
Abstract
Background
Intra-articular fractures of the distal radius (DRF) are associated with a twofold increase in the risk of scapholunate ligament injury (SLI). The aim of this study was to compare functional outcome, pain, and disability between patients with operatively treated DRF and either an acute, repaired scapholunate ligament injury or no ligament injury.
Methods
We retrospectively analyzed 18 patients with an intraarticular DRF and SLI that was diagnosed and treated (Group I) and compared them with 20 patients with DRF without associated ligament injury (Group II) (20 women, 18 men; average age 55 years, range 19–72). The two cohorts were analyzed for differences in motion, grip strength, pain, Mayo wrist score, and Quick Disabilities of the Arm, Shoulder, and Hand (DASH) score an average of 43 months (range 12–73) after surgery. Radiographic assessment included fracture union, palmar tilt, radial inclination, ulnar variance, intercarpal angles, and arthrosis (according to Knirk and Jupiter). We used T-tests to compare range of motion, grip strength, pain (visual analog scale), DASH scores, and radiographic alignment between cohorts. A Chi-squared analysis was used to determine radiographic differences of arthritis.
Results
There were no significant differences in mean range of motion, grip strength, Quick DASH score, Mayo wrist score, pain level, or radiographic arthrosis between cohorts. There was no correlation between radiographic signs of osteoarthritis and the QuickDASH score, and pain level.
Conclusion
The outcomes of intraarticular fractures of the distal radius with operatively treated associated SLI are comparable with the outcomes of intraarticular fractures of the distal radius without associated SLI.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Fractures of the distal radius represent approximately one-sixth of all fractures that are treated in emergency departments [1]. The prevalence of ligamentous injury associated with fractures of the distal radius has been reported to be as high as 69 % when partial injuries are included [2]. Intraarticular fractures are associated with a twofold increase in the risk of scapholunate ligament injury (SLI), although most of these are partial and of uncertain importance [3]. Diagnosis of acute SLI is difficult, especially when associated with a fracture of the distal radius. Fracture-associated pain precludes provocative wrist ligament testing [4] and presence of a displaced intraarticular distal radius fracture, and the resulting carpal malalignment might obscure differences in intercarpal angles on plain radiographs.
The degree to which SLI may add to the impairment, symptoms, and disability after recovery from a fracture of the distal radius is debated. Tang and associates [5] compared 20 patients with radiographic signs of scapholunate dissociation (SLD) associated with a fracture of the distal radius with 228 patients with fractures and no signs of intercarpal ligament disruption. All fractures were treated with closed reduction and cast immobilization and no ligament injuries were repaired. At 1 year, all patients with SLD showed signs of chronic instability and significantly increased scapholunate dissociation. Patients with SLD had significantly worse overall function and delayed ligament reconstruction or limited intercarpal arthrodesis was performed in eight cases.
The rationale for treatment of SLI is that lack of treatment may lead to increased motion between the two bones generating shear stress, local synovitis, and pain [6]. Complete scapholunate (SL) ligament disruption may lead to severe alterations in carpal balance and subsequent carpal collapse [4, 6, 7].
Considering rapid degeneration of a torn SL ligament, early diagnosis facilitates reduction and repair and leads to improved outcomes [4].
Our practice is based on the opinion that SLI that is diagnosed and treated in the acute phase with a percutaneous or arthroscopically guided Kirschner wire fixation might lead to less pain, disability, and arthrosis [4, 8, 9].
This case–control investigation tested the null hypothesis that there is no significant difference in wrist motion, pain, and disability between patients with an operatively treated intraarticular fracture of the distal radius and either an acute, treated partial or complete SLI or no ligament injury.
Materials and methods
This was a single center retrospective case–control study.
