
Abstract
Introduction
The purpose of the study was to investigate differences in the osseous structure anatomy of male and female distal radii.
Methods
Morphometric data were obtained of 49 distal human cadaveric radii. An imprint of the distal edge was attained using silicone mass and the palmar cortical angle (PCA) of the lateral and intermediate column, here declared as medial, according to the concept of Rikli and Rigazzoni. The lateral and medial length and five widths were digitally measured by three observers. In order to compare the measurements an unpaired t test was used. To prove the reliability of the measurements an intraclass correlation analyses was done.
Results
Overall mean medial PCA was 148.25° (SD ± 6.83) and mean lateral PCA 156.07° (SD ± 7.00). In male specimens, the mean medial PCA was 147.38° (SD ± 6.01) and mean lateral PCA was 153.6° (SD ± 6.20) whereas in female specimens, the mean medial PCA was 149.41° (SD ± 7.79) and the mean lateral PCA 159.37° (SD ± 6.78), with statistical significance for the female lateral PCA. No gender significant difference for the medial PCA and no significant side difference for the PCA’s could be found. The ICC of the observers was r = 0.936 and 0.976 for the medial and for lateral PCA 0.957–0.984. The palmar cortical length of the distal radius was significantly longer in male specimens. For all widths, larger values for male radii were measured, being statistically significant in all cases.
Conclusion
Male dimensions concerning the wide were significantly larger when compared with females. Regarding the PCA at the medial and lateral column, we found significant difference for lateral PCA concerning the gender. Overall, study results demonstrated an angle of 148.25° ± 6.83 for the medial PCA and 156.07° ± 7.00 for the lateral PCA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Limited contact internal locking plates are considered to be the gold standard in treating distal radius fractures. Anatomical precontoured plates were developed to restore the distal radius in its original anatomical position. The shape and contour of the plates and locking screw mechanism are continuously improved, and the manufacturers of the anatomical plates claim that no intraoperative adjustment like bending is necessary. The distal edge of palmar locking plates is designed to be placed against the watershed line. In theory and under the condition that the plate fits the anatomy, it functions as a template and can be used for reduction by performing the lift-off-technique as described by Schneppendahl et al. [1]. If reduction is performed properly, radiological parameters such as palmar tilt, radial inclination and ulnar variance should be restored to genuine conditions. The theory seems to be simple, but several studies showed that the initial anatomy cannot be reliably restored in all cases and that inadequate anatomic plate design can result in imprecise fracture reduction [2–4]. Buzzel et al. [5] were able to verify a plate-bone contact ranging from 3 to 6 % of the plate surface and concluded that the plate geometry could be optimized. One important parameter for plate geometry, which is not quantified in detail actually, could be the palmar cortical angle (PCA) of the distal radius cortex. The angle subtended between the palmar lip and the radius shaft in the majority of current available palmar plates differs between 155 and 165° (Table 1). The current plate designs do not take into account that the PCA differs between the medial and intermediate column according to the three-column-concept as described by Rikli and Regazzoni [6]. Although to the best of our knowledge there are only two scientific reports in the current literature addressing the slope of the medial and intermediate column [7, 8]. While both studies use CT scans for analyzing, no current study has investigated the PCA using negative imprints of the distal radius cortex.
The aim of this study was to independently obtain reliable morphometric data on differences in the anatomy of human distal radius concerning angle and size differences and in dependence of gender and side. It was hypothesized that the angle of the lateral column differs from that of the medial column. Furthermore it was aimed to find out whether there is need for gender-specific plate designs.
Methods and materials
Material
The surface anatomy of the distal radius was studied in 49 macerated human cadaver radii. There were 21 left-sided and 28 right-sided specimens from 28 male and 21 female donors with a mean age of 79 years (range 60–91) and 81 years (range 56–93).
All body donors consented in writing during their lifetime to the use of their body for research and education. Standard radiographs of the wrist were obtained to exclude any severe degenerative or posttraumatic changes which might have influenced the parameters.
