
Abstract
Objective
The objective was to evaluate the effects of infertility and its duration on female sexual functions.
Materials and methods
One-hundred and seventy-four (21.5 %) primary infertile cases, who attended the infertility outpatient clinic of our hospital, with a mean age of 31.2 ± 3.8 (range 20–45), have been determined as study group. In addition, 635 (78.5 %) cases with a mean age of 32 ± 3.2 (range 17–45) years, which attended the gynecology outpatient clinic with various complaints, were included as the control group. Infertile cases were grouped into three according to infertility duration: less than 2 years (Group I), 2–5 years (Group II), and 5 years and longer (Group III). Sexual dysfunction was evaluated via Turkish version of female sexual function index (FSFI) in the women who accepted to participate in this research.
Results
All the 809 cases incorporated in our study were found to be at risk for sexual dysfunction. Upon comparison between infertile and fertile groups, no meaningful statistical difference was determined within the scores of desire, arousal, lubrication, orgasm, sexual satisfaction, pain and total FSFI parameters (p > 0.05). The assessment on infertility durations showed that only sexual satisfaction scores were similar, whereas all other parameter scores and total FSFI scores were different significantly between all three groups. The scores got meaningfully lower as infertility duration of the couples extends (p < 0.05).
Conclusions
As the infertility duration extends, the scores of all parameters, except sexual satisfaction, decreases. But as many factors play a role in female sexual dysfunction, to blame prolonged infertility as a situation that negatively affects female sexual life, prospectively designed studies should be performed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although female sexual dysfunctions are more common than that of males, there is limited scientific research on this subject. Today, it has been suggested that connection between body and mind is associated with many sexual problems in females [1]. Various etiological factors including advanced age, chronic diseases, urinary incontinence and menopause play a role in female sexual dysfunction [2–5]. In this study, the effects of infertility and its duration on female sexual functions were evaluated.
Materials and methods
One-hundred and seventy-four (21.5 %) women with primary infertility, who attended the infertility outpatient clinic of our hospital, with a mean age of 31.2 ± 3.8 (range 20–45), have been determined as study group. In addition, 635 (78.5 %) cases with a mean age of 32 ± 3.2 (range 17–45) years, which attended the gynecology outpatient clinic with various complaints, were included as the control group. Infertile cases were grouped into three according to infertility duration: less than 2 years (Group I), 2–5 years (Group II), and 5 years and longer (Group III). Group I consisted of 65, Group II consisted of 67 and Group III consisted of 42 patients. The mean ages of the groups were 31.3 ± 5.3, 29.4 ± 4.1, and 33.0 ± 6.6 years, respectively. Sexual dysfunction was evaluated via Turkish version of female sexual function index (FSFI) in the women who accepted to participate in this research [6]. FSFI questionnaire comprises 19 questions including desire, arousal, lubrication, orgasm, sexual satisfaction and pain parameters. Points given for each topic changed between 0 and 5 and the score was calculated using multipliers of the factors. The cases with a total FSFI score below 26.55 were considered to be risky in terms of sexual dysfunction [7]. One-hundred and forty-two patients that have not completed or returned the forms were not included in the study. Those non-responders could not be compared with the responder cases. Pregnant women, women that attended the oncology policlinic, women with abnormal uterine bleeding and those attended the emergency room were excluded from the study. In addition, illiterate women and those with an education level inadequate to understand or answer the questions were also excluded from the study.
Mann–Whitney U, one way ANOVA and post-hoc tests were used for statistical analyses.
Informed consents were obtained from all participants. Approval of the Hospital Education Planning Committee that consists of the physicians responsible from the education of the assistant doctors and ethical aspects of the studies performed at the hospital was obtained.
Results
Of the 809 cases that completed the FSFI form, 174 (21.5 %) were infertile and 635 (78.5 %) were fertile. Their mean age was in turn 31.2 ± 3.8 and 32 ± 3.2 years. No significant difference was observed between the mean ages of the groups (p > 0.05).
