
Abstract
Purpose
Our aim is to determine if the reproductive performance after hysteroscopic resection of partial uterine septum was related to septum size.
Methods
The retrospective and comparative cohort study was conducted in a University-affiliated Hospital. A cohort of 112 non-parous patients was treated for a partial uterine septum. The septum size was evaluated by hysteroscopy and transvaginal 3-dimensional ultrasound. The patients were stratified into two groups: group 1 (85 women) with small partial uterine septum (≤2.5 cm) and group 2 (27 women) with large partial uterine septum (>2.5 cm). They were also divided according to their obstetrics history: 39 infertile women and 73 aborters. All underwent hysteroscopic metroplasty with a resectoscope with an equatorial semicircular loop cutting 0° with monopolar energy. All septa were almost completely removed and no complications occurred.
Results
The two groups of patients with small (group 1) and large (group 2) partial uterine septum were compared in the terms of reproductive history and performance before and after surgery. In the overall population the reproductive performance after surgery is greatly improved. No significant differences in reproductive performance were evident between patients with small and large partial uterine septa. The reproductive performance was also similar in infertile patients and in aborters.
Conclusions
This study demonstrates that hysteroscopic metroplasty in cases of partial uterine septum and infertility significantly improves the reproductive performance irrespectively of septum size and that reproductive performance is independent from previous obstetrics history.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Congenital uterine anomalies are the most common types of malformations of the reproductive system and result from a defect of fusion of paramesonephric ducts during embryogenesis [1]. They may be associated with recurrent pregnancy loss, preterm labor, abnormal fetal presentation, and infertility [1–3]. The incidence of uterine malformations varies from ~3–4 % [4] to ~6–7 % [5] in the general and infertile population and from ~13 % [4] to ~17 % [5] in recurrent pregnancy loss population. Grimbizis et al. [4] observed that the septate uterus was the most common anomaly in general population, whereas Saravelos et al. [5] indicated the arcuate uterus as the commonest anomaly in general and recurrent pregnancy loss population and the septate uterus in the infertile population. These apparently contradictory data may be explained by different diagnostic procedures and the subjectivity of the diagnostic criteria, although it is largely accepted today that the most accurate diagnostic procedures are combined hysteroscopy, laparoscopy and 3-dimensional ultrasound [5, 6].
According to the most worldwide accepted classification system of the American Society for Reproductive Medicine (ASRM) [7] a partial septate uterus corresponds to Class Vb, a complete uterine septum to a Class Va and an arcuate uterus to a Class VI. The hysteroscopic metroplasty by resectoscope is considered the first therapeutic option for such anomalies [8, 9]. The ASRM classification, however, presents some limitations on the exact assessment of each case [10]. In particular, Class Vb (partial septate uterus) includes a very heterogeneous variety of septa based on the severity of midline uterine abnormality and creates a non-homogenous group. Today, no data are reported on the impact on reproductive performance of different septum sizes within Class Vb.
The aim of our study was to assess for the first time the reproductive performance after hysteroscopic resection of partial septate uteri according to septum size. A small partial uterine septum was defined as having a length of ≤2.5 cm, namely less than one-half of a normal uterine cavity [11]. A partial septum was defined large, but not complete, if has a length of >2.5 cm, namely extending over more than one-half of the uterine cavity. We evaluated, in particular, (a) if is possible to indentify new subgroups of Class Vb according to the real dimension of the septum and its effect on reproduction, and (b) if the different obstetric history between women with no prior conceptions and women with earlier abortions in patients with uterine septum may have a clinical relevance in reproductive performance after surgery.
Materials and methods
Recently, we retrospectively evaluated the reproductive performance in 246 infertile patients having undergone hysteroscopic resection of a partial uterine septum (Class Vb) at our department [12]. Criteria for exclusion of any other causes of infertility other than the uterine septum were oligo- or anovulation and menstrual irregularities evaluated with at least some months of monophasic basal body temperature records and progesterone levels below 4 ng/mL in the mid-luteal phase, imperviousness of the Fallopian tubes demonstrated by laparoscopy or high-contrast sonography and partners with abnormal semen analysis.