Two equal casts were taken from each palmar cortex, beginning at the epiphyseal area and ending at the radius shaft using a special C-silicone mass with low shrinkage for accurate results (Optosil® Comfort Putty by Heraeus Kulzer, Inc. (Hanau, Germany)). For each radius cast, the authors created longitudinal and transversal slices using a manual slicing machine to gain the same section thickness for each slice. Thickness for the transversal slices was 3.0 mm and thickness for the longitudinal slices 1.3 mm. The authors took two longitudinal slices, basing on the three-column concept from Rikli and Rigazzoni [6]. One slice was taken from the center of the lateral column and one slice from the center of the medial column. All slices were scanned by a flatbed scanner and then digitally measured using the software Image J 1.48 [9].
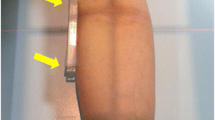
Six measurements beginning at the epiphysis and ending at the diaphysis were performed for each radius cast cut in transversal direction to measure the palmar cortical width (PCW), defined as the width of the palmar radius cortex from the ulnar to the radial side. The slice with the transversal cutting plane projecting 3 mm behind the scapholunate facet of the distal radius was defined as reference point “0” for the first width measurement as these section planes correspond to the watershed line. This measurement was repeated 3, 6, 9, 12 and 15 mm behind the reference point (Fig. 1). Three observers (JO, MW, and JW) measured each slice. All observers were blinded to prior measurements by the other observers. All examiners received an intensive review of the measurement method before the study.

Left side Distal radius, side views from the ulnar side. The red line displays the cutting plane “0”. +, Lunar facet; *, Scaphoid facet. Right side Cast sliced in transversional direction. The yellow highlighted slice is the slice in cutting plane 0, followed by slice 3–15
Two measurements were carried out on each longitudinal slice for the lateral and medial side (lateral and medial column) (Fig. 2). The first was the palmar cortical angle (PCA), defined as the angle between a first line drawn parallel to the palmar cortex of the distal radius epiphysis and a second line drawn concurrent to the radius diaphysis. The second was the palmar cortical length (PCL), defined as the length of the palmar radius cortex between the vertex of the PCA and the distal end of the radius epiphysis (Fig. 3).

Left side Distal radius, view from palmar. Green lateral column, blue medial column. The red lines demonstrate the cutting planes for the medial and lateral slices. Right side Cast cut in longitudinal direction. Green Slice used for measurements on lateral column. Blue Slice used for measurements on medial column

Measurements on longitudinal slices. On the upper side is the slice from the medial column and on the lower side the slice from the lateral column. * PCA between blue and green line. The green line also indicates the palmar cortical length
Statistical analyses were performed using SPSS 22.0 (SPSS Inc., Chicago, IL, USA). Mean values, standard deviations and intraclass correlation coefficient (ICC) between the three observers were calculated. ICC values were assessed in a two-way mixed model with absolute agreement in 95 % confidence intervals. To validate that the PCWs, PCAs, and PCLs in the present groups fitted a Gaussian distribution, Kolmogorov–Smirnov tests were performed prior to statistical analysis. Statistical analysis was carried out using Student’s t test. The level of significance was set at p < 0.05. The two-tailed test was used in all cases.
Results
Palmar cortical angle
Overall significant differences could be found concerning the lateral PCA in contrast to the medial PCA (p < 0.01). Another significant difference exits between the lateral and medial length (p < 0.01). The overall angle for the medial PCA was 148.25° (SD ± 6.83) and the lateral PCA was 156.07° (SD ± 7.00).
The lateral PCA measured on male radii was different to the one measured on female radii. Male specimens showed a mean medial PCA of 147.38° (SD ± 6.01) and a mean lateral of 153.6° (SD ± 6.20) whereas in female specimens, the mean medial PCA was 149.41° (SD ± 7.79) and the mean lateral PCA 159.37° (SD ± 6.78). Hence, the lateral PCA of the female distal radii was significantly wider than the ones of the male distal radii (p = 0.003). No significance for the medial PCA could be found among males and females (p = 0.097) and there was no significant side difference for the PCA’s (Table 2). The ICC regarding medial PCA was between r = 0.936 and 0.976, for lateral PCA 0.957–0.984.