Grouping the infertile subjects according to infertility duration, it was found that Group I consisted of 65, Group II consisted of 67 and Group III consisted of 42 patients. The mean ages of the groups were 31.3 ± 5.3, 29.4 ± 4.1 and 33.0 ± 6.6 years, respectively. There was no significant difference between the mean ages of the groups (p > 0.05). All the 809 cases incorporated in the study were found to be at risk for sexual dysfunction. Upon comparison between infertile and fertile groups, no meaningful statistical difference was determined within the scores of desire, arousal, lubrication, orgasm, sexual satisfaction, pain and total FSFI parameters (p > 0.05) (Table 1).
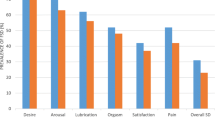
Comparing Group I, II and III, score of each parameter, except for sexual satisfaction, and total FSFI score were significantly different between all three groups. The scores got meaningfully lower as infertility duration of the couples extends (p < 0.05) (Table 2).
Discussion
Female sexual dysfunction is a multifactorial condition likely to be associated with numerous anatomical, physiological and psychological factors and likely to affect woman’s self-confidence, quality of life, mental status and relationships [2]. Sexual dysfunctions are age-related, progressive and common conditions and the degree of stress caused by this condition remains indefinite [3]. It is known that aging and menopause cause lubrication disorders [3]. Obesity, lower urinary tract symptoms, urinary incontinence and education level seem to have a role in sexual dysfunction [4, 5, 7–10]. In addition, another factor that is well known to be related with the sexual behavior is the duration of the partnership. In the study of Klausmann, the variation of sexual motivation with the duration of the partnership was analyzed in a large sample of 1,865 students aged between 19 and 32 years. Main results found were as follows: sexual activity and satisfaction decline in both sexes; sexual desire only declines in women and desire for tenderness declines in men and rises in women [11].
Number of studies that investigate the effect of infertility on sexual dysfunctions is limited. Millheiser et al. investigated FSFI scores in 119 infertile and 99 healthy women aged between 18 and 45 years. They considered the cases with a total FSFI score below 26.55 to be risky in terms of sexual dysfunction. They detected sexual dysfunction in 25 % of fertile and 40 % of infertile subjects. They found the scores of desire and arousal parameters significantly lower in the infertile group as compared to the fertile group. They expressed that the number of coitus and masturbation was significantly rarer in the infertile group [12]. Audu et al. obtained sexual history from 97 infertile women by asking various questions and reported that sexual dysfunction is common. The prevalence of frigidity was 78.4 %, dyspareunia was 57.7 %, difficulty in sexual arousal was 20.6 % and difficulty in achieving orgasm was 20.6 %; however, the absence of a control group and undefined questionnaire form made the interpretation difficult [13]. Drosdzol et al. used FSFI, International erectile function index and short form 36 Health Survey forms to investigate effect of infertility on sexual dysfunction in 206 infertile and 190 fertile couples; they found no significant difference between infertile and fertile women in terms of clinical sexual dysfunction (17.5 and 12.1 %, respectively; p = 0.13). The same study found clinically significant erectile dysfunction in 23.9 % of infertile males and in 13.7 % of male controls. Male infertility was determined to be the parameter that has most unfavorable effect on male sexual dysfunction [14]. Monga et al. evaluated 18 infertile couples and 12 couples seeking for elective sterilization via three questionnaires and found that infertility has no significant effect on female sexual dysfunction; however, International erectile function index scores and coitus satisfaction scores were found lower in infertile males [15]. Hurwitz et al. evaluated 40 couples with primary infertility, detected increased sexual dysfunction in 50 % of females during fertile phase of menstrual cycle, and reported loss of libido as the leading cause of dysfunction [16]. In the review of Wischmann et al., we see that sexual dysfunctions are unusual causes of involuntary childlessness, but sexual disorders caused by diagnosis and medical therapy are common in infertile couples, especially in women [17].
