
Abstract
Background
Dysphagia is a common complication of anterior cervical spine surgery, and most of them occurred in the early postoperative period. This study aimed to determine the incidence of early dysphagia after anterior cervical spine surgery and to identify its risk factors.
Methods
A review of 186 consecutive patients undergoing anterior cervical spine surgeries in a 3-year period was performed. Dysphagia at postoperative 1 month was surveyed, and the severity of dysphagia was evaluated. Demographic information and procedural characters were collected to determine their relationships to dysphagia.
Results
A total of 50 patients developed early postoperative dysphagia, including 23 males and 27 females. The incidence of early dysphagia after anterior cervical spine surgery was 26.9 % in this study. Mild, moderate, and severe dysphagia were found in 30, 14, and 6 patients, respectively. Female, advanced age, multi-levels surgery, use of plate, and a big protrusion of plate were found to be significantly increased early dysphagia after anterior cervical spine surgery.
Conclusion
There is a relatively high incidence of early dysphagia after anterior cervical spine surgery, which may be attributable to multiple factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The anterior cervical Smith–Robinson approach is commonly used for the treatment of various cervical spine pathologies [1, 2], and the clinical outcome is generally promising. However, a series of complications related to this approach have been documented [3–5]. Dysphagia, or swallowing problem, is one of the complications that occurs frequently [5–7]. Although having been proved to be the secondly common complication of anterior cervical spine surgery [8], dysphagia is poorly investigated for its self-resolving nature. In fact, dysphagia had significantly higher self-reported disability and lower physical health status [9]. Severe and persistent dysphagia may lead to some catastrophic event such as not eating or drinking normally and, pneumonia [10–12]. Therefore, removing the hardware becomes the only option for some patients with the dysphagia [13].
Previous clinical studies showed that dysphagia easily occurred in the early postoperative period, and its symptoms were particularly serious in this phase [14–16]. In the current study, we mainly concentrated on the early dysphagia after the cervical spine surgery, which happened at first month postoperatively. We aimed to determine the incidence of early dysphagia with a retrospective data of 186 consecutive patients. Furthermore, an attempt was also made to identify the possible risk factors.
Materials and methods
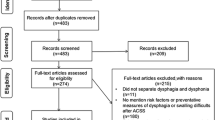
A total of 256 patients underwent anterior cervical spine surgeries between 1 January 2009 and 31 December 2011 in the study hospital. Seventy patients were excluded because of the uncomplete medical data, preoperative existing dysphagia, or losing follow-up. So 186 patients were involved in this study, including 114 males and 72 females. The average age of the study group was 51.1 years, ranging from 23 to 80 years. Patients in this study were operated by the same experienced team of surgeons in our hospital. Following a satisfactory general anesthesia, the anterior cervical spine surgery was started with a right-sided incision. Deep retractors were used to provide a nice exposure of the surgical site. Different procedures, including anterior cervical discectomy and fusion (ACDF), anterior cervical discectomy, corpectomy and fusion (ACCF), disc replacement, arthroplasty, focal cleaning, and dynamic cervical instrument (DCI) were performed as indicated on the basis of the patients’ presentation and preoperative studies. Allograft or iliac crest autograft was used per surgeon preference. Anterior plating was performed in selective patients using Slim-loc, Codman, Reflex Hybrid, Atlantis Vision, and Trinica or Stella.
Dysphagia happened during the first month after procedures were evaluated via clinical assessment, telephone surveys or letter contacts. The symptoms of dysphagia included difficulty with solid or liquid foods, pain when swallowing, food residue, and coughing when eating. Complaint due to unhealing surgical site pain was excluded. The presence of dysphagia was determined by the question “Do you have any swallowing difficulty”. If responses were symptomatic, then further information was obtained to determine its severity by the dysphagia grading system defined by Bazaz et al. [14–16]. In brief, the system defines four grades: none, mild, moderate, or severe dysphagia based on the subjective symptoms. Patients with no episodes of swallowing difficulty were graded as having “none”. Mild dysphagia was defined as rare episodes of dysphagia, which was not a significant clinical problem in these patients. Moderate dysphagia was defined as occasional swallowing difficulty with specific foods (i.e., bread or steak). Severe dysphagia was defined as frequent difficult swallowing with a majority of foods.
To find out the possible risk factors of early dysphagia after anterior cervical spine surgery, demographic information and procedural characters were collected to determine their relationships with dysphagia. The demographic information included diagnosis, gender, age, systematic comorbidity, course of disease, smoking, and alcohol use. Procedural characters included type of procedure, levels for surgery, use of plate, plate type, length of incision, duration of surgery, estimated blood loss, duration of postoperative drainage, and the protrusion length of plate (Fig. 1).