Palmar cortical length
Overall, the PCL of the distal radius was significantly longer in male if compared to female specimens (p < 0.001). The mean medial length was 11.86 mm (SD ± 1.77 mm) and the mean lateral length was 10.27 mm (SD ± 1.86 mm) in male specimens. For female specimens, the mean medial length was measured with 11.69 mm (SD ± 1.91 mm) and the lateral length with 9.81 mm (SD ± 2.46 mm) (Table 2).
The ICC ranged from 0.628 to 0.862 in length lateral and 0.813–0.93 in length medial measurements.
Palmar cortical width
The overall PCW was 26.79 mm (SD ± 2.92) on position B0 and as the radius becomes thinner up to its diaphysis, PCW on position B15 was 20.68 mm (SD ± 2.73). For all positions, larger values for male radii were measured, being statistically significant in all cases. The comparison between left and right-sided radii showed no significant difference (Table 2).
The ICC for the measurements regarding the width (B0 to B15) of the distal radii ranged between 0.813 and 0.970 overall.
Discussion
In this study, we investigated the morphometric data of the distal radius and the influence of gender and side. The study results showed that significant difference between the medial and lateral PCA could be found. The overall angle for the medial PCA was 148.25° (SD ± 6.83) and the lateral PCA 156.07° (SD ± 7.00). The analyses of the influence of gender showed that the lateral PCA of female specimens was significantly wider compared to the one of male specimens (159.37° ± 6.78–153.6° ± 6.20). The PCL was significantly longer in male specimens. Additionally, the width of male distal radius was significantly wider as the female’s, too.
Numerous studies have demonstrated the importance of anatomical restoration of distal radius fractures to reach good functional results and normal biomechanics of the wrist [10, 11]. Early in the history of trauma surgery, some authors, such as Gartland and Werly in 1951, pointed out that an acceptable reduction of distal radius fractures depends on the restoration of the palmar tilt [12]. Additionally Knirk and Jupiter noted that patients with an articular step off greater than 2 mm at the radiocarpal joint are involved in the danger of posttraumatic arthritis [13]. Most recently, it was demonstrated that a residual ulnar-positive deformity greater than 5 mm is associated with unsatisfactory postoperative outcome, the radio-ulnar deformity is also taken into account [14, 15]. Furthermore the posttraumatic instability of the distal radioulnar joint should be evaluated by a complex of clinical and radiological tests [16]. The dorsal capsular imbrication is a reliable and sufficient treatment option in these cases [17]. To reach the aim of anatomical reduction, precontoured distal radius plates need to have an anatomical correct shape. Vromen et al. considered that positioning anatomical plates may lead to residual errors in individual patients. The study showed a large variation in positioning, influenced by two factors: the subjective “best positioning” assessed by the surgeon and the plate design [3]. Although manufacturers claim that there is no need to bend distal radius locking plates, they nevertheless offer tools to bend them if necessary. In this case, it still remains unclear if the locking mechanism maintains its stability. Secondly, the screws could alter their angle and penetrate into the radiocarpal joint.