In the present study, all the cases were found to be at risk for sexual dysfunction. In addition, 142 patients did not complete or return the forms. This can be explained by the general Islamic community and its tabus about putting sexuality into words and confessing sexual satisfaction, especially in women. On the other hand, this study incorporates the women with primary infertility who attended the infertility outpatient clinic of our hospital and the women who attended the gynecology outpatient clinic with various complaints. It is very likely to see sexual dysfunction in women with different kinds of gynecologic complaints. FSFI scores of a randomly chosen women population at the out of the hospital will be expected to be higher. No significant difference was found between fertile and infertile groups in terms of scores of none of the parameters and total FSFI score. Comparing the groups according to infertility duration, scores of all parameters, except for sexual satisfaction, and total FSFI score were found significantly different between all three groups. The scores got meaningfully lower as infertility duration of the couples extends. This situation may originate not only from the duration of infertility but also from the extended duration of the partnership. Since the present study has not evaluated partners of the females, effect of male infertility on female sexual dysfunction could not be identified.
In conclusion, infertility may be one of the important conditions that can cause sexual dysfunction. But as many factors play a role in female sexual dysfunction, to blame prolonged infertility as a situation that negatively affects female sexual life, prospectively designed studies should be performed.
References
Ben-Zion IZ, Shiber A (2004) Female sexual dysfunction. Harefuah 143(6):417–419
Bronner G (2006) Female sexual function and chronic diseases. Harefuah 145(2):114–116
Davis AR (2000) Recent advances in female sexual dysfunction. Curr Psychiatry 2(3):211–214
Sako T, Inove M, Watanabe T, İshii A, Yokoyama T, Kumon H (2011) Impact of overactive bladder and lower urinary tract symptoms on sexual health in Japanese women. Int Urogynecol 22(2):165–169. doi:10.1007/s00192-010-1250-x
Lin ZS, Qion LX, Ximg P (2003) New progress on diagnosis and treatment of female sexual dysfunction. Zhonghua Nan ke Xue 9(6):457–461
Oksuz E, Malhan S (2005) Reliability and validity of the female sexual index in Turkish population. Sendrom 17:54–60
Rosen R, Brown C, Heiman J, Leiblum S et al (2000) The female sexual function Index (FSFI): a multidimensional self report instrument for the assessment of female sexual function. J Sex Marital Ther 26(2):191–208
Song SH, Jeon H, Kim SW, Paick JS, Son H (2008) The prevalence and risk factors of female sexual dysfunction in young Korean women: an internet- based survey. J Sex Med 5(7):1694–1701
Abu Ali RM, Hajeni RM, Khader Y, Ajlouni KM (2009) Factors associated with sexual dysfunction in Jordanian women and their sexual attitudes. Ann Saudi Med 29(4):270–274
Singh JC, Tharyan P, Kekre NS, Singh G, Gopalakrishman G (2009) Prevalence and risk factors for female sexual dysfunction in women attending a medical clinic in South India. J Postgrad Med 55(2):113–120
Klausmann D (2002) Sexual motivation and the duration of partnership. Arch Sex Behav 31(3):275–287
Millheiser LS, Helmer AE, Quintero RB, Westphal LM, Milki AA, Lathi RB (2010) Is infertility a risk factor for female sexual dysfunction? A case- control study. Fertil Steril 94(6):2022–2025
Audu BM (2002) Sexual dysfunction among infertile Nigerian women. J Obstet Gynaecol 22(6):655–657
Drosdzol A, Skrzypulec V (2008) Quality of life and sexual functioning of Polish infertile couples. Eur J Contracept Reprod Health Care 13(3):271–281
Monga M, Alexandrescu B, Katz SE, Stein M, Ganiats T (2004) Impact of infertility on quality of life, marital adjustment, and sexual function. Urology 63(1):126–130
Hurwitz MB (1989) Sexual dysfunction associated with infertility: a comparison of sexual function during the fertile and the non-fertile phase of the menstrual cycle. S Afr Med J 76(2):58–61
Wischmann TH (2010) Sexual disorders in infertile couples. J Sex Med 7:1868–1876
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iris, A., Aydogan Kirmizi, D. & Taner, C.E. Effects of infertility and infertility duration on female sexual functions. Arch Gynecol Obstet 287, 809–812 (2013). https://doi.org/10.1007/s00404-012-2633-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-012-2633-7