
Abstract
Introduction
Traditionally surgeons have treated failed shoulder instability with open capsulolabral repair. Despite improved instrumentation, technique and familiarity in shoulder arthroscopy, few studies have reported the outcomes of arthroscopic revision shoulder instability repair. The purpose of this study was to assess clinical outcomes in patients following revision shoulder arthroscopic anterior capsulolabral stabilization.
Materials and methods
Sixty-two patients (63 shoulders) with failure of primary instability repairs were treated with revision arthroscopic anterior shoulder stabilization at a mean follow-up of 46.9 ± 16.8 months (range 18–78). Clinical outcomes were evaluated using validated patient-reported outcome questionnaires including the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, visual analog pain scale and Western Ontario Shoulder Instability Index. In addition, patients were queried for recurrent instability events (subluxation or dislocation) or revision surgery.
Results
At final follow-up, the mean postoperative Western Ontario Shoulder Instability normalized score was 80.1 ± 18.7 (range 15.0–100). There were clinically significant improvements in American Shoulder and Elbow Surgeons scores, Simple Shoulder Test scores and ten-point visual analog scale for pain (P < 0.001). Recurrent instability occurred in 12 shoulders (19.0 %), with number of prior surgeries and hyperlaxity found to be significant risk factor for failure (P < 0.001 and P = 0.04, respectively).
Conclusion
Revision arthroscopic anterior stabilization of the shoulder can result in satisfactory outcomes in appropriately selected patients who have failed previous capsulolabral repair. An increased number of prior surgeries and hyperlaxity are predictive of poor outcome.
Study design
Case series, LOE IV.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the absence of significant glenoid bone loss, arthroscopic anterior capsulolabral repair is widely accepted as the treatment of choice in patients undergoing primary surgery for shoulder instability. However, recurrent shoulder instability following primary shoulder stabilization presents a difficult problem for both the patient and the surgeon. Revision shoulder stabilization has historically been treated via open surgery, with the reported rates of recurrent instability following open revision Bankart repair range from 0 to 39 % [1, 10, 12, 21, 25, 32]. More recently, arthroscopic revision stabilization for recurrent shoulder instability has become more popular secondary to increased surgeon familiarity with arthroscopic techniques and improvements in arthroscopic instrumentation and implants [7, 11, 17]. Lesions that were once considered to be an indication for open surgery are now treatable arthroscopically [5, 27]. In addition, arthroscopic approaches are less invasive and with minimal alteration of the subscapularis [3, 4, 6]. Subsequently, the reduced morbidity of arthroscopic surgery may result in early functional rehabilitation and improved range of motion [16, 27].
The purpose of this study was to determine clinical outcomes in patients following revision arthroscopic anterior capsulolabral stabilization of the shoulder. The specific aims were to determine the rate of failure, identify risk factors for recurrence of instability, and report on subjective patient-reported outcomes. The hypothesis was that revision arthroscopic stabilization would offer satisfactory clinical outcomes in appropriately selected patients.
Materials and methods
Patients
After obtaining approval by Institutional Review Board of Rush University Medical Center (August 30, 2014; 13060505-IRB01), this study was performed retrospectively by reviewing the outcomes of patient who were treated from July 2007 to June 2012. The clinical and operating records of four sports medicine fellowship-trained orthopedic surgeons were examined to identify patients with shoulder instability who had been previously treated with either open or arthroscopic soft tissue stabilization and went to develop recurrent instability requiring revision surgery. Medical records were reviewed to obtain details of previous surgical procedures, history of recurrent instability and hand dominance. From the operative notes of the revision procedure, details regarding size of the capsulolabral defect, number of anchors used, and amount of glenoid bone loss were recorded.
