
Abstract
Introduction
Combined hip and upper-extremity fractures raise clinical concerns because upper-extremity fractures may hinder early mobilization, thereby affecting rehabilitation and mortality. This systematic review and meta-analysis aimed to evaluate the effects of combined upper-extremity and hip fractures on rehabilitation and mortality.
Materials and methods
We systematically searched MEDLINE, Embase, and the Cochrane Library for studies published before March 20, 2022, that evaluated the impact of concomitant upper-extremity injuries in geriatric patients with hip fractures. The pooled analysis identified differences in the (1) length of hospital stay, (2) discharge destination, and (3) mortality rates between the isolated and combined hip fracture groups.
Results
A total of 217,233 patients with isolated hip fractures (n = 203,816) and combined hip and upper-extremity fractures (n = 13,417) from 12 studies were analyzed. The average length of hospital stay was significantly longer in the combined upper-extremity fracture group than in the isolated hip fracture group (mean difference = 1.67 days; 95% confidence interval [CI] 0.63–2.70; P = 0.002). Patients in the combined upper limb fracture group were less likely to be discharged directly home (odds ratio [OR] = 0.64; 95% CI 0.52–0.80; P < 0.001) and showed significantly higher 30-day mortality (OR = 1.44; 95% CI 1.32–1.58; P < 0.001). The mortality rate after 30 days was not significantly different between the two groups.
Conclusions
Concomitant upper-extremity fractures have debilitating effects on rehabilitation and early mortality in geriatric patients with hip fractures. Therefore, more focus should be placed on the early ambulation of patients with hip fractures and simultaneous upper limb fractures to promote rehabilitation and alleviate the public health burden.
Level of evidence
III meta-analysis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The growth in the global senile population has resulted in an increased incidence of geriatric hip fractures. It is estimated that there will be a 2.28-fold and 1.59-fold increase in the Asian hip fracture incidence and medical costs, respectively, by the year 2050 [1]. Patients with hip fractures are among the oldest and most fragile orthopedic patients. The overall 1-month mortality rate following hip fracture is 13.3%; the 3 to 6-month mortality, 15.8%; and the 1-year mortality, 24.5% [2]. Given the scale of this condition, optimal and cost-effective hip fracture care is critical. Standardized hip fracture care, including early mobilization and rehabilitation, is known to minimize mortality and healthcare expenditure [3, 4].
Combined hip and upper-extremity fractures are rare; however, due to the recent increase in hip fracture incidence among the global aging population, the incidence of concomitant injuries warrants attention [5,6,7]. Furthermore, combined fractures raise clinical concern because upper-extremity fractures may hinder early mobilization and rehabilitation, thereby affecting the hospitalization period and mortality.
To the best of our knowledge, only one cohort study comprising of a small meta-analysis was conducted on the impact of concomitant wrist injuries in geriatric patients with hip fractures in 2015 [8], however, this study was limited to the investigation of wrist fractures and performed a single-arm meta-analysis of only three studies. Several newly updated comparative studies have been published; however, to the best of our knowledge, no meta-analysis has directly compared the outcomes of combined hip and total upper-extremity fractures with those of isolated hip fractures in a large number of studies [9,10,11,12,13,14,15,16].
Therefore, in the current study, we aimed to evaluate the effects of combined upper-extremity and geriatric hip fractures on the length of hospital stay, discharge destination, and mortality rate in direct comparison with the effects of isolated hip fractures using double-arm meta-analyses.
Materials and methods
This study was performed in accordance with the revised assessment of multiple systematic reviews and preferred reporting items for systematic reviews and meta-analysis guidelines [17, 18].
Literature search
In accordance with the referenced guidelines, we searched MEDLINE, Embase, and Cochrane Library for studies that evaluated the impact of concomitant upper-extremity injuries in geriatric patients with hip fractures. Using an a priori search strategy, we identified articles published up to March 20, 2022. The search terms included synonyms and terms related to combined hip and upper-extremity fractures as follows: (“hip” OR “proximal fem*”) AND (“fracture*”) AND (“concurrent” OR “simultaneous” OR “concomitant” OR “coincident” OR “combined”) AND (“upper” OR “humer*” OR “elbow” OR “wrist” OR “radi*”). We placed no restrictions on the language or publication year. After the initial electronic search, the relevant articles and their bibliographies were manually searched.
