difficult as the risks of complications are presumably lower than medically required emergency procedures [9, 12–21]. In terms of elective early-term deliveries, there are greater reported rates of mortality among neonates delivered during the early-term period compared with those delivered at term [6].
De Luca et al. [16]. conducted a cohort study to evaluate the age-stratified risk of intrapartum and neonatal morbidity and mortality after elective cesarean delivery and found that mortality had a strong gestational age-related trend with the lowest rates found between 38 and 40 weeks’ gestation independent of delivery mode.
Compared to medically indicated procedures, studies about neonatal mortality following elective procedures are scarce. In case series, this outcome has been reported after ERCD but only as an uncommon complication; this lack of a large pool of relevant data decreases the ability to obtain statistically significant results specifically related to neonatal mortality and timing of ERCD [13, 14]. Some of the information regarding the subject is found within the results of morbidity-based studies; however, very few mortality cases are reported and this low rate of neonatal mortality associated with elective procedures accounts for why it is so difficult to achieve high powered studies on the subject [8, 14, 22–25]. A major strength of our study lies in the very large sample size available for evaluation, and also the comprehensive population-based nature of the data set, which includes all births over a broad time period, together with the large number of socio-demographic and medical variables available for analysis. Analyzing the mortality differential of ERCDs stratified for gestational age and finding a statistically significant difference in outcome was made possible by the size of the data pool. Because the mortality rate for elective delivery procedures is so low, most clinic- or hospital-based studies would not have had enough power in terms of sample size to detect a statistically significant difference in mortality of one infant death per 1000 live births.
Despite the above, limitations of the study associated with the database were also present; most notably the accuracy of reporting specific data items of interest along with gestational age ascertainments per the initial providers. Natality records provide an excellent resource for most demographic information as well as straightforward medically related items like method of delivery and fetal measurements post-delivery, however, there is still an underreporting of individual medical risk factors and complications of labor and delivery on birth certificates [26, 27].
ERCD timing decision-making should weigh and balance the risks and benefits for both mother and fetus. It is still not known if earlier delivery scheduling may help avoid certain complications that could potentially appear as gestation progresses such as preeclampsia, eclampsia, placental abruption and labor with a subsequent risk of urgent cesarean section and/or uterine rupture since it is estimated that about 10 % of women go into spontaneous labor between 37 and 39 weeks [28]. Delaying delivery for an additional week increases the time that the woman and her fetus are vulnerable to unexpected complications and increases the proportion of women who might be forced to deliver by emergency procedures [21]. Earlier scheduling on the other hand, could potentially increase patient comfort and the ability to schedule the delivery around life plans besides ensuring the presence of their private physician at delivery; however, it could also increase the risk of prematurity-related outcomes. Most ERCD studies tend to exclude women who delivered non-electively before the scheduled date of delivery from their statistical analysis [21]. Further research is needed to evaluate the impact that these cases have on the timing of elective procedures since excluding them may overestimate potential benefits of ERCD [21].
Beyond the health risks, cost is also always a consideration in health care decision-making and reform. Neonatal hospitalization costs may be contained through careful consideration of timing of delivery in patients undergoing ERCD [20]. Robinson et al. [20] found that the delay of ERCD to 39 weeks of gestational age was associated with significant cost savings in terms of neonatal management.
We believe there is still considerable research to be done focusing on ERCD timing, especially when it comes to the influence of other factors such as race/ethnicity and newborn gender; these factors should be studied and considered at the time of implementing more elaborate guidelines and policies in the field of maternal-fetal medicine.
Overall, there is a demonstrable increase in early death with ERCD performed at 37 weeks. Our study provides evidence of neonatal harm beyond the morbidity risks that are usually quoted. The latter should emphasize the importance of promoting better adherence to current recommendations [6], as well as to increase the awareness of physicians and patients to the risks of non-indicated early-term deliveries. In addition to preventing unnecessary adverse health outcomes for both mother and neonate, better adherence to established policies will also decrease the overwhelming financial burden of associated hospital and governmental costs of neonatal morbi-mortality. To our knowledge, this is the first study of its kind that has focused on evaluating risks of neonatal death according to gestational age in ERCD.