Additional requirements of the specific conditions of the distal radius anatomy are necessary. Studies concerning the distal radius geometry are rare. Pichler et al. investigated the different circular arc radiuses of the distal palmar radius on 100 radii. They showed that the circular arc radius differs between medial and lateral column of the distal radius [18]. In a study on 134 distal radii, Windisch et al. described an osseous prominence on the lateral column of the radius which rises on average 2.90 mm above the palmar cortex. They called it the promontorium of the radius and postulated to consider it developing new implants [19]. Andermahr et al. specified an analog osseous prominence on the ulnar side of the distal radius [20]. This prominence of the lunar joint facette seems to be particular sensitive for shearing forces; complications in surgical treatment have been reported [21]. Some studies deal with the geometry of the distal radius, but do not address the PCA as the majority of these studies ask for radiographic parameters to measure the outcome after distal radius fractures. Stevenson et al. compared the palmar tilt (PT), radial inclination (RI) and the ulnar variance (UV) pre- and postoperative in a retrospective study in 33 patients with distal radius fractures. Additionally they compared the parameters to the uninjured side. The mean correction of PT was 1° under correction, but with a range of 7.3–3.7 degree of overcorrection. Similar observations can also be made with the RI. Comparing the pre- and postoperative measurements the parameters have changed just slightly [22]. The authors did not state which plate was used and the measurements were only done by one observer. While interpreting these parameters it should be borne in mind that the position of the forearm while taking the X-ray influences these parameters. With the study of Mann et al. the effect of pronation or supination positioning of the forearm on the PT became apparent. Compared to a neutral position, pronation creates an increasing palmar tilt and supination brought a slight decrease in PT [14]. The side difference of the PT, RI and UV was examined by Hollevoet et al. on standard radiographs comparing 50 healthy volunteers. They pointed out that the variability of the right-left differences regarding these three parameters using the contralateral side is smaller than the variability of the whole group. It should be noted that the radiographs were taken with the forearm in neutral position and no degree of the lateral projection is given [23]. Despite the fact that no pairs of radii were used in our study, no significant influencing variable for PCA, PCL or PCW could be identified.
In a retrospective study, Patel et al. analyzed 60 cases of distal radius fractures, which were treated with open reduction and internal fixation (ORIF) using a DVR® plate. Comparing the PT, radial length(RL) and RI 3 months postoperative with normal values, significant differences for all parameters could be shown. Compared with the uninjured side, PT and RL were still significant; no difference was noted for RI [24]. Another retrospective study at 185 distal radius fractures treated with palmar locking plates (DVR® plates) created by Mignemi et al., showed that not even one half of the fractures achieved normal postoperative radiologic parameters regarding PT, RI and UV. This indicates that the tested plate in this study was not precontoured in an anatomically correct shape.
In all these studies, some radiological parameters were taken into account, but the PCA has not been investigated in this context. The majority of distal radius plates are curved to align with the PCA of the distal radius cortex. The PCA of the currently available plates differs; values spread between 155 and 165°, without being gender specific (Table 2). Anatomical studies concerning the PCA are rare. Bassi et al. measured the PCA on fifty lateral radiographs of normal wrists and found a mean value of 143° (130–154°) [25]. These findings were confirmed by Agir et al., they observed the differences of PCA using 18 intact cadaver radii. The mean PCA was 142.27° ± 6.76. They concluded that the PCA is variable and they suggested that preoperative measuring of the contralateral side can be adjusted to the true palmar angle [26]. Both authors measured the PCA on lateral X-ray photographs and did not decide between different columns.
According to the concept of Rikli and Rigazzoni, Gasse et al. measured the PCA in the center of each column and compared them to each other. With a mean value of 155° (143–167°) for the lateral column and a mean value of 145° (134–153°) for the medial column they proved statistical difference (p < 0.0001) [7]. These findings were conducted by Evans et al. who studied 74 dry human radii. They found a mean overall PCA of 147° (SD ± 5), while the PCA for the lateral column was 149° and for the medial column 145.9°, being statistically different. They also correlated it to gender and found statistical difference between men (146.3°) and women (148.5°) [8].
In our study, both PCA’s, for the lateral and for the medial column are flatter as described by Evans. This could be achieved due to the fact that Evans et al. used computer tomography for their measurements and our bases for the presented data were imprints. The PCA of current available studies is similar with the PCA in this study as shown in Table 3.