Patients
Institutional Review Board approval was granted before initiation of this study, and strict confidentiality guidelines were followed. Inclusion criteria for case patients were operatively treated intraarticular fractures of the distal radius and operatively confirmed traumatic concomitant scapholunate ligament injury (SLI) Geissler Grade III or IV [10] who initially presented to our centre from January 2006 to December 2010. The exclusion criteria were missing or incomplete radiographs; age less than 18; time elapsed between injury and surgery over 30 days; follow-up of less than a year; pregnancy; dementia; previous injury to the ipsilateral wrist; and open fracture. We used billing records to identify appropriate patients using the International Classification of Diseases, 10th Revision, codes (S63.3, S52.50, S52.51, S52.52, S52.59). Among the 57 patients that satisfied the inclusion and exclusion criteria, 3 (5 %) declined to participate and 36 patients (63 %) could not participate due to lack of transportation, work or family responsibilities, unknown address or infirmity. The remaining 18 patients (nine women, nine men) with a mean age of 56 years (range, 41–68) formed the case group (Group I). All patients had CT arthrograms at the time of injury.
Triple-compartment arthrography was performed by an experienced, board-certified radiologist under sterile conditions, local anesthesia and fluoroscopic guidance (Axion Artis, Siemens) with iodinated contrast medium. Patient were scanned in the “superman position” (prone position, overhead extension of the arm, pronation of the wrist) with the use of a Multislice CT (Sensation Cardiac 16, Siemens; spiral scan; slice width 0.6 mm, increment 0.4 mm). High-resolution, corrected sagittal, and coronal reformatted images were obtained and stored in PACS. Images were evaluated by a board-certified radiologist and a board-certified hand surgeon (Fig. 1).

Preoperative triple compartment CT arthrography: Coronary scans show a complete tear of the scapholunate ligament (left to right dorsal to palmar) (Courtesy of Prof. Rainer Schmitt, MD, Bad Neustadt a.d. Saale, Germany)
If there had been evidence of SLI on the CT, palmar (via a palmar portal through the incision for plate fixation; nine patients) or dorsal arthroscopy (nine patients) was performed to confirm the SLI. According to the Geissler classification system [10] there were nine Grade III tears and nine Grade IV tears (Fig. 2).

Arthroscopic view of an acute Geissler Grade III scapholunate ligament tear. Upper panel a probe may be passed through the gap. Lower panel hemorrhage of the scapholunate ligament
Control patients were identified from billing records with intraarticular fractures and no SLI that satisfied all the inclusion and exclusion criteria. They were invited in consecutive chronological order until we had a sufficient number that were willing to return for evaluation within a 4 weeks’ time period so that we had the resources to do the study. A total of 51 patients were invited. Three patients declined to participate (6 %) and 28 patients (55 %) could not participate due to lack of transportation, work or family responsibilities, and unknown address or infirmity, thus resulting in a control group of 20 patients (15 women, 5 men) with a mean age of 58 years (range, 19–72) (Group II).
All patients in the control group had unremarkable radiographs with respect to SLI. Carpal stability was confirmed using fluoroscopy and PACS documentation (OEC 6800; General Electric Medical Systems, Salt Lake City, USA). All fluoroscopic examinations were performed by board-certified hand surgeons after fracture reduction and fixation. The movement of the carpal bones was recorded from extreme radial to extreme ulnar deviation in the posteroanterior view and from extreme flexion to extension in the lateral view. The procedure was repeated twice to obtain reliable images. During radioulnar deviation of the wrist, the three proximal carpal bones move synergistically from a flexed position in radial deviation to an extended position in ulnar deviation. Complete disruption of the ligamentous link results in an alteration of motion, subluxation, or “clunking” of the scaphoid [11].
The characteristics of each patient and injury including age, gender, comorbidities, mechanism of injury, AO fracture type, and type of treatment were extracted from the file and immediate post injury radiographs were analyzed.
