
Abstract
Introduction
Reducing allogeneic blood transfusions remains a challenge in total knee arthroplasty. Patients with preoperative anemia have a particularly high risk for perioperative blood transfusions.
Materials and methods
176 anemic patients (Hb < 13.5 g/dl) undergoing total knee replacement were prospectively evaluated to compare the effect of a perioperative cell saver (26 patients), intraoperative fibrin sealants (5 ml Evicel®, Johnson & Johnson Wound Management, Ethicon, Somerville, NJ) (45 patients), preoperative autologous blood donation (PABD) (21 patients), the combination of fibrin sealants and preoperative autologous blood donation (44) and no intervention (40 patients) on perioperative blood loss and transfusion requirements.
Results
All protocols resulted in significant reduction of allogeneic blood transfusions. Transfusion rates were similar with the use of PABD (19 %), Evicel® (18 %), and cell saver (19 %), all significantly lower than the control group (38 %, p < 0.05). Combining Evicel® with PABD resulted in significantly higher wastage of autologous units (p < 0.05) with no significant reduction in allogeneic transfusion rate (14 %). The use of fibrin sealant resulted in a significant reduction of blood loss compared to the PABD group (603 vs. 810 ml, p < 0.005) as well as the control group (603 vs. 822 ml, p < 0.005).
Conclusions
While PABD proved to be the most cost-effective treatment option in anemic patients, fibrin sealants and cell saver show similar reduction in allogeneic transfusion rates compared to controls. The combination of fibrin sealants and PABD is not cost-effective and increases the number of wasted units.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty is accompanied by significant peri- and postoperative blood loss putting patients at risk for allogeneic blood transfusions. In addition, approximately 24 % of the patients scheduled for total knee arthroplasty are anemic [1]. The baseline hemoglobin level is the strongest predictor for receiving postoperative blood transfusions [2, 3] and several studies have shown that there is no need for blood management in non-anemic patients [4, 5]. In addition, preoperative anemia and allogeneic blood transfusions are independently associated with an increased risk of morbidity and mortality [1, 6, 7] making patients with preoperative anemia the most important target for blood management.
The goal of blood management is to minimize the exposure to allogeneic blood transfusions. Potential health risks of allogeneic blood transfusions include the transmission of infectious disease, transfusion reaction, allergic reaction, and postoperative infection [8, 9]. Despite the improvement in safety of allogeneic blood with modern blood bank protocols, its potential risks are still a concern.
Preoperative autologous blood donation (PABD) represents the gold standard [10]. The optimal time for donation is 1 month prior to the surgery. Although PABD is associated with a significant reduction in allogeneic blood transfusion, patients have a higher overall likelihood of receiving blood units compared to patients without predonation [11–14]. In addition, PABD is accompanied with a high rate of wasted blood [8, 14–16] and the technique does not eliminate the risks of transfusion reactions, administrative errors or bacterial contamination [17].
Another alternative is the use of fibrin sealant, plasma fibrinogen mixed with thrombin [18]. When sprayed onto the wound the activation of fibrinogen by thrombin forms an adhesive fibrin clot [19–21]. In addition, perioperative drainage blood reinfusion devices are utilized to minimize exposure to allogeneic blood [22].
The current study attempts to answer the following research questions: (1) which of the blood management protocols achieves the most significant reduction in allogeneic blood transfusion as compared to controls with no intervention? (2) Do these protocols have an impact on postoperative blood loss? and (3) is there a difference in the overall cost?
Materials and methods
A retrospective review was conducted of 192 patients with a preoperative hemoglobin of less than 13.5 g/dl undergoing total knee arthroplasty by the senior authors between 2010 and 2012. All procedures were performed with a standardized mid-vastus or parapatellar approach under hypotensive spinal–epidural anesthesia. 16 patients were excluded because of preoperative treatment with blood thinners or the presence of a bleeding disorder leaving 176 patients eligible for the study. 31 males and 145 females were included with an average age of 68 years at the time of the surgery (range 27–90 years) and mean BMI of 25.5 kg/m2 (range 14–46 kg/m2). The study was approved by the Institutional Review Board at the authors’ Institution, and all patients gave their informed consent prior to their inclusion in the study.