Plate protrusion: from the anterior surface of the vertebral body to that of the plate at its most cephalad aspect
All statistics analyses were performed using the Statistical Packages for Social Sciences v13.0 (SPSS, Chicago, IL). Univariate analyses were used to evaluate potential risk factors associated with postoperative dysphagia. For quantitative variables, means and standard deviations were calculated. Differences were tested using the t test for symmetrically distributed variables and the nonparametric Wilcoxon test for those that were not. For categorical variables, contingency tables were used to assess association by Fisher’s exact test. The variables with univariate P < 0.2 were considered as candidates for multiple logistic regression using Stepwise forward method [17]. A P < 0.05 was accepted as significant.
Results
A total of 50 patients developed early dysphagia, including 23 males and 27 females. The incidence of early dysphagia after anterior cervical spine surgery was 26.9 % in this study. According to the Bazaz dysphagia grading system, mild, moderate and severe dysphagia were found in 30, 14, and 6 patients, respectively. By the time of last follow-up, all dysphagia resolved themselves with or without dietary restriction except a old female case. However, this patient improved quickly after the plate was removed.
Univariate analysis showed five factors that had significant association with dysphagia after anterior cervical spine surgery (Tables 1, 2). These factors included female, advanced age, multi-levels surgery, the utilization of plate, and a big protrusion of the plate.
Multiple logistic regression using Stepwise forward method tested the eight significant factors by univariate analysis as well as those parameters with a P < 0.2. Therefore, parameters evaluated by multivariate analysis included gender, age, type of procedure, levels for surgery, use of plate, type of plate, and protrusion length of plate. Three independent significant risk factors, including females, advanced age, and a big protrusion of the plate were identified by this multivariate analysis (Table 3).
Discussion
Dysphagia is increasedly recognized as a common complication after anterior cervical spine surgery [8]. A review of the literature yields an largely varied incidence of postoperative dysphagia, ranking from 3.0 to 88.8 % [5, 18]. The following reasons may account for its wide range: firstly, the study designs. A prospective design tends to report a high incidence of postoperative dysphagia compared to that in a retrospective design [9, 19], secondly, how the dysphagia is evaluated. Edwards et al. [18] found that dysphagia was underreported by 80 % when only the surgeon records were used. Thirdly, the period at which the dysphagia is concerned. Most dysphagia happen in the first month, and as time going on, they resolve themselves [7, 9, 16]. In the current study, we mainly dealt with the early dysphagia, and we reported a incidence of 26.9 %, which is consistent with literature [9, 20].
To our knowledge, there is no universal standard for the diagnosis of dysphagia. While most studies determine the presence of dysphagia via the subjective complaints of the patients [9, 14, 15, 21]. Fluoroscopic swallow studies and electromyography had never been used to gain objective evidence of dysphagia [12, 22]. Siska et al. [23] also reported a way using the swallowing scale. Unfortunately, the objective method is not sensitive enough to discover all the existing dysphagia, It was showed that nearly one-third (7 of 19) of patients shown to have significant dysphagia on radiographic examination had no subjective dysphagia [19]. And ways using swallowing scale are complicated to be carried out. So we used a subjective way described by Bazaz et al. [14] in this study. It determined and graded a dysphagia by simply asking whether there was some difficulty in swallowing and how they influence the daily life. However, when persistent dysphagia happened or a esophageal fistula was doubted, we chose to do the barium swallow studies.
It is well-known that swallowing difficulty is related to recurrent laryngeal nerve injury, esophagus injury, local edema or hematoma, and formation of scar. But the risk factor for postoperative dysphagia have not been well-demonstrated. Being female is a risk factors of postoperative dysphagia, which has been identified in several studies [15, 24, 25]. The prevalence ratio in our study also suggested that female patients were almost five times likely to develop early postoperative dysphagia than male patients. This might be related to the overall small anatomic structure in women. Consistent with the previous study reported [9, 24], patient age was also found to have a significant effect on the occurrence of dysphagia in the current study, not surprising given that anatomic and physiologic changes associated with aging predispose elderly patients to dysphagia. Our results also supported that multi-level surgery resulted in more postoperative dysphagia than one level surgery [24, 26], although it is not significant in the multi-factors analyze. This is likely secondly to a much aggressive surgical invasion, especially the continuous retraction to the esophageal [27]. Furthermore, we found that the use of plate may be a predisposing factor, which contradict the result of previous study in which the use of instrumentation was not found to be a risk factor for dysphagia [16]. Therefore, further investigation should be performed to identify the effect of instrumentation use on dysphagia.