All fractures were classified according to the AO/ASIF classification system [12] (Table 1) by a single board-certified orthopedic hand and trauma surgeon. The cause of the fracture was a fall from a standing height in 31 patients and a higher energy injury (fall from height, motor vehicle accidents or sport-related accidents) in 17 patients. We recorded associated ipsilateral fractures and dislocations, and acute carpal tunnel syndrome (CTS). Ligamentous injuries and lesions of the triangular fibrocartilage complex (TFCC) were recorded in patients that received CT arthrogram, arthroscopy, or capsulotomy (Table 1).
Surgical treatment
All fractures were treated by four experienced hand surgeons after a median of 4 days (range, 0–30) after the injury. Fractures were treated with open reduction and dorsal plating (n = 3), palmar plating (n = 25), or dorsal and palmar plating (n = 20, 18 with ancillary fixation with screws and/or Kirschner wires).
Fracture fixation and treatment of SLI were performed partly according to the degree of injury and partly the surgeons’ discretion (Table 2a, b; Fig. 3). Wrists were immobilized a median of 6 weeks (range, 4–8) in Group I and a median of 4 weeks (range, 2–6) in Group II.

Intraoperative picture of a complete scapholunate ligament tear. Left panel static widening of the SL-interval. Right panel good reduction following SL-ligament repair and transfixation
Evaluation
The patients were evaluated by an independent investigator not involved in the patients’ treatment a median of 43 months (range 12–73) after surgery. Active range of wrist motion was measured using a goniometer. Grip strength was measured with a dynamometer (Jamar; JA Preston Corp., Jackson, MI) at position 3 with the elbow at 90° and the forearm neutral and averaged over three trials. All clinical data were compared with the uninvolved side.
Wrist pain was evaluated using a numeric rating scale (NRS) between 0 (no pain) and 10 (severe pain) [13]. Upper extremity specific disability was measured with the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) questionnaire (range, 0–100, with 0 representing no symptoms or disability) [14]. The Mayo Wrist Score was calculated (range, 0–100, with 100 for the best result) [15].
Radiographic assessment
All radiographic measurements were retrospectively performed by two experienced investigators. On lateral radiographs of the symptomatic wrist in the neutral position, palmar tilt (number of degrees from the neutral position) of the articular surface of the distal radius, the scapholunate angle (SLA), the radiolunate angle (RLA), and the capitolunate angle (CLA) were measured using the tangential method and the axial method, respectively [6].
On anteroposterior (AP) radiographs the scapholunate gap (midpoint of the lateral facet of the scaphoid to the midpoint of the opposing lunate facet), radial inclination of the articular surface of the distal radius, and ulnar variance were measured as described by Medoff [16]. For better comparability, the scapholunate gap was measured in the AP view since preoperative Moneim [17] projections were missing for most patients. All measurements were made using Impax EE® software (Agfa HealthCare, Mortsel, Belgium) and the included length and angulation tools packaged in the software.
Statistical analysis
Descriptive statistics were computed for variables of interest. After testing for normality, either non-parametric Mann–Whitney Test or unpaired T test was used to test for differences in continuous variables. Fisher’s exact test was used to assess differences for categorical variables. Significance level of statistical tests was set at p ≤ 0.05.
Results
Patients
There was no significant difference between groups regarding age (p = 0.91), sex (p = 0.1), AO fracture type (p = 0.46), fracture treatment (0.37), or the intervals between injury and surgery (p = 0.24), and surgery and final evaluation (0.74).
Function, symptoms, and disability
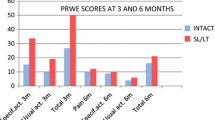
Both groups regained an average of more than 80 % of range of motion and grip strength compared with the unaffected side and there were no significant differences between groups (Table 3). There were no significant differences in pain, Mayo score, or QuickDASH between groups (Table 4).