References
Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Kirmeyer S, Mathews TJ, Wilson EC (2011) Births: final data for 2009. Natl Vital Stat Rep 60(1):1–70
NIH State-of-the-Science Conference Statement on cesarean delivery on maternal request (2006) NIH Consens State Sci Statements 23(1):1–29
Obstetrics ACoPB (2009) ACOG Practice Bulletin No. 107: Induction of labor. Obstetrics and gynecology 114 (2 Pt 1):386–397. doi:10.1097/AOG.0b013e3181b48ef5
Gynecologists ACoOa (2013) ACOG committee opinion no. 559: Cesarean delivery on maternal request. Obstetrics and gynecology 121(4):904–907. doi:10.1097/01.AOG.0000428647.67925.d3
Gynecologists ACoOa (2013) ACOG committee opinion no. 560: Medically indicated late-preterm and early-term deliveries. Obstetrics and gynecology 121(4):908–910. doi:10.1097/01.AOG.0000428648.75548.00
Gynecologists ACoOa (2013) ACOG committee opinion no. 561: Nonmedically indicated early-term deliveries. Obstetrics and gynecology 121(4):911–915. doi:10.1097/01.AOG.0000428649.57622.a7
Bates E, Rouse D, Tita A (2011) Neonatal outcomes after demonstrated fetal lung maturity before 39 weeks of gestation. Obstet Gynecol 117(5):1229. doi:10.1097/AOG.0b013e3182176296
Tita AT, Landon MB, Spong CY, Lai Y, Leveno KJ, Varner MW, Moawad AH, Caritis SN, Meis PJ, Wapner RJ, Sorokin Y, Miodovnik M, Carpenter M, Peaceman AM, O’Sullivan MJ, Sibai BM, Langer O, Thorp JM, Ramin SM, Mercer BM, Network EKSNM-FMU (2009) Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med 360(2):111–120. doi:10.1056/NEJMoa0803267
Tita AT, Lai Y, Landon MB, Spong CY, Leveno KJ, Varner MW, Caritis SN, Meis PJ, Wapner RJ, Sorokin Y, Peaceman AM, O’Sullivan MJ, Sibai BM, Thorp JM, Ramin SM, Mercer BM, (MFMU) EKSNIoCHaHDNM-FMUN (2011) Timing of elective repeat cesarean delivery at term and maternal perioperative outcomes. Obstet Gynecol 117(2 Pt 1):280–286. doi:10.1097/AOG.0b013e3182078115
Ertuğrul S, Gün I, Müngen E, Muhçu M, Kılıç S, Atay V (2013) Evaluation of neonatal outcomes in elective repeat cesarean delivery at term according to weeks of gestation. J Obstet Gynaecol Res 39(1):105–112. doi:10.1111/j.1447-0756.2012.01951.x
Saidu R, Bolaji BO, Olatinwo AW, McIntosh CM, Alio AP, Salihu HM (2011) Repeat caesarean delivery as a risk factor for abnormal blood loss, blood transfusion and perinatal mortality. J Obstet Gynaecol 31(8):728–731. doi:10.3109/01443615.2011.606933
Tzur T, Weintraub AY, Sheiner E, Wiznitzer A, Mazor M, Holcberg G (2011) Timing of elective repeat caesarean section: maternal and neonatal morbidity and mortality. J Matern Fetal Neonatal Med 24(1):58–64. doi:10.3109/14767051003678267
Clark SL, Miller DD, Belfort MA, Dildy GA, Frye DK, Meyers JA (2009) Neonatal and maternal outcomes associated with elective term delivery. Am J Obstet Gynecol 200(2):156.e151–156.e154. doi:10.1016/j.ajog.2008.08.068
Chiossi G, Lai Y, Landon MB, Spong CY, Rouse DJ, Varner MW, Caritis SN, Sorokin Y, Oʼsullivan MJ, Sibai BM, Thorp JM, Ramin SM, Mercer BM, Network EKSNIoCHaHDNM-FMUM (2013) Timing of delivery and adverse outcomes in term singleton repeat cesarean deliveries. Obstet Gynecol 121(3):561–569. doi:10.1097/AOG.0b013e3182822193