Study selection
Using titles and abstracts, two board-certified orthopedic surgeons trained in adult hip reconstruction and trauma surgery (CHK and HSK) independently selected studies for full-text review. If the data from the abstract were insufficient to make a decision regarding article inclusion, the full article was reviewed.
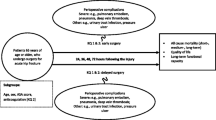
The inclusion criteria were as follows: (1) design type: a clinical randomized controlled trial, prospective cohort study, retrospective cohort study (RCS), or case–control study; (2) study subjects treated for hip fractures; and (3) comparison of postoperative outcomes between the isolated hip fracture and combined hip and upper-extremity fracture groups. The exclusion criteria were as follows: (1) non-original articles and (2) duplicate articles from the same investigation group.
We calculated the kappa values at each stage of the literature search to determine the inter-reviewer agreement for study selection. We correlated the agreement between reviewers based on the following kappa values: κ = 1.0, perfect agreement; 1.0 > κ ≥ 0.8, almost perfect agreement; 0.8 > κ ≥ 0.6, substantial agreement; 0.6 > κ ≥ 0.4, moderate agreement; 0.4 > κ ≥ 0.2, fair agreement; and κ < 0.2, slight agreement.
Data extraction
All extracted data were recorded independently by two investigators, and all disagreements were resolved by discussion. The following information and variables were extracted using a standardized form from the selected studies for qualitative data synthesis: (1) year and country of publication, (2) sample size, (3) age, (4) sex, (5) anatomic sites of upper limb fractures analyzed in the study, and (6) study design.
For the meta-analyses, the following outcome variables were collected: (1) length of hospital stay, (2) number of patients who were discharged home, (3) mortality within 30 days postoperatively, and (4) mortality beyond 30 days postoperatively.
Risk-of-bias assessment
We assessed the methodological quality of the included studies using the Methodological Index for Non-randomized Studies (MINORS) [19], a valid tool for assessing the quality of non-randomized studies. The maximum MINORS checklist score for the comparative studies was 24. Two independent reviewers performed the quality assessments, and any disagreements were resolved through discussion.
Data synthesis and statistical analyses
Heterogeneity in the study results was assessed using chi-squared and I2 tests. In cases of high heterogeneity (P ≤ 0.05, I2 > 50%), a random-effects model was used, whereas in cases of acceptable heterogeneity (P > 0.05, I2 ≤ 50%), a fixed-effects model was used. Comparisons of dichotomous data were reported by odds ratios (ORs) and 95% confidence intervals (CIs), and continuous variables were analyzed as mean ± standard deviation and compared on the basis of mean differences (MDs). Forest plots were used to present the meta-analysis results. Statistical significance was set at P < 0.05. We did not perform a test for publication bias because it is recommended only when at least 10 studies are included in the meta-analysis [20]. Data analyses were performed using RevMan (Review Manager) version 5.4 (The Cochrane Collaboration) and R (R Foundation for Statistical Computing).
Results
Study identification
The primary search yielded 1712 studies, of which 844 duplicates were excluded. Eight additional articles were identified through manual search. After careful review of the titles and abstracts, 854 articles were excluded. Full-text articles were retrieved and reviewed, resulting in the exclusion of 10 studies. Ultimately, 12 cohort studies were included (Fig. 1) [6, 8,9,10,11,12,13,14,15,16, 21, 22]. The inter-reviewer agreement was substantial (κ = 0.704) at the title review stage, almost perfect at the abstract review stage (κ = 0.814), and perfect at the full-text review stage (κ = 1.0).