Procedures were divided into five groups based on the method of blood management that was employed. Gender, age, BMI, preoperative Hb, date of preoperative Hb measurement, date of autologous blood donation, number of autologous transfusions, number of allogeneic transfusions, time of transfusion, and postoperative Hb levels until date of discharge, and in-house complications (thromboembolic events, cardiac events, bleeding, hematomas, and urinary tract infections) were documented. The volume of blood lost was calculated as the sum of intraoperative blood loss and the volume retrieved from drains. All drains were removed after 24 h.
Of 132 primary total knee arthroplasty procedures performed in anemic patients, 21 (16 %) donated autologous blood preoperatively, 26 (20 %) used a reinfusion device (OrthoPat®, Haemonetics, Braintree, MA), and 45 (34 %) received intraoperative fibrin sealant (5 ml Evicel®, Johnson & Johnson Wound Management, Ethicon, Somerville, NJ). 40 cases (30 %) had no intervention and served as controls. These patients were all operated by one of the two senior authors (FB) and each protocol was used for 7–9 months at a time between 2010 and 2012. A combination of PABD and Evicel® was used in 44 cases operated on by the second surgeon in the current study (CC). Patients received allogeneic transfusions if their hemoglobin level dropped below 8.0 g/dl and they displayed clinical symptoms of anemia (tachycardia and/or hypotension) despite an intravenous fluid bolus of 500 cc. The decision to transfuse autologous blood was made at the discretion of the anesthesiologist and medical attending, and strict transfusion guidelines were not enforced. All four groups were similar in terms of age, BMI, and American Society of Anesthesiologists (ASA) scores (Table 1).
The cost benefits were calculated considering the average cost of an autologous/allogeneic unit of blood of US $240, a type and cross fee of US $100, and a transfusion fee of US $100. Furthermore, one reinfusion device ran at US $438 and 5 ml of fibrin sealant cost US $505. Insurance reimbursement for preoperative donation or transfusion was not considered for this protocol.
Data were analyzed using ANOVA (Microsoft Excel, Microsoft Corporation, Redmond, WA, USA, Microsoft Office Professional Plus 2010 Version 14.0.6 for Windows 7). A p value of less than 0.05 was considered statistically significant (Table 2).
Results
Transfusion rates were similar with the use of PABD (19 %), Evicel® (18 %), and cell saver (19 %), all significantly lower than the control group (38 %, p < 0.05). Among patients who predonated autologous blood, 19 % required an allogeneic unit with an autologous wastage rate of 29 %. Combining Evicel® with PABD resulted in significantly higher wastage of autologous units (59 vs. 29 %; p < 0.05) with no significant reduction in allogeneic transfusion rate (14 %) (Fig. 1).

Percentage of patients in each group who received allogeneic blood
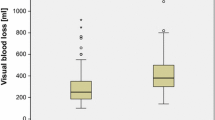
Wound drainage on the first postoperative day was found to be reduced in the fibrin sealant group as compared to PABD and cell saver (p < 0.05). The measured volume of blood lost in the topical fibrin sealant group averaged 603 ml, followed by the PABD group (810 ml, p < 0.05), the control group (822 ml, p < 0.05), and the cell saver group (905 ml, p < 0.05). However, after accounting for blood reinfused in the cell saver group, the blood loss of 759 ml is not significantly higher than the sealant group (p = 0.13) (Fig. 2).

Patients in the fibrin sealant group lost less blood intra- and postoperatively. No drains were use in the combination group
The mean hemoglobin level at discharge was similar in all groups regardless of the intervention, an average 3 g/dl drop from preoperative levels. The smallest drop was seen in the predonation group with 2.5 g/dl compared to 3.1 g/dl with Evicel® (p < 0.05). No postoperative complications or differences in length of hospital stay were noted among the four groups. The mean duration of hospital stay for all the patients was 3.8 days (range 2–10 days). Patients in all groups averaged a hospital stay of 4 days, except the combination PABD and Evicel group who were discharged after a mean 2.8 days (p < 0.001), highlighting the impact of postoperative transfusions on length of stay (Fig. 3).

All four groups did not differ significantly in hemoglobin levels at discharge (after transfusion)
The use of fibrin sealants resulted in a 26 % reduction in perioperative blood loss compared to the control group (p = 0.05). A similar reduction of 25 % was observed between the PABD group and the fibrin sealant group (p < 0.05), and 20 % when compared to the cell saver group (p = 0.13).