Anterior cervical hyperosteophytosis can lead to dysphagia alone [28, 29], bigger and thicker plate tend to cause a dysphagia [15], and even a anterior cervical hyperlordosis may aggravated a dysphagia [30]. All these imply that an excessive protrusion from the cervical vertebrae due to various reasons may be a independent risk factor of dysphagia after anterior cervical surgery. Chin et al. [21] only concerned the thickness of plate, but the distance between plate and vertebrae was neglected. So in this study, we compared the total protrusion length of plate in dysphagia group with no dysphagia group on the postoperative X-ray graphs. As a result, there was a bigger protrusion about 1.4 mm in the dysphagia group, which was significantly different. Since plates represent a mass between the pharynx or esophagus and the spine, bigger protrusion means more obstruction and oppression to the passage of foot. This result confirmed what was commonly thought which indicated that a excessive protrusion need to be avoided when the operations are being performed.
Dietary modification is recommended in patients with dysphagia to prevent material from entering the airway, and it may reduce the risk of airway obstruction or aspiration pneumonia [19]. To those with persistent dysphagia, removal of the hardware may be a wise choice in some patients.
Limitations of this study included the relatively small sample size and not providing an objective evaluation of dysphagia. And with a retrospective design, it couldn’t eliminate the influence of other confounding factors when one factor was analyzed. Moreover, the present study only concentrated whether there was a dysphagia in the first 1 month after surgery, how the dysphagia evolved since then was unknown.
In conclusion, there is a relatively high incidence for early dysphagia after anterior cervical spine surgery, which may be attributable to multiple factors. Patients should be adequately counseled about this postoperative complication. Minimization of surgical invasiveness, avoidance of continuous retraction to the esophageal, adequate removal of the osteophyte, and rational location of the hardware are suggested to decrease the occurrence of dysphagia for patients scheduled to anterior cervical surgeries, especially for those with risk factors.
References
Bailey RW, Badgley CE (1960) Stabilization of the cervical spine by anterior fusion. J Bone Joint Surg Am 42-A:565–594
Smith GW, Robinson RA (1961) The treatment of certain cervical–spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 40-A(3):607–624
Zeidman SM, Ducker TB, Raycroft J (1997) Trends and complications in cervical spine surgery: 1989–1993. J Spinal Disord 10(6):523–526
Emery SE, Bohlman HH, Bolesta MJ, Jones PK (1998) Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy. Two to seventeen-year follow-up. J Bone Joint Surg Am 80(7):941–951
Fehlings MG, Smith JS, Kopjar B, Arnold PM, Yoon ST, Vaccaro AR et al (2012) Perioperative and delayed complications associated with the surgical treatment of Cervical Spondylotic Myelopathy based on 302 patients from the AOSpine North America cervical spondylotic myelopathy Study. J Neurosurg Spine 16(5):425–432
Winslow CP, Winslow TJ, Wax MK (2001) Dysphonia and dysphagia following the anterior approach to the cervical spine. Arch Otolaryngol Head Neck Surg 127(1):51–55
Baron EM, Soliman AM, Gaughan JP, Simpson L, Young WF (2003) Dysphagia, hoarseness, and unilateral true vocal fold motion impairment following anterior cervical discectomy and fusion. Ann Otol Rhinol Laryngol 112(11):921–926
Daniels AH, Riew KD, Yoo JU, Ching A, Birchard KR, Kranenburg AJ et al (2008) Adverse events associated with anterior cervical spine surgery. J Am Acad Orthop Surg 16(12):729–738
Riley LR, Skolasky RL, Albert TJ, Vaccaro AR, Heller JG (2005) Dysphagia after anterior cervical decompression and fusion: prevalence and risk factors from a longitudinal cohort study. Spine (Phila Pa 1976) 30(22):2564–2569
Yue WM, Brodner W, Highland TR (2005) Persistent swallowing and voice problems after anterior cervical discectomy and fusion with allograft and plating: a 5- to 11-year follow-up study. Eur Spine J 14(7):677–682