The PRISMA flow diagram of study selection
Study characteristics
Of the 12 studies, nine were retrospective in nature [8, 10,11,12, 14,15,16, 21, 22], and the other three were prospective studies [6, 9, 13]. A total of 217,233 patients with isolated hip fractures (n = 203,816) and combined hip and upper-extremity fractures (n = 13,417) were analyzed. The mean age of both the isolated and combined hip fracture cohorts in all the studies was > 70 years. Likewise, all 12 studies in both cohorts included more female than male participants. Five studies investigated wrist or distal radius fractures [8, 9, 12, 14, 22], three included both wrist and proximal humerus fractures [13, 15, 21], and one investigated only proximal humerus fractures [10]. Three other studies included wrist and proximal humerus, as well as all other upper-extremity fractures in the shoulder, upper arm, elbow, forearm, and hand regions [6, 11, 16]. The overall incidence of concomitant upper limb fractures was 6.2%. The additional details are presented in Table 1.
Risk-of-bias assessment
The mean MINORS score for methodological quality assessment was 18.4 (range 17–20; Table 1). All 11 studies received point deductions for (1) a lack of double-blind evaluation of subject endpoints and (2) a lack of prospective sample size calculation from the eight main evaluation parameters. Nine studies [8, 10,11,12, 14,15,16, 21, 22] received point deductions owing to their retrospective design. In the “baseline equivalence of the group” domain, one point was deducted in one study [8] while another study [10] scored zero for the absence of baseline characteristic analysis.
Quantitative data synthesis (meta-analysis)
Length of hospital stay
Eleven studies were included to compare the average length of hospital stay between the isolated and combined fracture groups [6, 9,10,11,12,13,14,15,16, 21, 22]. The results of the heterogeneity analysis showed high heterogeneity among the studies (P < 0.001, I2 = 78%). The details are shown in Fig. 2A (MD = 1.67; 95% CI 0.63–2.70; P = 0.002). The mean length of hospital stay was significantly longer in the combined upper limb fracture group than in the isolated hip fracture group.

A forest plot of the length of hospital stay in the isolated hip fracture group compared with that in the combined upper-extremity fracture group
Discharge destination
Four studies [10, 13, 14, 16] reported the discharge destination. The meta-analysis revealed that patients in the combined upper limb fracture group were less likely to be discharged directly home (OR = 0.64; 95% CI 0.52–0.80; P < 0.001; I2 = 53%) than those in the isolated hip fracture group. The results are shown in Fig. 3.

A forest plot of the percentage of patients discharged home in the isolated hip fracture group compared with that in the combined upper-extremity fracture group
Mortality
Nine studies [6, 8,9,10, 13,14,15,16, 22] assessed the 30-day mortality associated with isolated hip fractures in comparison with that associated with the combined upper limb fracture groups. The pooled estimate revealed significantly higher 30-day mortality in the combined upper limb fracture group (OR = 1.44; 95% CI 1.32–1.58; P < 0.001), with moderate heterogeneity (P = 0.05; I2 = 49%; Fig. 4A).

A forest plot of A ≤ 30-day mortality and B > 30-day mortality in the isolated hip fracture group compared with that in the combined upper limb fracture group
Six studies [6, 8,9,10, 13, 15] reported a mortality rate of > 30 days; no significant differences were found between the isolated hip fracture and combined upper limb fracture groups (OR, 0.93; 95% CI 0.78–1.11; P = 0.43; I2 = 24%), as shown in Fig. 4B.
Discussion
The principal findings of this pooled analysis were that compared with the patients in the isolated hip fracture group, those in the combined hip and upper-extremity fracture group (1) required a longer average length of hospital stay, (2) were less likely to be discharged directly home, and (3) had higher 30-day mortality.
In this meta-analysis, the mean length of hospital stay was significantly longer in the combined upper-extremity and hip fracture group. Although two studies [9, 14] concluded that there were no significant differences between the two groups, the other included studies favored longer hospital stays for the combined fracture groups. Although conflicts may exist owing to differences in healthcare systems among countries, the facts that the results varied between the two groups from the same country [14, 15] and that the other studies were from various other countries support our findings. The average length of hospital stay is an important indicator of healthcare expenditure, clinical efficiency, and outcomes [23] and increased hospital stay among patients with simultaneous hip and upper limb fractures indicates that this subset of geriatric patients with hip fractures requires more rigorous acute management in an inpatient facility, which inevitably incurs a higher financial cost.