Cost analysis revealed highest cost per patient when Evicel® and PABD were combined (US $876/patient), followed by Evicel® (US $622/patient), cell saver (US $540/patient), and PABD alone (US $395/patient). All interventions were significantly more expensive than the control group (US $220/patient; p < 0.001) (Fig. 4).

Average cost per patient for each intervention
Discussion
The current retrospective study evaluates the efficacy of reinfusion devices, PABD, the use of fibrin sealants and the combination of both in anemic patients undergoing primary total knee arthroplasty.
All interventions proved to be similarly effective in reducing allogeneic transfusion rates compared to controls.
The administration of topical fibrin sealants has been shown to reduce blood loss as well as allogeneic transfusion risk in joint replacement [19–21]. In a prospective, multicenter, randomized study Levy et al. [20] demonstrated a significant reduction in blood loss compared to controls (360 vs. 878 ml), as well as lower transfusion rates (17 vs. 55 %), and a smaller drop in hemoglobin level (2.5 vs. 3.7 g/dl). The literature reveals a significant decrease in blood loss with the use of fibrin sealants (185 vs. 408 ml) in total knee and hip arthroplasty [21, 23], as well as a shorter hospital stay, superior range of motion, and decreased incidence of arthrofibrosis 5 months after the surgery [24]. Moreover, Mawatari et al. [25] reported reduced blood loss over the first 48 h postoperatively (580 vs. 810 ml) in a study in which all patients in the treatment and control groups predonated autologous blood. Whereas 20 % of patients in the control group lost more than 1,200 ml postoperatively, only 4 % of the patients who were treated with fibrin sealant registered such a volume of blood loss [25]. Although fibrin sealants resulted in a significant 20–25 % reduction in the current study, the reduction in blood loss was not as marked as that reported in other studies.
Cell saver can recover up to 60 % of the blood lost during total knee arthroplasty [22, 26]. Patients in the cell saver group were reinfused with an average 102 ml the day of surgery and 46 ml on postoperative day 1. A Cochrane review showed similar results with reinfusion of washed or unwashed blood in orthopedic trials. The relative risk of exposure to blood transfusion was reduced on average by 52 % with washed cell salvage and 53 % with unwashed cell salvage [27].
Preoperative donation reduces exposure to allogeneic blood, at the expense of a 2.5–2.7 times increased risk of receiving any transfusion (allogeneic and/or autologous) [8, 16]. The current study confirms that routine PABD for anemic patients significantly decreases the need for allogeneic blood. It is well established that the preoperative hemoglobin is the strongest predictor for postoperative transfusions [5, 8, 9, 14–16] and PABD seems to be especially effective in this high-risk group. In contrast, previous studies have revealed no benefit for non-anemic patients [4, 28]. Hatzidakis et al. [15] showed that up to 83 % of the predonated blood was discarded when PABD is utilized in non-anemic patients less than 65 years of age. The high rates of wasted autologous blood and the increased overall transfusion rates highlight the importance of selecting an appropriate group for an autologous donation protocol. This targeted approach in which patients are grouped by hemoglobin level is important to evaluate the efficacy and cost-benefit of blood-saving interventions in orthopedic surgery. Although a recent randomized-controlled trial found no significant difference in blood loss with the use of intra-articular fibrin sealants in TKA, the paper does not provide an independent calculation for anemic patients [29].
To our knowledge, there is no data in the literature about the concurrent use of fibrin sealants and PABD. This combination significantly reduced the number of autologous transfusions and the overall transfusion rate when compared to PABD alone, which reflected on a higher autologous wastage rate (59 vs. 29 %, respectively; p < 0.05).
Although no treatment at all is most cost-effective, the high rate of allogeneic blood transfusions makes it an unpractical approach. Among the treatment protocols that were tested, PABD remains the most cost-effective approach to blood management in anemic patients. A previous study from our center reported that while routine PABD is costly, limiting it to anemic patients only increases cost-effectiveness [4]. However, routine use of PABD with postoperative drains reduces its overall cost-effectiveness. Although reinfusion devices and fibrin sealants are more expensive they do not require the patient to spend time prior to surgery to donate blood and remain appealing treatment options for patients or centers that do not have PABD readily available. It is also important to notice that the difference in cost is related to the price of the cell saver and fibrin sealant. At lower prices, their effectiveness might be similar to PABD.