Through mail-in and online-based survey, the identified patients were contacted and queried regarding symptoms of recurrent instability, satisfaction with surgery, ability to participate in sports, and if further surgery had been performed since the arthroscopic revision stabilization procedure. Patients also were asked to complete the following validated questionnaires: Western Ontario Shoulder Instability Index (WOSI), American Shoulder and Elbow Surgeons (ASES) shoulder assessment form, Simple Shoulder Test (SST) and visual analog scale (VAS) for pain. Clinical scores from patients who had recurrent instability after the revision surgery, as well as those that underwent additional arthroscopic soft tissue were considered in the analysis. However, patient-reported outcome scores from those who went onto have bony or soft tissue augmentation procedures were not included in the analysis, as the study sought to assess outcome scores after arthroscopic soft tissue stabilization procedures rather than augmentation procedures.
Surgical technique
All patients had magnetic resonance imaging of their shoulder to verifying capsulolabral lesion before surgery (Fig. 1). The surgeries were performed by one of four sports medicine fellowship-trained orthopedic surgeons. The choice of general anesthesia or regional block was determined by patient preference. Examination under anesthesia was performed to assess degree and direction of instability. Hyperlaxity was defined as shoulder that the examiner can easily subluxate the humeral head out of the socket anteriorly and posteriorly on drawer testing (2+ or greater laxity) and inferiorly with sulcus testing [14, 18].

Axial proton density MRI of right shoulder showing anterior glenoid labrum with macerated appearance (red arrow), large joint effusion (blue arrow) and bone marrow edema (white arrow) of the humeral head
Following evaluation under anesthesia, patients were placed in a lateral decubitus position on a beanbag and the operative extremity was placed in traction with 10 pounds of in line traction and 10 pounds of abduction traction. The shoulder was abducted approximately 50° and flexed 15°. Diagnostic arthroscopy was performed through standard posterior and anterosuperior portals. Particular attention was paid to evaluate glenoid bone loss and assess for defects of the humeral head as computer tomography (CT) scan was not routinely acquired preoperatively. The decision to proceed with arthroscopic revision stabilization was made after ruling out an inverted-pear glenoid and confirming that glenoid bone loss was not significant (<25 %) with the aid of a graduated probe [22]. The labrum was carefully assessed and mobilized with an elevator. The edge of the glenoid rim was carefully debrided to remove fibrous tissue and prepare a bleeding bony bed. Position of the first anchor, suture passing and tying was dependent on surgeon preference and injury characteristics. Only sutured anchors were used. Anteroinferior and 7 o’clock portals were frequently used and inferior-to-superior capsular plication sutures were placed in the inferior and posterior–inferior capsular tissue of all cases [10]. This technique of the arthroscopic management of shoulder instability has been previously published [10, 28]. Capsulolabral tissues were probed for stability after the repair and suture plication was performed as necessary. Rotator interval closure was performed if the space was deemed to be redundant and according to surgeon preference.
Postoperative rehabilitation
All procedures were performed as outpatient cases. Patients followed the same postoperative rehabilitation protocol, which involved shoulder immobilization in a sling for 4–6 weeks. The sling was removed during this period only for hygiene activities and therapeutic exercises. Initial therapy consisted of passive exercises with 90° of forward elevation, 45° of abduction and 20° of external rotation. After 4–6 weeks, slings were discontinued and scapular stabilization exercises were initiated. Patients were progressed to active range of motion to 60° abduction with internal rotation behind the back to waist level, 140° of forward flexion, and 40° of external rotation with the arm at the side. At 8 weeks, patients were progressed to full active motion as tolerated and advanced to gentle strengthening. After 12 weeks, patients began functional progression back to work, sports-related activities and advanced weight training. At 6 months after surgery, unrestricted return to sports and work was permitted.
Statistics
Failure was defined as recurrent episodes of dislocation or symptomatic instability after the revision procedure. GraphPad program (GraphPad Inc., La Jolla, CA, USA) was used for all analyses. Continuous variables were recorded as mean and one standard deviation. The Wilcoxon matched-pairs signed-rank test was used to evaluate the differences between the preoperative and postoperative functional scores and the Mann–Whitney test was used for unpaired data. The instability group was compared to the non-instability group in univariate analysis using two-sample t tests and Fischer’s exact tests. Results were considered statistically significant at P < 0.05.