Radiographic results
There were no significant differences between groups for palmar tilt in dorsally displaced fractures, radial inclination, ulnar variance, and radiolunate or capitolunate angle at the time of injury (Table 5a). The mean scapholunate interval at the time of injury was significantly wider in Group I (p = 0.01). A prereduction scapholunate angle of more than 60° was found in 78 % of patients in Group I and 45 % of patients in Group II. The final radiographs showed no significant differences between groups (Table 5b). There were no signs of progressive carpal malalignment or radiocarpal arthrosis in any wrist.
Complications and reoperations
Complications were noted in nine patients (24 %).
One patient in Group I developed chronic regional pain syndrome type I (CRPS I) and another patient reported transient paraesthesia of the superficial radial nerve.
One patient in Group II had a postoperative hematoma that was evacuated and another patient had a second surgery to address residual intraarticular step-off. Five patients had dorsal implants removed to address extensor tendon irritation. Six additional patients requested implant removal for discomfort without evidence of tendon irritation.
Discussion
Patients with articular fracture of the distal radius and operatively treated SLI had impairment, symptoms, and disability comparable to patients with articular fracture and no SLI. More than 80 % of patient patients in both cohorts regained more than 80 % of wrist motion and grip strength and returned to their regular employment.
Our study is similar to a randomized prospective study [18] that compared arthroscopically and fluoroscopically assisted fixation for intraarticular DRF to fluoroscopically assisted fixation alone. Complete or incomplete scapholunate ligament tears were diagnosed and treated in nine patients in the arthroscopy group. Patients who underwent arthroscopically and fluoroscopically assisted treatment had significantly better supination, extension and flexion, and a higher mean modified Mayo wrist score at all time points. The authors concluded that better treatment of associated intra-articular injuries might have been one of the reasons for the improved outcome.
Dynamic image intensifier examination and CT arthrography are part of the diagnostic algorithm for patients with intraarticular fractures of the distal radius and radiographic or clinical signs of SLI at our institution. Previous studies suggest that CT-arthrography of the wrist can detect scapholunate and lunotriquetral ligament injury and central TFCC tear with a sensitivity of up to 94 % and specificity of up to 95 % [19–21].
There are several limitations to our study. The two cohorts are heterogeneous with regard to injury severity, surgical treatment and postoperative immobilization, which might have affected outcome. However, there was no statistically significant difference between groups with respect to clinical or functional outcomes and our results are in line with those of several other studies evaluating outcome after distal radius fractures [22–25]. Given the paucity of data on SLI associated with fracture of the distal radius and the lack of untreated controls in our group, we cannot state definitively that recognizing and treating SLI improves motion, grip and, comfort, or that it limits the potential for future arthrosis. In addition, intraarticular DRF itself may lead to arthritis of the radiocarpal joint and the distal radial ulnar joint and to decreased range of wrist motion, forearm rotation, grip strength, and pain if anatomic restoration of the articular surface is not achieved [26, 27]. We do acknowledge that a mean follow-up of 43 months might not be long enough for long-term sequelae as osteoarthritis or SLAC wrist to develop. However, none of our patients showed signs of progressive carpal malalignment at the time of follow-up, and anatomic fracture reduction was maintained.
With the relatively small sample size, the generalizability of our results is limited. Our use of dynamic motion on an image intensifier to rule out SLI in the control group is not as reliable as wrist arthroscopy, although it has been reported to detect high-grade SLI with a sensitivity of up to 86 % and a specificity of up to 95.0 % [28, 29].
Scapholunate angles greater than 60° are indicative of SLI and studies comparing arthroscopic and radiographic findings reported good sensitivity and specificity [6, 29, 30]. In our cohort, the average prereduction SL angle was significantly greater in patients with SLI. However, nine patients without SLI had SL angles greater than 60°. One possible explanation is the presence of a displaced intraarticular distal radius fracture and the resulting carpal malalignment, which might obscure differences in intercarpal angles.