According to our meta-analysis, patients with geriatric hip fractures and concomitant upper limb fractures are at a higher risk of discharge to postoperative rehabilitation facilities. To the best of our knowledge, this is the first meta-analysis evaluating this parameter. Early ambulation within 48 h of a hip fracture surgery is critical for functional rehabilitation and is correlated with less discharge to rehabilitation facilities [24,25,26]. As hip fracture patients require walking aids to facilitate early postoperative ambulation, concomitant injuries to the upper limb result in a debilitating effect on mobilization and rehabilitation. In a matched pair study, Tow et al. demonstrated that a smaller number of patients with combined wrist fractures were able to ambulate at discharge (12 vs. 21, P = 0.049) [27]. Ng et al. also indicated that concurrent upper limb fractures require longer rehabilitation after discharge to rehabilitation facilities (mean: 34.6 versus 19.9 days, P = 0.009) [14]. Extended hospitalization is also indicative of an increased burden on healthcare resources. Therefore, more focus should be placed on the early ambulation of patients with hip fractures with simultaneous upper limb fractures to facilitate better outcomes and decrease both the length of hospital stay and the need for assistance with rehabilitation in care facilities.
A previous meta-analysis on the differences in mortality between isolated hip fracture and concurrent wrist fracture groups showed that both 30-day and beyond 30-day mortality had no significant differences [8]. However, this study pooled only three studies, including their own RCS, for a single-arm meta-analysis. Our study is the first well-structured meta-analysis to analyze mortality associated with all concurrent upper limb fractures in geriatric patients with hip fractures, not only within but also beyond the 30-day mark. In our study, the 30-day mortality was higher in the combined fracture group than in the isolated hip fracture group, although mortality beyond 30 days showed no significant differences. This analysis supports our initial hypothesis that simultaneous upper-extremity and hip fractures result in higher early mortality due to failure in mobilization of patients with these fractures early in the acute postoperative stage. Moreover, several other studies have indicated that early mobilization of patients with hip fractures reduces the in-hospital 30-day mortality [4, 25, 28].
The current study had several limitations. First, we could not include outcome variables that assess the degree of rehabilitation, such as the Barthel Index (BI), Instrumental Activities of Daily Living (IADL), and Motor Functional Independence Measure (FIM), owing to the lack of comparable data in the included studies. Di Monaco et al. showed that concomitant shoulder fractures resulted in a lower median BI after rehabilitation (70 vs. 90, P = 0.003) [21]. Dubljanin-Raspopović et al. compared motor FIM gain and IADL scores at the 4-month follow-up between patients with hip fractures with and without concomitant wrist fractures and found no significant differences [9]. Lin et al. assessed the BI of patients with concomitant wrist fractures at the 6-month follow-up and found no significant differences (75.7 vs. 75.1, P = 0.831) [12]. As these measures are more direct means of evaluating functional rehabilitation than the length of hospital stay and discharge destination, further studies should be undertaken to investigate these measures. Second, our study was limited by the fact that most of the included studies were retrospective cohort studies. As the absolute incidence rate of combined hip and upper limb fractures is relatively small, it is difficult to perform randomized controlled trials. Third, the results of the meta-analysis of the length of hospital stay showed high heterogeneity, which poses a potential risk of bias in interpreting the synthetic results. Regardless, this study has the following strengths: (1) it is the first to pool all concomitant upper-extremity fractures for analysis, not confined to just a systematic review. A meta-analysis is a widely accepted ‘gold standard’ modality for evidence synthesis and provides a powerful means of looking across datasets [29]; (2) it included a larger number of studies than previous meta-analyses; (3) it is the first meta-analysis to evaluate discharge destination; and (4) it successfully correlated rehabilitation difficulty and higher early mortality in the combined upper limb fracture groups.
Conclusion
Collectively, this meta-analysis revealed that concomitant upper-extremity fractures have debilitating effects on rehabilitation and early mortality in geriatric patients with hip fractures. Therefore, more focus should be placed on the early ambulation of patients with hip fractures and simultaneous upper limb fractures to promote rehabilitation and alleviate the public health burden.