Results
During the study period, 169 patients that underwent revision stabilization procedures for anterior shoulder instability with or without hyperlaxity were identified. After excluding 73 patients with large bony defects (>25 % bone loss of the glenoid) that underwent revision Latarjet or distal tibial allograft procedures (49 and 24 during the same period of data collection, respectively) and three patients whose index procedures were coracoid transfer procedures (Bristow or Latarjet), 93 patients were identified. Of the remaining 93 patients, 14 patients with workers compensation cases were excluded. Therefore, 79 patients (80 shoulders) with follow-up greater than 12 months were eligible for inclusion in the study, with 62 (78.4 %) patients available for mean follow-up of 46.9 ± 16.8 (range 18–78). There were 46 male patients and 16 female patients with a mean age of 23.3 ± 6.9 years (range 15–58) at time of revision surgery. The dominant extremity was involved in 54.1 % of patients (Table 1). Patients had an average of 1.17 surgeries (all patients had one or two prior surgeries except for one patient who had four surgeries: two arthroscopic capsular procedures, one open Bankart and one capsular shrinkage procedure) before undergoing revision surgery.
Sixty-two of 79 patients were successfully contacted for a follow-up rate of 78.4 %. Despite extensive attempts to locate them, 17 patients were not locatable (Fig. 2). At the time of arthroscopic revision capsulolabral repair, it was noted that twelve patients (13 shoulders) had an underlying diagnosis of hyperlaxity. Intra-operatively, using the 360° circle concept, the overall mean degree of capsulolabral injury was 151 ± 44°. On average, 4.41 ± 1.55 suture anchors were used for the revision procedure and rotator interval closure was performed in 7 (11.3 %) shoulders.

Patient flowchart
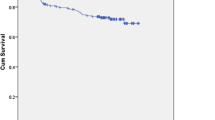
The mean follow-up duration after revision arthroscopic stabilization was 46.9 months (range 18–78 months). Follow-up in 74.1 % of patients was greater than 30 months after their revision procedure. With regard to patient-reported outcome scores, there were significant increases seen in postoperative ASES (P < 0.001) and SST scores (P < 0.001) with significant decreases in VAS pain scores postoperatively (P < 0.05). These values are shown in Table 2. Preoperative WOSI scores were not available, but at final follow-up, the mean normalized WOSI was 80.1 ± 18.7. Majority of patients (74.2 %) were able to return to at least recreational level of sports.
Following arthroscopic revision stabilization, recurrent instability occurred in 11 patients (17.7 %) and in 12 shoulders (19.0 %). Two shoulders had symptomatic subluxations, while ten shoulders experienced frank dislocations. The cause was mild trauma that occurred during daily activities of living (without the involvement of any significant external force) in 5 (45.5 %) shoulders, moderate trauma that occurred during activities similar to the level of sporting activity in 2 (18.2 %) shoulders, and major trauma caused by significant external force in 5 (45.5 %) shoulders. Of the 11 patients who had recurrent instability, seven patients (eight shoulders) underwent additional stabilization procedures, with a mean time to repeat surgery of 32 months (range 7–51 months). There were four open Latarjet procedures, two distal tibial allograft transplants to augment the glenoid, one additional arthroscopic capsulolabral stabilization, and one open capsular stabilization with rotator interval closure using semitendinosus allograft.
The 11 patients who had recurrence of instability were compared to 51 patients who did not have further instability to determine potential risk factors related to failure. The number of prior surgeries (P < 0.001) and presence of hyperlaxity (P = 0.04) were found to be significantly associated with failure (Table 3). Between the two groups, there was no significant difference in the number of suture anchors used, size of capsular injury, age at time of surgery, and gender.
Discussion
This study sought to quantify the surgical effectiveness of arthroscopic revision anterior capsulolabral stabilization in patients that previously had shoulder stabilization procedures. The most important finding of this study is that of the 62 patients (63 shoulders) treated with arthroscopic revision surgery and followed up at a mean of 46.9 months, 11 patients (12 shoulders) failed with recurrent dislocations. These results are in keeping with the current published evidence on arthroscopic revision shoulder stabilization [1, 18, 20, 25, 26]. Furthermore, this study confirms previous papers that the overall recurrence is twice that number of primary arthroscopic Bankart repair [1, 4, 18].