In this study, particularly, our primary outcome parameter was to evaluate if septum size may interfere on the reproductive performance after surgery. Therefore, the main criterion for inclusion were accurate data on the size of the septum, and within the whole group of 246 treated patients only a cohort of 112 women, operated between January 2001 and June 2007, had these requirements derived from office hysteroscopy and transvaginal 3-dimensional ultrasound. Pelvic ultrasound assessment was performed by two experienced sonographers (M.G. and C.B.). In most cases laparoscopy was also available. Accordingly, the subjects were divided into two groups. Group 1 consisted of 85 women with uterine septum ≤2.5 cm (mean ± standard deviation (SD) age 35.3 ± 4.7 [95 % confidence interval (CI) 33.9–36.0]). Group 2 consisted of 27 women with uterine septum >2.5 cm (mean ± SD age 33.3 ± 4.8 [95 % CI 31.1–34.9]). Age was not significantly different between the two groups (p = 0.054).
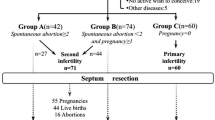
As a second outcome parameter we evaluated the reproductive performance after surgery compared to the previous obstetrics history and we additionally compared the reproductive outcome during the last 2 years before (24.1 ± 4.1 months [23.3–24.8: 95 % CI]) and the first 2 years after the operation (24.8 ± 2.4 months [24.3–25.2: 95 % CI]). This period was chosen because, by definition, a patient should be defined infertile if does not get a full-term pregnancy after at least 1 year. The patients were then divided into two sub-groups according to their fertility history: 39 infertile patients and 73 aborters. Four patients, who had had an abortion before the preoperative follow-up, were added to aborters, and three (3.5 %) of these take part of Group 1 and one (3.7 %) of Group 2 (p = N.S.). The study was approved by our local Ethical Committee. All the procedures followed in the study were in accordance with the Helsinki Declaration of 1975.
All hysteroscopic resections were scheduled after signed an informed surgical consent form in the early follicular phase without any preoperative hormonal treatment. Surgery was made under general anesthesia and performed as previously reported [12, 13]. In brief, the cervix was dilated with Hegar dilatators up to size 10 to enable to introduce a 27 F gauge resectoscope in the uterine cavity. The resectoscope includes a continuous-flow sheath that provides constant inflow and outflow of fluid generating a continuous washing of the uterine cavity and a 12° telescope (Hopkins II®, Storz, Tuttlingen, Germany). The septum resection was performed with an equatorial semicircular loop [13], cutting 0° with monopolar energy (cut 80 W) (Hopkins II®, Storz, Tuttlingen, Germany) and a non-conductive, hypoosmolar solution of sorbitol (2.7 %) and mannitol (0.54 %) (Bieffe Medical, Grosseto, Italy) as a medium of distension. Data on septum length were confirmed during hysteroscopic resection comparing the length of the 1.0-cm-long yellow tip of the electronic knife to the length of the resected septum. After visualization of the tubal ostia the resection was started from the lower margin of the septum and continued until the muscular component of the wall uterus and venous myometrial vessels was evident. An adequate fundus thickness is important to avoid uterine perforation during the surgery itself or the rupture of the uterus during pregnancy or childbirth. After incision a normal cavity was obtained and the hysteroscope could be moved freely from one tubal ostium to the other without any intervening obstruction. Surgical procedures took 10–20 min and were made by the same highly experienced surgeon (R.P.). All the patients were discharged on the same day after surgery.
After surgery no hormonal treatment was administered. Patients were advised to have safe sex for 3 months to avoid pregnancy and a transvaginal 3-dimensional ultrasound was performed after 3–4 months to confirm surgical outcome and evaluate eventual residual uterine septa. An adequate period of follow-up of the patients was followed, and it was similar to that of the pre-surgery follow-up. Follow-up was done by phone with particular emphasis of the desire to become pregnant, the achievement of pregnancy and its outcome. All women had actively tried to conceive and carry the pregnancy to term. No patient was lost during the follow-up.
Statistical analysis
Statistical analysis was made by means of the SPSS 13.0 software; SPSS Inc., Chicago IL, USA. The mean ± SD and 95 % CI were used to describe continuous data. The Mann–Whitney test was also used to compare the age of the two groups. The Fisher exact test was used to analyze dichotomous variables, as well as to compare the frequencies of cases that modified the type of infertility after surgery between the two groups, while the Mc Nemar test was applied to paired data. Data were further confirmed by Z-testing for two proportions. Two-tailed p values less than 0.05 were accepted as statistically significant.
