
Abstract
Objective
To provide a basis for the choice of anterior surgery procedures in the treatment of cervical spondylotic myelopathy (CSM) through long-term follow-up.
Methods
A consecutive series of 89 patients with CSM having complete follow-up data were analyzed retrospectively. All patients were treated with anterior cervical discectomy and fusion (ACDF), and anterior cervical corpectomy and fusion (ACCF) from July 2000 to June 2007. The lesions were located in one segment (n = 25), two segments (n = 56), and three segments (n = 8). Preoperative and postoperative, the C2–C7 angle, cervical intervertebral height, radiographic fusion status, result of the adjacent segment degeneration, the Japanese Orthopaedic Association (JOA), and the Short Form 36-item (SF36) questionnaire scores were used to evaluate the efficacy of the surgery.
Results
According to the different compression conditions of the 89 cases, different anterior operation procedures were chosen and satisfactory results were achieved, indicating that direct anterior decompressions were thorough and effective. The follow-up period was 60–108 months, and the average was 79.6 months. The 5-year average symptom improvement rate, effectiveness rate, and fineness rate were 78.36 %, 100 % (89/89), and 86.52 % (77/89), respectively.
Conclusions
For CSM with compression coming from the front side, proper anterior decompression based on the specific conditions could directly eliminate the compression. Through long-term follow-up, the effect of decompression became observable.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cervical spondylotic myelopathy (CSM) is one of the most common orthopedic diseases, causing progressive degenerative changes in the cervical spine of patients over 55 years old [1, 2]. CSM can result in the symptomatic compression of the spinal cord and nerve roots, and once CSM has been diagnosed, early surgical treatment should be performed to halt further neurological deterioration, such as quadriparesis or paralysis [2]. According to the patients’ general condition, the location of the spinal cord compression, and the surgeons’ preference, surgical treatment is primarily categorized into three procedures namely, anterior operation, posterior operation, and combined approach with instrumentation [3–5]. Anterior operations such as cervical discectomy decompression, corpectomy, and autograft or titanium cage and fusion [4, 6], as well as posterior operations such as laminectomy, fusion, and laminoplasty [5, 7, 8], have been advocated to achieve adequate spinal cord decompression, maintain or restore sagittal alignment, and avoid kyphosis [3]. Generally, the anterior approach is favored when soft disc herniations of one to two levels are involved with concomitant severe axial neck pain and kyphosis, whereas the posterior approach is utilized for multilevel compression when congenital stenosis or ossification of the posterior longitudinal ligament (OPLL) is involved [9, 10]. When the compression location of the spinal cord involves three or more levels, the patient is recommended to undergo combined anterior and posterior surgery [11, 12] to further decompress the neural elements.
In this article, we examined the long-term follow-up of anterior operations namely, cervical discectomy decompression, corpectomy, and autograft or titanium cage and fusion (ACDF and ACCF), in the treatment of CSM.
Materials and methods
Patient selection
Between July 2000 and June 2007, a series of 89 consecutive patients (58 males and 31 females) who underwent anterior decompression and segmental fixation because of one-level or adjacent two-level or three-level cervical spondylosis, having complete follow-up data were involved in this study, accounting for 21.3 % of all cases (89/417) for 8 years. The number of levels operated on is shown in Table 1. The average age at operation was 51.3 ± 6.5 years (range 31–71). All patients had signs and symptoms of neural compression at the homologous segment, which was refractory to conservative treatment. The common compressive pathology of CSM was soft disc herniation, osteophyte formation, and dynamic instability, and there were no severe intervertebral space stenosis and anterior osteophytes at the right level. All patients underwent X-ray, CT scan, and MRI pre-surgery.
Surgical technique
The choice between the anterior operation anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) depended on the cord compression radiological characteristic. The one- and two-level segments with soft disc herniation were decompressed by ACDF, and the segments with ossification of the posterior longitudinal ligament (OPLL), osteophytes, and huge prolapsed intervertebral disc were decompressed by ACCF. The segments with severe intervertebral space stenosis and anterior osteophytes were also decompressed by ACCF (Table 2).
All patients under general anesthesia underwent a standard anterior approach operation regardless of whether one or more levels were to be decompressed. The standard surgical procedure includes discectomy and/or corpectomy, removal of osteophytes and the degenerated disk, opening of OPLL, harvest from the iliac crest of an adequate size graft or with a synmesh cage (Synthes AG, Bettlach, Switzerland) and its placement in the anterior trench, and the positioning of an anterior locking compression plate (LCP®) (Synthes AG, Bettlach, Switzerland). Postoperation, all patients wore a Philadelphia collar for at least 12 weeks. Blood loss and operation time were noted.
Data collection and follow-up
Clinical data, surgical records, and postoperative status of each patient were collected. The parameters collected include age, sex, segment of the cervical spine, treatment, and post-surgery symptoms as determined by interviews with patients. Post-surgery X-ray, CT scan, or MRI result was also examined. The last follow-up date was recorded as the last documented clinical follow-up or phone interview for patients. The follow-up time after surgery was 79.6 ± 20.5 months (range 60–108 months). A total of 89 patients returned for the final follow-up.