References
Cheung CL, Ang SB, Chadha M, Chow ES, Chung YS, Hew FL, Jaisamrarn U, Ng H, Takeuchi Y, Wu CH, Xia W, Yu J, Fujiwara S (2018) An updated hip fracture projection in Asia: the Asian Federation of Osteoporosis Societies study. Osteoporos Sarcopenia 4:16–21. https://doi.org/10.1016/j.afos.2018.03.003
Hu F, Jiang C, Shen J, Tang P, Wang Y (2012) Preoperative predictors for mortality following hip fracture surgery: a systematic review and meta-analysis. Injury 43:676–685. https://doi.org/10.1016/j.injury.2011.05.017
Siu AL, Penrod JD, Boockvar KS, Koval K, Strauss E, Morrison RS (2006) Early ambulation after hip fracture: effects on function and mortality. Arch Intern Med 166:766–771. https://doi.org/10.1001/archinte.166.7.766
Heiden JJ, Goodin SR, Mormino MA, Siebler JC, Putnam SM, Lyden ER, Tao MA (2021) Early ambulation after hip fracture surgery is associated with decreased 30-day mortality. J Am Acad Orthop Surg 29:e238–e242. https://doi.org/10.5435/jaaos-d-20-00554
Buecking B, Wack C, Oberkircher L, Ruchholtz S, Eschbach D (2012) Do concomitant fractures with hip fractures influence complication rate and functional outcome? Clin Orthop Relat Res 470:3596–3606. https://doi.org/10.1007/s11999-012-2419-z
Robinson PM, Harrison T, Cook A, Parker MJ (2012) Orthopaedic injuries associated with hip fractures in those aged over 60 years: a study of patterns of injury and outcomes for 1971 patients. Injury 43:1131–1134. https://doi.org/10.1016/j.injury.2012.03.012
Schoeneberg C, Pass B, Oberkircher L, Rascher K, Knobe M, Neuerburg C, Lendemans S, Aigner R (2021) Impact of concomitant injuries in geriatric patients with proximal femur fracture: an analysis of the Registry for Geriatric Trauma. Bone Jt J 103-b:1526–1533. https://doi.org/10.1302/0301-620x.103b9.Bjj-2021-0358.R1
Uzoigwe CE, Venkatesan M, Johnson N, Lee K, Magaji S, Cutler L (2015) Influence of coincident distal radius fracture in patients with hip fracture: single-centre series and meta-analysis. J Orthop Traumatol 16:93–97. https://doi.org/10.1007/s10195-013-0281-8
Dubljanin-Raspopović E, Lj MD, Kadija M, Tomanović Vujadinović S, Tulić G, Selaković I, Aleksić M (2019) Simultaneous hip and distal radius fractures-does it make a difference with respect to rehabilitation? Geriatrics (Basel). https://doi.org/10.3390/geriatrics4040066
Haque A, Singh HP (2020) Mortality following combined fractures of the hip and proximal humerus. World J Orthop 11:426–430. https://doi.org/10.5312/wjo.v11.i10.426
Kang SW, Shin WC, Moon NH, Suh KT (2019) Concomitant hip and upper extremity fracture in elderly patients: Prevalence and clinical implications. Injury 50:2045–2048. https://doi.org/10.1016/j.injury.2019.09.010
Lin YP, Hung SH, Su YP, Feng CK, Liu CL, Chiu FY (2015) Concomitant hip and distal radius fractures. J Chin Med Assoc 78:304–307. https://doi.org/10.1016/j.jcma.2014.12.005
Morris DLJ, Nightingale JM, Geoghegan JM, Moran CG (2020) Concurrent upper limb and hip fracture in the elderly. Injury 51:1025–1030. https://doi.org/10.1016/j.injury.2020.02.073
Ng A, Mattin A, Seymour H, McKinnon E (2019) Comparison of outcomes between hip fracture patients with concurrent upper limb injuries and patients with an isolated hip fracture. ANZ J Surg 89:57–60. https://doi.org/10.1111/ans.14942
Siaw VWS, Kim S, Hakendorf P, Horwood C, To T (2017) Concomitant upper limb and hip fractures in older adults—does the site matter? A retrospective clinical observation study. J Clin Gerontol Geriatr 8:47–51. https://doi.org/10.24816/jcgg.2017.v8i2.02
Thayer MK, Kleweno CP, Lyons VH, Taitsman LA (2018) Concomitant upper extremity fracture worsens outcomes in elderly patients with hip fracture. Geriatr Orthop Surg Rehabil. https://doi.org/10.1177/2151459318776101