In our opinion, early diagnosis and treatment of high-grade SLI associated with intraarticular fractures of the distal radius is worthwhile in active patients that place high demands on their wrists to facilitate repair and prevent pain, disability, and arthrosis. Future studies should address this prospectively. Given that high-grade SLI associated with fracture of the distal radius is uncommon, multicenter trials may be necessary. Wrist arthroscopy is necessary for diagnosis in both groups, cases and controls, to diagnose complete scapholunate ligament injury and to be sure it is acute and not preexisting. An ideal study would be randomized, single blinded to the extent possible and use blinded to independent observers. Long-term studies would be necessary to determine the effect of treatment of the SLI on arthrosis.
References
Ruch DS (2006) Fractures of the distal radius and ulna. In: Bucholz RW, Heckman JD, Court-Brown C (eds) Rockwood and Green’s fractures of adults, vol 1, 6th edn. Lippincott Williams & Wilkins, Philadelphia, pp 909–988
Mehta JA, Bain GI, Heptinstall RJ (2000) Anatomical reduction of intra-articular fractures of the distal radius. An arthroscopically-assisted approach. J Bone Joint Surg Br 82:79–86
Forward DP, Lindau TR, Melsom DS (2007) Intercarpal ligament injuries associated with fractures of the distal part of the radius. J Bone Joint Surg Am 89:2334–2340. doi:10.2106/JBJS.F.01537
Kitay A, Wolfe SW (2012) Scapholunate instability: current concepts in diagnosis and management. J Hand Surg Am 37:2175–2196. doi:10.1016/j.jhsa.2012.07.035
Tang JB, Shi D, Gu YQ, Zhang QG (1996) Can cast immobilization successfully treat scapholunate dissociation associated with distal radius fractures? J Hand Surg 21A:583–590. doi:10.1016/S0363-5023(96)80007-4
Garcia-Elias M (2011) Carpal Instability. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH (eds) Green’s operative hand surgery, 6th edn. Elsevier/Churchill Livingstone, Philadelphia, pp 465–522
Pilny J, Kubes J, Hoza P, Mechl M, Visna P (2007) Scapholunate instability of the wrist following distal radius fracture. Acta Chir Orthop Traumatol Cech 74:55–58
Walsh JJ, Berger RA, Cooney WP (2002) Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 10:32–42
Darlis NA, Kaufmann RA, Giannoulis F, Sotereanos DG (2006) Arthroscopic debridement and closed pinning for chronic dynamic scapholunate instability. J Hand Surg 31A:418–424. doi:10.1016/j.jhsa.2005.12.015
Geissler WB, Freeland AE (1996) Arthroscopically assisted reduction of intraarticular distal radial fractures. Clin Orthop Relat Res 327:125–134
Short WH, Werner FW, Green JK, Masaoka S (2005) Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: part II. J Hand Surg Am 30:24–34. doi:10.1016/j.jhsa.2004.09.015
Mueller ME, Nazarian S, Koch P, Schatzker J (1990) The comprehensive classification of fractures of long bones. Springer-Verlag, New York
McCaffery M, Pasero C (1999) Pain: clinical manual, 2nd edn. Mosby, St. Louis
Beaton DE, Wright JG, Katz JN (2005) Development of the QuickDASH: comparison of three item-reduction approaches. J Bone Joint Surg Am 87:1038–1046. doi:10.2106/JBJS.D.02060
Amadio PC, Berquist TH, Smith DK, Ilstrup DM, Cooney WP 3rd, Linscheid RL (1989) Scaphoid malunion. J Hand Surg Am 14:679–687 (0363-5023(89)90191-3 pii)
Medoff RJ (2005) Essential radiographic evaluation for distal radius fractures. Hand Clin 21:279–288. doi:10.1016/j.hcl.2005.02.008