Reported redislocation rates following revision arthroscopic capsulolabral repair range from 0 to 27 % in the literature. In 1996, Lehmann et al. [20] reported on the first published series using an arthroscopic revision stabilization technique in 14 patients. They reported no recurrence at only 13-month follow-up following arthroscopic suture repair. In another series, Bartl et al. [4] prospectively evaluated 56 patients who underwent arthroscopic revision stabilization with suture anchors via the 5:30 approach. In their series, six patients (11 %) experienced recurrent instability after revision with those failures correlating with poor capsular quality noted at the time of surgery [4]. Of the six failures, one patient had glenoid bone loss measuring 20 % of the glenoid width and all others had smaller glenoid compression defects, ranging from 5 to 15 %. Using a similar operative technique, Patel et al. [27] reported a 10 % recurrence rate over a 36-month period with good clinical outcomes. Neri et al. [26] reported a recurrence rate of 27 % (3 of 11) after a mean follow-up duration of 34 months after using a suture anchor repair technique with a high rate of rotator interval closure. Arce et al. [2] published their results following arthroscopic revision stabilization in 16 patients with three cases of recurrent shoulder instability. In their study, the three patients who experience redislocation all had two prior surgeries [2]. In a recent systematic review by Abouali et al. [1], the overall rate of recurrent instability was 14.2 %. Similarly, Creighton et al. [10] have previously reported a failure rate of 17 % at a mean follow-up of 30 months, which is similar to the current series with a failure rate of 17.7 % (11 of 62 patients) at a mean follow-up of 46.9 months.
The reported recurrence rate following open revision procedures is comparable to arthroscopic techniques and ranges between 8 and 26 % [30, 33]. However, arthroscopy has become increasingly popular and is continuing to evolve. While being less invasive, arthroscopy allows closer inspection of the joint and labral structures with less scarring, stiffness and minimal subscapularis alteration [13]. In a study of 26 shoulders that underwent open revision stabilization after a failed arthroscopic procedure, Cho et al. [9] reported a recurrent instability rate of 11.5 %. Despite positive results in recurrence rates, the authors also noted significant decreases in active forward flexion and external rotation, presumably due to the prolonged avoidance of external rotation following open surgery. They concluded that the open procedure led to loss of motion which undermined return to previous sports activity level [9]. In 2012, Schmid et al. [31] reported 14 % rate of failure following Latarjet procedure for treatment of recurrent glenohumeral instability after previous operative repair. Forty-eight of the 49 consecutive patients in their study showed an osseous defect of the anterior–inferior glenoid rim on preoperative CT scan, with an average superoinferior extension of the damage of 17.7 mm [31]. Following Latarjet procedure, six cases of complications were noted which included four cases of delayed wound healing and two other cases frozen shoulder [31].
Previously reported reasons for redislocation include hyperlaxity, not utilizing enough suture anchors, glenoid bone loss, humeral head defect and return to contact sports [1, 2, 6, 9]. Failure analysis in this series showed that recurrent instability was the result of moderate to severe trauma in 7 of 12 (58.3 %) shoulders. Two of seven traumatic failures had signs of hyperlaxity. Remaining five shoulders that sustained atraumatic recurrent dislocations all displayed signs of hyperlaxity. One shoulder with recurrent instability had an estimated intraoperative glenoid bone loss measuring 25 %, with the remaining 11 shoulders exhibiting less glenoid bone loss ranging from 0 to 10 % of the glenoid width. Bartl et al. [4] showed a significant correlation between younger age and recurrent instability after revision arthroscopic shoulder stabilization (22.6 year in unstable shoulders vs 30.8 years for stable shoulders). In contrast, Meehan et al. [24] showed that age greater than 30 years at the time of revision surgery was a negative prognostic factor. The reported results from this study do not support either studies as there were no statistical differences in age between stable and unstable shoulders (23.6 ± 5.9 vs 23.1 ± 7.2 years, respectively, P = 0.83).