Results
All septa were almost completely removed and no complications occurred. In same cases a residual uterine septum was observed after surgery, but none were re-judged to need further surgery.
The reproductive performance in the whole cohort of patients and in the two subgroups of infertile patients and aborters after surgery is reported in Table 1. In the overall non-parous population (112 patients), almost half (53, 47.3 %) of the patients had a preterm or term delivery, evidencing a significant increase of delivery rate (p < 0.001). This delivery rate, however, was identical both in infertile women and in aborters (p = N.S.). About the 59 patients not delivering after surgery, a trend to the increase of the infertile women was observed (Table 1), although not reaching the significant limit (p = N.S.); in fact 63.6 % of the infertile patients continued to fail pregnancy versus 51.4 % of the aborters which continued to have abortions.
Moreover, we have analyzed the reproductive history and performance before and after septum resection, respectively, of the two groups of patients with small (Group 1) and large (Group 2) partial uterine septum. The main analyzed variables (pregnancy, abortion, live birth rates, etc.) before surgery are reported in Table 2 and after surgery in Table 3. Before surgery there are no differences in obstetrics history between Group 1 and 2 (p = N.S.). After surgery also no significant differences (p = N.S.) in the term of reproductive performance are observed in the two groups.
Discussion
The study shows an excellent prognosis for successful pregnancy after hysteroscopic metroplasty because in the cohort of patients treated the septum resection highly improves reproductive performance, increasing delivery rates and decreasing indirectly abortion rates. This confirms the efficacy of surgical correction of uterine anomalies reported earlier [12, 13] and other studies [14–17]. Moreover, we minimize the eventual persistence of any residual uterine septum of <1 cm after surgery because may be considered in the same way of arcuate anomaly as a benign and almost normal variant of uterine morphology [18] and therefore of no impact in reproductive outcomes, according to Fedele et al. [19], although Kormanyos et al. [20] disagree.
Analyzing patients who underwent metroplasty according to their obstetric history, there were no differences between infertile patients and aborters. Our data confirm the efficacy of surgical treatment also in infertile patients, in agreement with other recent studies [21–23], who found good outcomes in pregnancy, fecundity, and life birth rate after metroplasty in patients with unexplained primary infertility, but in contrast with Bosteels et al. [24] who demonstrated a significantly higher pregnancy rate in patients with recurrent pregnancy loss than in those with primary infertility, although recurrent pregnancy loss is a multifactorial disease. The multifactorial origin of recurrent pregnancy loss is, in fact, the explanation of the persistently higher abortion rate after surgery compared to the general population. Worthy of signaling among the aborters is that almost half of the patients not delivering after metroplasty did not conceive. This problem may be attributable to the short follow-up period or to the high maternal age, as has been reported by us already [12]. It is worth mentioning also the different mean ± SD age between the patients of our study and those of Tonguc et al. [23] study. Our cohort of patients has a markedly higher age than that of Tonguc’s cohort, probably because of different socio-cultural and socio-economical conditions, but the reproductive performance after surgical treatment is very similar. This enhances the hypothesis that in premenopausal women, when septum is removed, the normal uterine fibromuscular tissue retains a good effectiveness in the course of the years.
We also evaluated for the first time the impact of the uterine septum size within ASRM Classification Class Vb on the reproductive history and performance before and after hysteroscopic metroplasty, respectively. A cut-off of approximately 2.5 cm (1 in.) was arbitrarily selected based on the size of uterine cavity. Considering that uterine corpus without cervix has a length of about 5 cm, by varying from 4.4 cm in nulliparas to 4.9 cm in primiparas and 5.6 cm in women with two or more deliveries [11], we chose 2.5 cm as ideal cut-off between small septa with a length less than one half of the uterine cavity and large but not complete septa with a length more than one half of the uterine cavity. In truth there is a difference between the length of uterine corpus and the length of uterine cavity. However, this can be accepted as a minor drawback of the study. Indeed, we found no significant differences in any of the analyzed variables in the two groups that were homogeneous for preoperative characteristics and both small and large septa profited by surgical treatment regardless of size. The supposed pathogenetic mechanisms by which the septate uterus causes reproductive failure and obstetric complications are extremely various, such as inadequate uterine vascularization [25], uncoordinated uterine contractions [26, 27], altered composition of the fibroelastic connective tissue of septum [27] and/or irregular sensitivity to hormonal changes of septal endometrium [28]. However, whatever the real mechanism may be, this is probably not influenced by septum size.