Moneim MS (1981) The tangential posteroanterior radiograph to demonstrate scapholunate dissociation. J Bone Joint Surg 63A:1324–1326
Varitimidis SE, Basdekis GK, Dailiana ZH, Hantes ME, Bargiotas K, Malizos K (2008) Treatment of intra-articular fractures of the distal radius: fluoroscopic or arthroscopic reduction? J Bone Joint Surg 90B:778–785. doi:10.1302/0301-620X.90B6.19809
Theumann N, Favarger N, Schnyder P, Meuli R (2001) Wrist ligament injuries: value of post-arthrography computed tomography. Skeletal Radiol 30:88–93
Bille B, Harley B, Cohen H (2007) A comparison of CT arthrography of the wrist to findings during wrist arthroscopy. J Hand Surg 32A:834–841. doi:10.1016/j.jhsa.2007.04.005
Schmid MR, Schertler T, Pfirrmann CW, Saupe N, Manestar M, Wildermuth S, Weishaupt D (2005) Interosseous ligament tears of the wrist: comparison of multi-detector row CT arthrography and MR imaging. Radiology 237:1008–1013. doi:10.1148/radiol.2373041450
Rozental TD, Blazar PE (2006) Functional outcome and complications after volar plating for dorsally displaced, unstable fractures of the distal radius. J Hand Surg 31A:359–365. doi:10.1016/j.jhsa.2005.10.010
Matschke S, Marent-Huber M, Audige L, Wentzensen A (2011) The surgical treatment of unstable distal radius fractures by angle stable implants: a multicenter prospective study. J Orthop Trauma 25:312–317. doi:10.1097/BOT.0b013e3181f2b09e
Jakubietz MG, Gruenert JG, Jakubietz RG (2012) Palmar and dorsal fixed-angle plates in AO C-type fractures of the distal radius: is there an advantage of palmar plates in the long term? J Orthop Surg Res 7:8. doi:10.1186/1749-799X-7-8
Richard MJ, Wartinbee DA, Riboh J, Miller M, Leversedge FJ, Ruch DS (2011) Analysis of the complications of palmar plating versus external fixation for fractures of the distal radius. J Hand Surg 36A:1614–1620. doi:10.1016/j.jhsa.2011.06.030
Lutz M, Arora R, Krappinger D, Wambacher M, Rieger M, Pechlaner S (2011) Arthritis predicting factors in distal intraarticular radius fractures. Arch Orthop Trauma Surg 131:1121–1126. doi:10.1007/s00402-010-1211-3
Prommersberger KJ, Pillukat T, Muhldorfer M, van Schoonhoven J (2012) Malunion of the distal radius. Arch Orthop Trauma Surg 132:693–702. doi:10.1007/s00402-012-1466-y
Kwon BC, Baek GH (2008) Fluoroscopic diagnosis of scapholunate interosseous ligament injuries in distal radius fractures. Clin Orthop Relat Res 466:969–976. doi:10.1007/s11999-008-0126-6
Pliefke J, Stengel D, Rademacher G, Mutze S, Ekkernkamp A, Eisenschenk A (2008) Diagnostic accuracy of plain radiographs and cineradiography in diagnosing traumatic scapholunate dissociation. Skeletal Radiol 37:139–145. doi:10.1007/s00256-007-0410-7
Megerle K, Pohlmann S, Kloeters O, Germann G, Sauerbier M (2011) The significance of conventional radiographic parameters in the diagnosis of scapholunate ligament lesions. Eur Radiol 21:176–181. doi:10.1007/s00330-010-1910-8
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Institutional Review Board
This study was performed under a protocol approved by the institutional review board (IRB) at the Rhön Klinikum AG, Klinik für Handchirurgie, Bad Neustadt Saale, Germany.
Rights and permissions
About this article
Cite this article
Gradl, G., Pillukat, T., Fuchsberger, T. et al. The functional outcome of acute scapholunate ligament repair in patients with intraarticular distal radius fractures treated by internal fixation. Arch Orthop Trauma Surg 133, 1281–1287 (2013). https://doi.org/10.1007/s00402-013-1797-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-013-1797-3