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, Group P-P (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4:1. https://doi.org/10.1186/2046-4053-4-1
Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, Porter AC, Tugwell P, Moher D, Bouter LM (2007) Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol 7:10. https://doi.org/10.1186/1471-2288-7-10
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73:712–716. https://doi.org/10.1046/j.1445-2197.2003.02748.x
Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (2022) Cochrane handbook for systematic reviews of interventions version 6.3 Cochrane. www.training.cochrane.org/handbook. Accessed 30 Mar 2022
Di Monaco M, Castiglioni C, Vallero F, Di Monaco R, Tappero R (2015) Concomitant upper limb fractures and short-term functional recovery in hip fracture patients: does the site of upper limb injury matter? Am J Phys Med Rehabil/Assoc Acad Physiatr 94:366–372. https://doi.org/10.1097/PHM.0000000000000191
Mulhall KJ, Ahmed A, Khan Y, Masterson E (2002) Simultaneous hip and upper limb fracture in the elderly: incidence, features and management considerations. Injury 33:29–31. https://doi.org/10.1016/s0020-1383(01)00097-3
Rotter T, Kinsman L, James EL, Machotta A, Gothe H, Willis J, Snow P, Kugler J (2010) Clinical pathways: effects on professional practice, patient outcomes, length of stay and hospital costs. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD006632.pub2
Lee KJ, Um SH, Kim YH (2020) Postoperative rehabilitation after hip fracture: a literature review. Hip Pelvis 32:125–131. https://doi.org/10.5371/hp.2020.32.3.125
Goubar A, Martin FC, Potter C, Jones GD, Sackley C, Ayis S, Sheehan KJ (2021) The 30-day survival and recovery after hip fracture by timing of mobilization and dementia: a UK database study. Bone Jt J 103-b:1317–1324. https://doi.org/10.1302/0301-620x.103b7.Bjj-2020-2349.R1
Oldmeadow LB, Edwards ER, Kimmel LA, Kipen E, Robertson VJ, Bailey MJ (2006) No rest for the wounded: early ambulation after hip surgery accelerates recovery. ANZ J Surg 76:607–611. https://doi.org/10.1111/j.1445-2197.2006.03786.x
Tow BPB, Chua BSY, Fook-Chong S, Howe TS (2009) Concurrent fractures of the hip and wrist: a matched analysis of elderly patients. Injury 40:385–387. https://doi.org/10.1016/j.injury.2008.09.013
Ferris H, Brent L, Coughlan T (2020) Early mobilisation reduces the risk of in-hospital mortality following hip fracture. Eur Geriatr Med 11:527–533. https://doi.org/10.1007/s41999-020-00317-y
Haddaway NR (2015) A call for better reporting of conservation research data for use in meta-analyses. Conserv Biol 29:1242–1245. https://doi.org/10.1111/cobi.12449
Funding
No funding was involved in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Ethics approval
No ethical approval was retrieved because data from previous published studies, in which informed consent was obtained by primary investigators, are to be retrieved and analysed.
Informed consent
No additional informed consent was necessary since informed consent was obtained by primary investigators of previous published studies analysed in this study, and all investigations were conducted in conformity with ethical principles of research.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kim, H.S., Lee, J.E., Choi, R.J. et al. Impact of concomitant upper-extremity injuries in patients with hip fractures: a systematic review and meta-analysis. Arch Orthop Trauma Surg 143, 3795–3802 (2023). https://doi.org/10.1007/s00402-022-04608-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-022-04608-w