There were significant differences in the number of previous surgeries when comparing patients who had recurrent instability and those who were stable after revision surgery. A cohort study by Krueger et al. [19] compared the outcome of arthroscopic revision surgery with results of primary arthroscopic instability repair using the same suture anchor technique. In their series, no patient in either group experienced recurrent instability, but the revision group had significantly lower scores in subjective outcome measures (Walch-Duplay score, Melbourne Instability Shoulder score, Western Ontario Shoulder Instability Index and Subjective Shoulder Value). Multiple surgeries can negatively affect bone and soft tissue quality, decrease available sites for anchor placement, reduce healing capacity, and subsequently increase the overall complexity of the case [19]. Moreover, patients with inherently poor tissue quality would be predisposed to failure after surgery and such patients may undergo greater number of additional procedures.
Despite the failures, the current study reveals that patients undergoing revision arthroscopic shoulder stabilization generally had satisfactory outcomes. A high percentage of patients were able to return to recreational sports (74.2 %). The subjective patient-reported outcomes in this study are similar to those seen in previous reports on revision arthroscopic shoulder stabilization. The reported mean ASES score ranges from 76 to 99.6 in the literature [8, 10, 27], which is consistent with the findings in this patient population (mean ASES 85.1). Kim et al. [16] and Neri et al. [26] reported post-revision normalized SST scores of 91.7 and 95.4, respectively, which is again similar to postoperative SST score of 90.9 from this study. With respect to WOSI score, Krueger et al. [19] reported a mean score of 68.5 after revision arthroscopic stabilization compared to mean score of 89.8 after primary surgery. The authors reported that the revision group more often feared falling on their shoulders and had more difficulties in maintaining their levels of fitness, thus likely attaining lower scores on emotion and lifestyle subitems on the WOSI questionnaire. This study’s patients’ mean WOSI score of 80.1 is higher than the revision stabilization group score but lower than the primary group score reported by Krueger et al. [19]. The reason for higher overall WOSI score in this patient population after revision surgery is not exactly clear. One reason may be secondary to the difference in ability to in return to sports (30 % in Krueger et al. [19] vs 74.2 % in present study). As previously reported, “the ability to participate in sports seems to play an important role in this young patient population” [15, 19].
The improvements seen in patients in this study suggest that the appropriately chosen patient can expect increased shoulder function and decreased pain with an arthroscopic capsulolabral repair for failed primary stabilization of the shoulder. The reported results support the use of arthroscopic techniques in revision stabilization procedures. Creighton et al. [10] have previously reported an aggressive surgical technique using multiple anchors and generally 120°–180° repair construct with similar results [10]. By plicating the inferior and posterior–inferior capsular tissue, it is possible to eliminate the redundant inferior capsular pouch and minimize recurrence rates.
Limitations
Our study has several limitations. The main limitation of the study is that we did not include in-person clinical evaluations. At the time of revision surgery, 43.5 % of patients were less than 20 years of age and we anticipated difficulties in attaining clinic follow-up visits with a young mobile population secondary to careers and education. Due to this obstacle, we chose to evaluate patient-reported outcomes (ASES, VAS, SST and WOSI) that were obtained via questionnaire. However, the primary goal of revision instability surgery (particularly from a patient perspective) is to eliminate shoulder instability events and allow a return to activities and sports. Both of these outcomes have been adequately evaluated using the current methodology. A further weakness of this study is that we report only the postoperative WOSI score. The WOSI is a quality of life questionnaire designed specifically for shoulder instability with excellent supporting evidence for reliability and responsiveness [29]. However, WOSI scores were not routinely obtained preoperatively from patients and as a result, we could not determine change in WOSI score. Moreover, preoperative shoulder CT scan was not routinely performed. Thus, we were unable to accurately quantify and characterize the amount of glenoid bone loss using a standardized method and comment on the percentage at which bone loss may be a risk factor for failure in arthroscopic capsulolabral revision surgery. Another possible weakness of the study includes performance bias which may result from combining outcome data from four surgeons. However, the inclusion of multiple surgeons adds to the generalizability of the results. In addition, follow-up imaging was not obtained for the current study. Longer term follow-up with radiographic imaging is necessary to better understand the natural disease progression and the implications of treatment. Previous studies showed that failures rates for arthroscopic capsulolabral repair increased when follow-up was beyond 5 years [8, 23].