In literature the impact of different septum size on the reproductive outcome was very poorly and rarely studied. Golan et al. [29] evaluated patients with early abortions undergone diagnostic hysteroscopy and found uterine anomalies in a quarter of cases, especially incomplete septum, concluding that a partial uterine septum is a major risk factor predisposing to miscarriage. This is, however, an observational study in which women did not undergo any surgery and the length of the septum was not evaluated. Tomazevic et al. [30], on the other hand, analyzed women with history of hysteroscopic metroplasty, comparing the preterm births rate in two groups of patients with Class VI (arcuate uterus) and whole Class V (partial and complete septate uterus) anomalies. These authors concluded that these anomalies are an important risk factor for preterm deliveries regardless of size septum, but did not distinguish within the Class V anomalies between complete and partial uterine septum and within the Class Vb anomalies between small and large partial uterine septum. Finally, the observation that the reproductive performance after metroplasty is independent of septum size in cases of Class Vb fits very well with the new ESHRE–EGSE consensus on the classification system of female genital tract congenital anomalies where any septum above the level of internal cervical os is defined as partial (Class U2a) [31].
Even with the limitations of a retrospective study and the absence of control groups our figures demonstrated that (a) hysteroscopic metroplasty in case of partial uterine septum and infertility improves significantly the reproductive performance irrespectively of septum size; (b) infertile patients have after surgery a marked increase of pregnancy rate and (c) aborters have a marked decrease of abortion rate and therefore even if these patients are able to achieve pregnancy they need metroplasty in advance to avoid possibly preventable abortions.
References
Rock JA, Jones HWJ (1977) The clinical management of the double uterus. Fertil Steril 12:798–806
Raga F, Bauset C, Remohi J, Bonilla-Musoles F, Simón C, Pellicer A (1997) Reproductive impact of congenital Müllerian anomalies. Hum Reprod 12:2277–2281
Heinonen PK, Saarkisoski S, Pystynen P (1982) Reproductive performance of women with uterine anomalies. Acta Obstet Gynecol Scand 61:157–162
Grimbizis GF, Camus M, Tarlatzis BC, Bontis JN, Devroey P (2001) Clinical implications of uterine malformations and hysteroscopic treatment results. Hum Reprod Update 7:161–174
Saravelos SH, Cocksedge KA, Li T-C (2008) Prevalence and diagnosis of congenital uterine anomalies in women with reproductive failure: a critical appraisal. Hum Reprod Update 14:415–429
Ghi T, Casadio P, Kuleva M, Perrone AM, Savelli L, Giunchi S et al (2009) Accuracy of three-dimensional ultrasound in diagnosis and classification of congenital uterine anomalies. Fertil Steril 92:808–813
The American Fertility Society (1988) The American Fertility Society Classifications of Adnexal Adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Müllerian anomalies and intrauterine adhesions. Fertil Steril 49:944–955
Siegler AM, Valle RF (1988) Therapeutic hysteroscopic procedures. Fertil Steril 50:685–701
Valle RF (1996) Hysteroscopic treatment of partial and complete uterine septum. Int J Fertil Menop S 41:310–315
Gubbini G, Di Spiezio Sardo A, Nascetti D, Marra E, Spinelli M, Greco E et al (2009) New outpatient subclassification system for American fertility society classes V and VI uterine anomalies. J Minimal Invasive Ginecol 16:554–561
Merz E, Miric-Tesanic D, Bahlmann F, Weber G, Wellek S (1996) Sonographic size of uterus and ovaries in pre- and postmenopausal women. Ultrasound Obstet Gynecol 7:38–42
Paradisi R, Barzanti R, Natali F, Battaglia C, Venturoli S (2011) Hysteroscopic metroplasty in a large population of women with septate uterus. J Minim Invasive Gynecol 18:449–454