The current paper is limited by its retrospective and non-randomized nature. It is not clear whether the best cut-off for anemia is 13.5 g/dl or lower. Further studies are needed to answer these questions and it is likely that cut-off levels will differ from institution to institution based on anesthesia and surgical technique. It is worth mentioning although transfusion rates did not different significantly, drains were used in all groups except the combination group. Because hypotensive spinal anesthesia and its associated fluid substitution independently reduces hemoglobin and hematocrit, blood loss could not be reliably calculated based on hemoglobin drop and had to rely on the measurement of intraoperative blood loss and postoperative drain output. Comparing treatments during different time periods does add the potential problem that surgical or perioperative changes over time could affect transfusion rates. The senior surgeons did not change their surgical technique between 2010 and 2012 and utilized the same type of anesthesia and perioperative medications. In addition, larger sample sizes are needed to detect any significant difference in efficacy between various blood management modalities.
In conclusion, PABD proved to be the most cost-effective method in reducing allogeneic transfusions in anemic patients undergoing total knee arthroplasty. However, PABD requires a setup in place to adequately handle the blood units. Fibrin sealants and perioperative reinfusion devices both offer similar efficacy but are slightly more expensive. Fibrin sealants are appealing since they do not require preoperative blood donation or postoperative handling of a cell saver; however, their cost-effectiveness depends on the purchase price. The combination of fibrin sealants and PABD is not justified in primary TKA, as it significantly increases the cost and wastage with no benefit.
References
Spahn DR (2010) Anemia and patient blood management in hip and knee surgery: a systematic review of the literature. Anesthesiology 113(2):482–495. doi:10.1097/ALN.0b013e3181e08e97
Noticewala MS, Nyce JD, Wang W, Geller JA, Macaulay W (2012) Predicting need for allogeneic transfusion after total knee arthroplasty. J Arthroplast 27(6):961–967. doi:10.1016/j.arth.2011.10.008
Ahmed I, Chan JK, Jenkins P, Brenkel I, Walmsley P (2012) Estimating the transfusion risk following total knee arthroplasty. Orthopedics 35(10):e1465–e1471. doi:10.3928/01477447-20120919-13
Kim S, Altneu E, Monsef JB, King EA, Sculco TP, Boettner F (2011) Nonanemic patients do not benefit from autologous blood donation before total knee replacement. HSS J: Musculoskelet J Hosp Special Surg 7(2):141–144. doi:10.1007/s11420-011-9200-9
Salido JA, Marin LA, Gomez LA, Zorrilla P, Martinez C (2002) Preoperative hemoglobin levels and the need for transfusion after prosthetic hip and knee surgery: analysis of predictive factors. J Bone Joint Surg Am 84-A(2):216–220
Husted H, Holm G, Jacobsen S (2008) Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Acta Orthop 79(2):168–173. doi:10.1080/17453670710014941
Musallam KM, Tamim HM, Richards T, Spahn DR, Rosendaal FR, Habbal A, Khreiss M, Dahdaleh FS, Khavandi K, Sfeir PM, Soweid A, Hoballah JJ, Taher AT, Jamali FR (2011) Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study. Lancet 378(9800):1396–1407. doi:10.1016/S0140-6736(11)61381-0
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB (1999) An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 81(1):2–10
Bong MR, Patel V, Chang E, Issack PS, Hebert R, Di Cesare PE (2004) Risks associated with blood transfusion after total knee arthroplasty. J Arthroplast 19(3):281–287
Sinclair KC, Clarke HD, Noble BN (2009) Blood management in total knee arthroplasty: a comparison of techniques. Orthopedics 32(1):19
Bern MM, Bierbaum BE, Katz JN, Losina E (2006) Autologous blood donation and subsequent blood use in patients undergoing total knee arthroplasty. Transfus Med 16(5):313–319. doi:10.1111/j.1365-3148.2006.00701.x