In order to achieve an anatomically correct fit, it may become necessary to design new plates addressing the PCA difference between the lateral and medial column. An advantage of anatomical fitting could be seen during the reduction process of the distal fragment. A radius plate pre-shaped correctly according to anatomical structures would promote these objectives unequivocally.
How wide and how long the head of the plate can maximally be, are important questions for the manufacturers designing a new plate. In this context, it seems to be interesting that longer plate heads with more screw rows do not inevitably lead to more stability as Drobetz et al. [27] showed in a biomechanical study comparing single row to double row plates. Thus, it seems to be helpful to have several different plates to fit best for different radius dimensions. As the results of the presented study show, the width of the radii of male and female radii differs significantly. According to the study results, distal radius plates used in male specimens should have a distal width around 28.31 mm (SD ± 2.45), and become thinner, to be 21.81 mm ± 2.64 at 15 mm proximal to the watershed line. In contrast to this, distal radius plates used in female specimens should be smaller at each width, so on the level of the watershed line plates should have a width of 24.77 ± 2.20 and 15 mm proximal 19.16 mm ± 2.05.
Limitations of this paper are the use of dried cadaver specimens and the limited number of 49 distal radii. Moreover, due to the fact that no paired distal radii were used, the data for the side influence mirror the population but not the individual anatomy. The differences within one individual between left and right side are less as compared to other individuals.
Strength of the presented study is the use of a special C-silicone mass with low shrinkage for accurate results, so a perfect negative imprint could be created. Contrary to measurements at radiographs, the imprints would not be influenced by capture settings. The ICC with over 0.80 shows the high reliability of the measured parameters. The ICC considered as fair for values less than 0.41, moderate between 0.41 and 0.60, substantial between 0.61 and 0.80, and almost perfect between 0.81 and 1.00 [28].
In conclusion, we were able to demonstrate that with the present numbers, male dimensions concerning the width were significantly larger when compared with females. Regarding the PCA at the medial and lateral column, we found significant difference for the lateral PCA concerning the gender.
Overall, study results demonstrated an angle of 148.25° ± 6.83 for the medial PCA and 156.07° ± 7.00 for the lateral PCA.
Based on this finding, reflections should take place on whether gender-specific distal radius plates are necessary.
References
Schneppendahl J, Windolf J, Kaufmann R (2012) Distal radius fractures: current concepts. J Hand Surg Am 37(8):1718–1725
Oppermann J, Wacker M, Stein G et al (2014) Anatomical fit of seven different palmar distal radius plates. Arch Orthop Trauma Surg 134(10):1483–1489
Vroemen JC, Dobbe JG, Sierevelt IN, Strackee SD, Streekstra GJ (2013) Accuracy of distal radius positioning using an anatomical plate. Orthopedics 36(4):e457–e462
Mignemi ME, Byram IR, Wolfe CC et al (2013) Radiographic outcomes of volar locked plating for distal radius fractures. J Hand Surg Am 38(1):40–48
Buzzel JE, Weikert DR, Watson JT, Lee DH (2008) Precontoured fixed-angle volar distal radius plates: a comparison of anatomic fit. J Hand Surg Am 33(7):1144–1152
Rikli DA, Regazzoni P (1996) Fractures of the distal end of the radius treated by internal fixation and early function. A preliminary report of 20 cases. J Bone Joint Surg Br 78(4):588–592
Gasse N, Lepage D, Pem R et al (2011) Anatomical and radiological study applied to distal radius surgery. Arch Orthop Trauma Surg 33(6):485–490
Evans S, Ramasamy A, Deshmukh SC (2014) Distal volar radial plates: how anatomical are they? Orthop Traumatol Surg Res 100(3):293–295