Skeppholm M, Ingebro C, Engstrom T, Olerud C (2012) The dysphagia short Questionnaire: an instrument for evaluation of dysphagia: a validation study with 12 months’ follow-up after anterior cervical spine surgery. Spine (Phila Pa 1976) 37(11):996–1002
Daniels SK, Mahoney MC, Lyons GD (1998) Persistent dysphagia and dysphonia following cervical spine surgery. Ear Nose Throat J 77(6):470, 473–475
Fogel GR, McDonnell MF (2005) Surgical treatment of dysphagia after anterior cervical interbody fusion. Spine J 5(2):140–144
Bazaz R, Lee MJ, Yoo JU (2002) Incidence of dysphagia after anterior cervical spine surgery: a prospective study. Spine (Phila Pa 1976) 27(22):2453–2458
Lee MJ, Bazaz R, Furey CG, Yoo J (2005) Influence of anterior cervical plate design on Dysphagia: a 2-year prospective longitudinal follow-up study. J Spinal Disord Tech 18(5):406–409
Lee MJ, Bazaz R, Furey CG, Yoo J (2007) Risk factors for dysphagia after anterior cervical spine surgery: a 2-year prospective cohort study. Spine J 7(2):141–147
Pull TGA, Cohen DB (2009) Incidence, prevalence, and analysis of risk factors for surgical site infection following adult spinal surgery. Spine (Phila Pa 1976) 34(13):1422–1428
Edwards CN, Karpitskaya Y, Cha C, Heller JG, Lauryssen C, Yoon ST et al (2004) Accurate identification of adverse outcomes after cervical spine surgery. J Bone Joint Surg Am 86-A(2):251–256
Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA (2004) Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976) 29(13):1441–1446
Kalb S, Reis MT, Cowperthwaite MC, Fox DJ, Lefevre R, Theodore N et al (2012) Dysphagia after anterior cervical spine surgery: incidence and risk factors. World Neurosurg 77(1):183–187
Chin KR, Eiszner JR, Adams SJ (2007) Role of plate thickness as a cause of dysphagia after anterior cervical fusion. Spine (Phila Pa 1976) 32(23):2585–2590
Ryu JS, Lee JH, Kang JY, Kim MY, Shin DE, Shin DA (2011) Evaluation of dysphagia after cervical surgery using laryngeal electromyography. Dysphagia 27:318–324
Siska PA, Ponnappan RK, Hohl JB, Lee JY, Kang JD, Donaldson WR (2011) Dysphagia after anterior cervical spine surgery: a prospective study using the swallowing-quality of life questionnaire and analysis of patient comorbidities. Spine (Phila Pa 1976) 36(17):1387–1391
Kang SH, Kim DK, Seo KM, Kim KT, Kim YB (2011) Multi-level spinal fusion and postoperative prevertebral thickness increase the risk of dysphagia after anterior cervical spine surgery. J Clin Neurosci 18(10):1369–1373
Frempong-Boadu A, Houten JK, Osborn B, Opulencia J, Kells L, Guida DD et al (2002) Swallowing and speech dysfunction in patients undergoing anterior cervical discectomy and fusion: a prospective, objective preoperative and postoperative assessment. J Spinal Disord Tech 15(5):362–368
Riley LR, Vaccaro AR, Dettori JR, Hashimoto R (2010) Postoperative dysphagia in anterior cervical spine surgery. Spine (Phila Pa 1976) 35(9 Suppl):S76–S85
Mendoza-Lattes S, Clifford K, Bartelt R, Stewart J, Clark CR, Boezaart AP (2008) Dysphagia following anterior cervical arthrodesis is associated with continuous, strong retraction of the esophagus. J Bone Joint Surg Am 90(2):256–263
Lin HW, Quesnel AM, Holman AS, Curry WJ, Rho MB (2009) Hypertrophic anterior cervical osteophytes causing dysphagia and airway obstruction. Ann Otol Rhinol Laryngol 118(10):703–707
Oppenlander ME, Orringer DA, La Marca F, McGillicuddy JE, Sullivan SE, Chandler WF et al (2009) Dysphagia due to anterior cervical hyperosteophytosis. Surg Neurol 72(3):266–271
Leigh JH, Cho K, Barcenas CL, Paik NJ (2011) Dysphagia aggravated by cervical hyperlordosis. Am J Phys Med Rehabil 90(8):704–705
Acknowledgments
The authors thank Mr. Jian Zhou for his generous help in the gathering of patient data.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
J.-H. Zeng and Z.-M. Zhong contributed equally to this work.
Rights and permissions
About this article
Cite this article
Zeng, JH., Zhong, ZM. & Chen, JT. Early dysphagia complicating anterior cervical spine surgery: incidence and risk factors. Arch Orthop Trauma Surg 133, 1067–1071 (2013). https://doi.org/10.1007/s00402-013-1773-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-013-1773-y