Forgie MA, Wells PS, Laupacis A, Fergusson D (1998) Preoperative autologous donation decreases allogeneic transfusion but increases exposure to all red blood cell transfusion: results of a meta-analysis. International study of perioperative transfusion (ISPOT) Investigators. Arch Intern Med 158(6):610–616
Henry DA, Carless PA, Moxey AJ, O’Connell D, Forgie MA, Wells PS, Fergusson D (2002) Pre-operative autologous donation for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev (2):CD003602. doi:10.1002/14651858.CD003602
Sculco TP, Gallina J (1999) Blood management experience: relationship between autologous blood donation and transfusion in orthopedic surgery. Orthopedics 22(1 Suppl):s129–s134
Hatzidakis AM, Mendlick RM, McKillip T, Reddy RL, Garvin KL (2000) Preoperative autologous donation for total joint arthroplasty. An analysis of risk factors for allogenic transfusion. J Bone Joint Surg Am 82(1):89–100
Keating EM, Meding JB, Faris PM, Ritter MA (1998) Predictors of transfusion risk in elective knee surgery. Clin Orthop Relat Res 357:50–59
Birkmeyer JD, Goodnough LT, AuBuchon JP, Noordsij PG, Littenberg B (1993) The cost-effectiveness of preoperative autologous blood donation for total hip and knee replacement. Transfusion 33(7):544–551
Thoms RJ, Marwin SE (2009) The role of fibrin sealants in orthopaedic surgery. J Am Acad Orthop Surg 17(12):727–736
Carless PA, Henry DA, Anthony DM (2003) Fibrin sealant use for minimising peri-operative allogeneic blood transfusion. Cochrane Database Syst Rev (2):CD004171. doi:10.1002/14651858.CD004171
Levy O, Martinowitz U, Oran A, Tauber C, Horoszowski H (1999) The use of fibrin tissue adhesive to reduce blood loss and the need for blood transfusion after total knee arthroplasty. A prospective, randomized, multicenter study. J Bone Joint Surg Am 81(11):1580–1588
Wang GJ, Hungerford DS, Savory CG, Rosenberg AG, Mont MA, Burks SG, Mayers SL, Spotnitz WD (2001) Use of fibrin sealant to reduce bloody drainage and hemoglobin loss after total knee arthroplasty: a brief note on a randomized prospective trial. J Bone Joint Surg Am 83-A(10):1503–1505
Sculco TP (1998) Global blood management in orthopaedic surgery. Clin Orthop Relat Res 357:43–49
Wang GJ, Goldthwaite CA Jr, Burks S, Crawford R, Spotnitz WD (2003) Fibrin sealant reduces perioperative blood loss in total hip replacement. J Long Term Eff Med Implants 13(5):399–411
Everts PA, Devilee RJ, Oosterbos CJ, Mahoney CB, Schattenkerk ME, Knape JT, van Zundert A (2007) Autologous platelet gel and fibrin sealant enhance the efficacy of total knee arthroplasty: improved range of motion, decreased length of stay and a reduced incidence of arthrofibrosis. Knee Surg Sports Traumatol Arthrosc: Off J ESSKA 15(7):888–894. doi:10.1007/s00167-007-0296-x
Mawatari M, Higo T, Tsutsumi Y, Shigematsu M, Hotokebuchi T (2006) Effectiveness of autologous fibrin tissue adhesive in reducing postoperative blood loss during total hip arthroplasty: a prospective randomised study of 100 cases. J Orthop Surg (Hong Kong) 14(2):117–121
Flynn JC, Metzger CR, Csencsitz TA (1982) Intraoperative autotransfusion (IAT) in spinal surgery. Spine 7(5):432–435
Carless PA, Henry DA, Moxey AJ, O’Connell D, Brown T, Fergusson DA (2010) Cell salvage for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev (4):CD001888. doi:10.1002/14651858.CD001888.pub4
Billote DB, Glisson SN, Green D, Wixson RL (2002) A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 84-A(8):1299–1304
Heyse TJ, Haas SB, Drinkwater D, Lyman S, Kim HJ, Kahn BA, Figgie MP (2013) Intraarticular fibrinogen does not reduce blood loss in TKA: a randomized clinical trial. Clin Orthop Relat Res. doi:10.1007/s11999-013-3036-1
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bou Monsef, J., Buckup, J., Waldstein, W. et al. Fibrin sealants or cell saver eliminate the need for autologous blood donation in anemic patients undergoing primary total knee arthroplasty. Arch Orthop Trauma Surg 134, 53–58 (2014). https://doi.org/10.1007/s00402-013-1876-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-013-1876-5