Schneider CA, Rasband WS, Eliceiri KW (2012) NIH Image to Image J: 25 years of image analysis. Nat Methods 9(7):671–675
Figl M, Weninger P, Liska M, Hofbauer M, Leixnering M (2009) Volar fixed-angle plate osteosynthesis of unstable distal radius fractures: 12 months results. Arch Orthop Trauma Surg 129(5):661–669
Lerch SSH, Wilken F, Wittenberg CE (2009) Clinical and radiological results after distal radius fracture: intramedullary locking nail versus volar locking plate osteosynthesis. Z Orthop Unfall 147(5):547–552
Gartland JJ Jr, Werley CW (1951) Evaluation of healed Colles’ fractures. J Bone Joint Surg Am 33-A(4):895–907
Knirk JL, Jupiter JB (1986) Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 68(5):647–659
Mann FA, Kang SW, Gilula LA (1992) Normal palmar tilt: is dorsal tilting really normal? J Hand Surg Br 17(3):315–317
Altissimi M, Mancini GB, Bicocchi R (1983) Radiographic parameters of the distal epiphysis of the radius in the healthy and fractured wrist. Arch Putti Chir Organi Mov 33:367–370
Spies CK, Muller LP, Oppermann J, Hahn P, Unglaub F (2014) Instability of the distal radioulnar joint - an overview of clinical and radiological procedures regarding their efficacies. Handchir Mikrochir Plast Chir 46(3):137–150
Unglaub F, Manz S, Bruckner T et al (2013) Dorsal capsular imbrication for dorsal instability of the distal radioulnar joint. Oper Orthop Traumatol 25(6):609–614
Pichler W, Clement H, Hausleitner L et al (2008) Various circular arc radii of the distal volar radius and the implications on volar plate osteosynthesis. Orthopedics 31(12):89–91
Windisch G, Clement H, Tanzer K et al (2007) Promontory of radius: a new anatomical description on the distal radius. Surg Radiol Anat 29(8):629–633
Andermahr J, Lozano-Calderon S, Trafton T, Crisco JJ, Ring D (2006) The volar extension of the lunate facet of the distal radius: a quantitative anatomic study. J Hand Surg Am 31(6):892–895
Harness NG, Jupiter JB, Orbay JL, Raskin KB, Fernandez DL (2004) Loss of fixation of the volar lunate facet fragment in fractures of the distal part of the radius. J Bone Joint Surg Am 86-A(9):1900–1908
Stevenson I, Carnegie CA, Christie EM, Kumar K, Johnstone AJ (2009) Displaced distal radial fractures treated using volar locking plates: maintenance of normal anatomy. J Trauma 67(3):612–616
Hollevoet N, Van Maele G, Van Seymortier P, Verdonk R (2000) Comparison of palmar tilt, radial inclination and ulnar variance in left and right wrists. J Hand Surg Br 25(5):431–433
Patel S, Menendez PB, Hossain FS et al (2014) Does the DVR((R)) plate restore bony anatomy following distal radius fractures? Ann R Coll Surg Engl 96(1):49–54
Bassi RS, Krishnan KM, Dhillon SS, Deshmukh SC (2003) Palmar cortical angle of the distal radius: a radiological study. J Hand Surg Br 28(2):163–164
İsmail Agir, Mahmut Nedim Aytekin, Fatih Kückdurmaz, Onur Basci, Tetik C (2014) Distal radius measurements and efficacy of fixed-angle locking volar plates. Turk J Med Sci 44(1):36–41
Drobetz H, Weninger P, Grant C et al (2013) More is not necessarily better. A biomechanical study on distal screw numbers in volar locking distal radius plates. Injury 44(4):535–539
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33(1):159–174
Acknowledgments
J.O. and M.W. did not and will not receive any financial benefit in any form. The authors thank Justus Wenning (JW), who did one measurement series in scope of his scientific project. No benefits in any form have been received related directly or indirectly to the subject of this article.
Conflict of interest
There is no conflict of interest of all authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Oppermann, J., Bredow, J., Beyer, F. et al. Distal radius: anatomical morphometric gender characteristics. Do anatomical pre-shaped plates pay attention on it?. Arch Orthop Trauma Surg 135, 133–139 (2015). https://doi.org/10.1007/s00402-014-2112-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-014-2112-7