Clark SL, Frye DR, Meyers JA, Belfort MA, Dildy GA, Kofford S, Englebright J, Perlin JA (2010) Reduction in elective delivery at < 39 weeks of gestation: comparative effectiveness of 3 approaches to change and the impact on neonatal intensive care admission and stillbirth. Am J Obstet Gynecol 203(5):449.e441–449.e446. doi:10.1016/j.ajog.2010.05.036
De Luca R, Boulvain M, Irion O, Berner M, Pfister RE (2009) Incidence of early neonatal mortality and morbidity after late-preterm and term cesarean delivery. Pediatrics 123(6):e1064–e1071. doi:10.1542/peds.2008-2407
Ecker J (2013) Elective cesarean delivery on maternal request. JAMA 309(18):1930–1936. doi:10.1001/jama.2013.3982
Hansen AK, Wisborg K, Uldbjerg N, Henriksen TB (2007) Elective caesarean section and respiratory morbidity in the term and near-term neonate. Acta Obstet Gynecol Scand 86(4):389–394. doi:10.1080/00016340601159256
Hourani M, Ziade F, Rajab M (2011) Timing of planned caesarean section and the morbidities of the newborn. N Am J Med Sci 3(10):465–468. doi:10.4297/najms.2011.3465
Robinson CJ, Villers MS, Johnson DD, Simpson KN (2010) Timing of elective repeat cesarean delivery at term and neonatal outcomes: a cost analysis. Am J Obstet Gynecol 202(6):632.e631–632.e636. doi:10.1016/j.ajog.2010.03.045
Salim R, Shalev E (2010) Health implications resulting from the timing of elective cesarean delivery. Reprod Biol Endocrinol 8:68. doi:10.1186/1477-7827-8-68
Paterson CM, Saunders NJ (1991) Mode of delivery after one caesarean section: audit of current practice in a health region. BMJ 303(6806):818–821
Perveen S (2011) Maternal and neonatal adverse outcome at repeat cesarean delivery versus repeat vaginal delivery. J Coll Physicians Surg Pak 21(2):84–87. doi:02.2011/JCPSP.8487
Bujold E, Francoeur D (2005) Neonatal morbidity and decision-delivery interval in patients with uterine rupture. J Obstet Gynaecol Can 27(7):671–673 (author reply 673)
Go MD, Emeis C, Guise JM, Schelonka RL (2011) Fetal and neonatal morbidity and mortality following delivery after previous cesarean. Clin Perinatol 38(2):311–319. doi:10.1016/j.clp.2011.03.001
Lydon-Rochelle MT, Holt VL, Cárdenas V, Nelson JC, Easterling TR, Gardella C, Callaghan WM (2005) The reporting of pre-existing maternal medical conditions and complications of pregnancy on birth certificates and in hospital discharge data. Am J Obstet Gynecol 193(1):125–134. doi:10.1016/j.ajog.2005.02.096
Adams MM, Kirby RS (2007) Measuring the accuracy and completeness of linking certificates for deliveries to the same woman. Paediatr Perinat Epidemiol 21(Suppl 1):58–62. doi:10.1111/j.1365-3016.2007.00838.x
Abouzeid H, Aggarwal D, De Graaf F (2007) Timing of planned repeated caesarean section: an enigma. J Obstet Gynaecol 27(8):798–801. doi:10.1080/01443610701666843
Acknowledgments
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest.
Rights and permissions
About this article

Cite this article
Vilchez, G., Hoyos, L.R., Maldonado, M.C. et al. Risk of neonatal mortality according to gestational age after elective repeat cesarean delivery. Arch Gynecol Obstet 294, 77–81 (2016). https://doi.org/10.1007/s00404-015-3955-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-015-3955-z