Finally, this was a retrospective analysis with no control group. A high-quality randomized control trial comparing outcomes of arthroscopic versus open stabilization would best determine outcomes following revision surgery. However, it must be noted that with increasing availability and success of arthroscopic surgery along with the increased morbidity associated with open procedures, patients with failed instability surgery may not be willing to undergo open surgery. Finally, further study is needed to determine differences in outcome between arthroscopic, open soft tissue and open or arthroscopic bone transfer techniques for recurrent instability with specific attention to elimination of instability, restoration of motion, return to sport, and long-term risk of glenohumeral arthritis to help determine the most appropriate technique for this complex patient population.
The results of this study indicate that arthroscopic revision shoulder stabilization may result in high patient satisfaction rates and a high rate of return to sporting activity. Arthroscopic revision shoulder stabilization can provides a reliable treatment option in appropriately selected patients who have failed previous capsulolabral repair. Longer term studies are required to determine whether similar results are maintained over time.
References
Abouali JA, Hatzantoni K, Holtby R, Veillette C, Theodoropoulos J (2013) Revision arthroscopic Bankart repair. Arthroscopy 29:1572–1578
Arce G, Arcuri F, Ferro D, Pereira E (2012) Is selective arthroscopic revision beneficial for treating recurrent anterior shoulder instability? Clin Orthop Relat Res 470:965–971
Barnes CJ, Getelman MH, Snyder SJ (2009) Results of arthroscopic revision anterior shoulder reconstruction. Am J Sports Med 37:715–719
Bartl C, Schumann K, Paul J, Vogt S, Imhoff AB (2011) Arthroscopic capsulolabral revision repair for recurrent anterior shoulder instability. Am J Sports Med 39:511–518
Bedi A, Ryu RK (2010) Revision arthroscopic Bankart repair. Sports Med Arthrosc 18:130–139
Boileau P, Richou J, Lisai A, Chuinard C, Bicknell RT (2009) The role of arthroscopy in revision of failed open anterior stabilization of the shoulder. Arthroscopy 25:1075–1084
Bottoni CR, Smith EL, Berkowitz MJ, Towle RB, Moore JH (2006) Arthroscopic versus open shoulder stabilization for recurrent anterior instability: a prospective randomized clinical trial. Am J Sports Med 34:1730–1737
Castagna A, Garofalo R, Melito G, Markopoulos N, De Giorgi S (2010) The role of arthroscopy in the revision of failed Latarjet procedures. Musculoskelet Surg 94(Suppl 1):S47–S55
Cho NS, Yi JW, Lee BG, Rhee YG (2009) Revision open Bankart surgery after arthroscopic repair for traumatic anterior shoulder instability. Am J Sports Med 37:2158–2164
Creighton RA, Romeo AA, Brown FM Jr, Hayden JK, Verma NN (2007) Revision arthroscopic shoulder instability repair. Arthroscopy 23:703–709
Fabbriciani C, Milano G, Demontis A, Fadda S, Ziranu F, Mulas PD (2004) Arthroscopic versus open treatment of Bankart lesion of the shoulder: a prospective randomized study. Arthroscopy 20:456–462
Franceschi F, Longo UG, Ruzzini L, Rizzello G, Maffulli N, Denaro V (2008) Arthroscopic salvage of failed arthroscopic Bankart repair: a prospective study with a minimum follow-up of 4 years. Am J Sports Med 36:1330–1336
Gartsman GM, Roddey TS, Hammerman SM (2000) Arthroscopic treatment of anterior–inferior glenohumeral instability. Two to five-year follow-up. J Bone Joint Surg Am 82-A:991–1003
Gerber C, Nyffeler RW (2002) Classification of glenohumeral joint instability. Clin Orthop Relat Res 400:65–76