Venturoli S, Colombo FM, Vianello F, Seracchioli R, Possati G, Paradisi R (2002) A study of hysteroscopic metroplasty in 141 women with septate uterus. Arch Gynecol Obstet 266:157–159
Valle RF, Sciarra JJ (1986) Hysteroscopic treatment of the septate uterus. Obstet Gynecol 67:253–257
Grimbizis G, Camus M, Clasen K, Tournaye H, De Munck L, Devroey P (1998) Hysteroscopic septum resection in patients with recurrent abortion or infertility. Hum Reprod 13:1188–1193
Porcu G, Cravello L, D’Ercole C, Cohen D, Roger V, de Montgolfier R et al (2000) Hysteroscopic metroplasty for septate uterus and repetitive abortions: reproductive outcome. Eur J Obstet Gynecol Reprod Biol 88:81–84
Bakas P, Gregoriou O, Hassiakos D, Liapis A, Creatsas M, Konidaris S (2012) Hysteroscopic resection of uterine septum and reproductive outcome in women with unexplained infertility. Gynecol Obstet Invest 73:321–325
Mucowski SJ, Herndon CN, Rosen MP (2010) The arcuate uterine anomaly: a critical appraisal of its diagnostic and clinical relevance. Obstet Gynecol Surv 65:449–454
Fedele L, Bianchi S, Marchini M, Mezzopane M, Di Nola G, Tozzi L (1996) Residual uterine septum of less than 1 cm after hysteroscopic metroplasty does not impair reproductive outcome. Hum Reprod 11:727–729
Kormanyos Z, Molnar BG, Pal A (2006) Removal of a residual portion of a uterine septum in women of advanced reproductive age: obstetric outcome. Hum Reprod 21:1047–1051
Mollo A, De Franciscis P, Colacurci N, Cobellis L, Perino A, Venezia R et al (2009) Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: a prospective controlled trial. Fertil Steril 91:2628–2631
Nouri K, Ott J, Huber JC, Fisher EM, Stögbauer L, Tempfer CB (2010) Reproductive outcome after hysteroscopic septoplasty in patients with septate uterus—a retrospective cohort and systematic review of the literature. Reprod Biol Endocrinol 8:52
Tonguc EA, Var T, Batioglu S (2011) Hysteroscopic metroplasty in patients with a uterine septum and otherwise unexplained infertility. Int J Gynecol Obstet 113:128–130
Bosteels J, Weyers S, Puttemans P, Panayotidis C, Van Herendael B, Gomel V et al (2010) The effectiveness of hysteroscopy in improving pregnancy rates in subfertile women without other gynaecological symptoms: a systematic review. Hum Reprod Update 16:1–11
Dabirashrafi H, Bahadori M, Mohammad K, Alavi M, Moghadami-Tabrizi N, Zandinejad K et al (1995) Septate uterus: new idea on the histologic features of the septum in this abnormal uterus. Am J Obstet Gynecol 172:105–107
Blum M (1978) Comparative study of serum CAP activity during pregnancy in malformed and normal uterus. J Perinat Med 6:165–168
Sparac V, Kupesic S, Ilijas M, Zodan T, Kurjak A (2001) Histologic architecture and vascularisation of hysteroscopically excised intrauterine septa. J Am Assoc Gynecol Laparosc 8:111–116
Fedele L, Bianchi S, Marchini M, Franchi D, Tozzi L, Dorta M (1996) Ultrastructural aspects of endometrium in infertile women with septate uterus. Fertil Steril 65:750–752
Golan A, Langer R, Neuman M, Wexler S, Segev E, David MP (1992) Obstetric outcome in women with congenital uterine malformations. J Reprod Med 37:233–236
Tomaževič T, Ban-Frangež H, Ribič-Pucelj M, Premru-Sršen T, Verdenik I (2007) Small uterine septum is an important variable risk for preterm birth. Eur J Obstet Gynecol Reprod Biol 135:154–157
Grimbizis GF, Gordts S, Di Spiezio Sardo A, Brucker S, De Angelis C, Gergolet M et al (2013) The ESHRE/EGSE consensus on the classification of female genital tract congenital anomalies. Hum Reprod 28:2032–2044
Acknowledgments
Special thanks to Drs. Maria Teresa Iammarino and Alessandro Paccapelo, Statisticians of the Department of Clinical Medicine, University of Bologna, Bologna, Italy for their assistance in statistical analysis.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Paradisi, R., Barzanti, R., Natali, F. et al. Hysteroscopic metroplasty: reproductive outcome in relation to septum size. Arch Gynecol Obstet 289, 671–676 (2014). https://doi.org/10.1007/s00404-013-3003-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-013-3003-9