Gerometta A, Rosso C, Klouche S, Hardy P (2014) Arthroscopic Bankart shoulder stabilization in athletes: return to sports and functional outcomes. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-2984-7
Kim SH, Ha KI, Cho YB, Ryu BD, Oh I (2003) Arthroscopic anterior stabilization of the shoulder: two to six-year follow-up. J Bone Joint Surg Am 85-A:1511–1518
Kropf EJ, Tjoumakaris FP, Sekiya JK (2007) Arthroscopic shoulder stabilization: is there ever a need to open? Arthroscopy 23:779–784
Krueger D, Kraus N, Pauly S, Chen J, Scheibel M (2011) Subjective and objective outcome after revision arthroscopic stabilization for recurrent anterior instability versus initial shoulder stabilization. Am J Sports Med 39:71–77
Krueger D, Kraus N, Pauly S, Chen J, Scheibel M (2011) Subjective and objective outcome after revision arthroscopic stabilization for recurrent anterior instability versus initial shoulder stabilization. Am J Sports Med 39:71–77
Lehmann M, HaberMeyer P, Lichtenberg S, Werner A (1996) Arthroscopic revision surgery in shoulder instability. J Shoulder Elbow Surg 5:S67
Levine WN, Arroyo JS, Pollock RG, Flatow EL, Bigliani LU (2000) Open revision stabilization surgery for recurrent anterior glenohumeral instability. Am J Sports Med 28:156–160
Lo IK, Parten PM, Burkhart SS (2004) The inverted pear glenoid: an indicator of significant glenoid bone loss. Arthroscopy 20:169–174
Manta JP, Organ S, Nirschl RP, Pettrone FA (1997) Arthroscopic transglenoid suture capsulolabral repair. Five-year followup. Am J Sports Med 25:614–618
Meehan RE, Petersen SA (2005) Results and factors affecting outcome of revision surgery for shoulder instability. J Shoulder Elbow Surg 14:31–37
Millar NL, Murrell GA (2008) The effectiveness of arthroscopic stabilisation for failed open shoulder instability surgery. J Bone Joint Surg Br 90:745–750
Neri BR, Tuckman DV, Bravman JT, Yim D, Sahajpal DT, Rokito AS (2007) Arthroscopic revision of Bankart repair. J Shoulder Elbow Surg 16:419–424
Patel RV, Apostle K, Leith JM, Regan WD (2008) Revision arthroscopic capsulolabral reconstruction for recurrent instability of the shoulder. J Bone Joint Surg Br 90:1462–1467
Provencher MT, Ghodadra N, Romeo AA (2010) Arthroscopic management of anterior instability: pearls, pitfalls, and lessons learned. Orthop Clin North Am 41:325–337
Rouleau DM, Faber K, MacDermid JC (2010) Systematic review of patient-administered shoulder functional scores on instability. J Shoulder Elbow Surg 19:1121–1128
Rowe CR, Zarins B, Ciullo JV (1984) Recurrent anterior dislocation of the shoulder after surgical repair. Apparent causes of failure and treatment. J Bone Joint Surg Am 66:159–168
Schmid SL, Farshad M, Catanzaro S, Gerber C (2012) The Latarjet procedure for the treatment of recurrence of anterior instability of the shoulder after operative repair: a retrospective case series of forty-nine consecutive patients. J Bone Joint Surg Am 94:e75
Sisto DJ (2007) Revision of failed arthroscopic Bankart repairs. Am J Sports Med 35:537–541
Zabinski SJ, Callaway GH, Cohen S, Warren RF (1999) Revision shoulder stabilization: 2- to 10-year results. J Shoulder Elbow Surg 8:58–65
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
NN Verma is a consultant for Smith and Nephew, BJ Cole is a consultant for Arthrex, AA Romeo is a consultant for Arthrex, GP Nicholson is consultant for Tornier, and other authors have no potential conflicts of interest in relation to this article.
Rights and permissions
About this article

Cite this article
Shin, J.J., Mascarenhas, R., Patel, A.V. et al. Clinical outcomes following revision anterior shoulder arthroscopic capsulolabral stabilization. Arch Orthop Trauma Surg 135, 1553–1559 (2015). https://doi.org/10.1007/s00402-015-2294-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-015-2294-7