Outcomes assessment
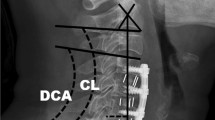
The global curvature of the cervical spine (C2–C7) was measured and analyzed after surgery. The C2–C7 angle was formed by the lines tangential to the inferior aspects of C2 and C7. The cervical intervertebral height was also measured pre- and post-surgery. The radiographic fusion status and the result of the adjacent segment degeneration were observed post-surgery. Neurological functions were evaluated according to the Japanese Orthopedic Association (JOA) scores and the Short Form 36-item (SF36) questionnaire scores. The recovery rate of the JOA score was calculated according to the following formula:
-
recovery rate = (postoperative score − preoperative score)/(17 − preoperative score) × 100 %.
Statistical analyses
The values were presented as arithmetic mean ± standard deviation. Paired t test and the Mann–Whitney U test were used for statistical analyses of C2–C7 angle, cervical intervertebral height, JOA score, and SF-36 score, which were considered statistically significant when probability values were less than 0.05 using the SPSS software (SPSS 13.0, SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
The conditions of all patients improved in this long-term follow-up study, and the symptoms disappeared or were relieved in 46 cases, disappeared overall in 31 cases, and improved without surgery-related complications in 12 cases. Postoperative physical examinations showed that all patients with preoperative muscle weakness were performed anterior surgery and gained good recovery of muscle strength with proper exercise. Postoperative limb sensory disturbances in 74 patients disappeared, and 15 patients still had some numbness. Various kinds of pathological signs gradually disappeared.
Radiographic outcomes
Significant differences were observed in the C2–C7 angle and the cervical intervertebral height between preoperative and postoperative patients after 1 year and in the final follow-up (P < 0.05). The C2–C7 angle and the intervertebral height of patients could be restored by ACDF and ACCF. In these patients, there were no significant differences between 1-year-postoperative and the final follow-up (P > 0.05) (Table 3). Re-examination of 1-year postoperative showed that all 89 patients reached a complete fusion in the CT scans, and the fusion rate was 100 %. Imaging examinations showed that adjacent segment degeneration occurred in 12 cases, which did not generate new clinical symptoms. These cases were under asymptomatic adjacent segment degeneration, and the degeneration rate was 13.48 % (12/89). No pseudarthrosis and no internal fixation loosening, detachment, and fracture occurred under postoperative X-ray examination (Figs. 1, 2).

a Postoperative MRI showing C5 and C6 disc herniation through discectomy and fusion (ACDF), no pseudarthrosis and no internal fixation loosening, detachment, and fracture occurred in one-year postoperative X-ray (b) and five-year postoperative X-ray (c)

a Postoperative MRI showing C4 to C6 disc herniation. After discectomy and C5 corpectomy and fusion (ACCF), no pseudarthrosis and no internal fixation loosening, detachment, and fracture occurred in one-year postoperative X-ray (b) and five-year postoperative X-ray (c)
JOA scores
In the ACDF group, the average JOA score was 8.2 points preoperative, 14.3 points at the 1-year follow-up, 14.2 points at the 5-year follow-up, and 14.0 points at the final follow-up. In the ACCF group, the average JOA score was 8.1 points preoperative, 14.5 points at the 1-year follow-up, 14.2 points at the 5-year follow-up, and 14.1 points at the final follow-up. No statistically significant difference between ACDF and ACCF groups was found at any of the follow-up visits (Table 4).
SF-36 questionnaire
Table 5 shows the preoperative and postoperative SF-36 scores. The scores of the four dimensions namely, physical functioning, physical role, bodily pain, and general health were significantly different between preoperative and postoperative (P < 0.05). The scores of the remaining four dimensions, namely, vitality, social functioning, emotional role, and mental health 1-year- and 5-year-postoperative were higher than those of preoperative. However, the differences in vitality and social functioning were statistically significant (P < 0.05), whereas the differences in emotional role and mental health were not statistically significant (P > 0.05).
Discussion
The anterior surgical options can be used for single-level and multi-level CSM, accounting ahead for soft disc herniations, concomitant severe axial neck pain, kyphosis, and one to three levels of involvement [9]. Anterior decompression and fusion, including discectomy, corpectomy, and fusion (i.e., ACDF and ACCF) [13–15], are recognized as a reliable and effective method in treating CSM [16]. In this study, different operations were chosen according to different compressions, indicating that direct anterior decompression operations are thorough and effective. The follow-up period was 60–108 months, with an average of 79.6 months. The 5-year average symptom improvement rate, effectiveness rate, and fineness rate were 78.36 %, 100 % (89/89), and 86.52 % (77/89), respectively.
The advantages of anterior decompression are the direct decompression and resection of the object causing pressure on the spinal cord in front, including soft disc herniations backwards, osteophytic proliferation, and ossification of the posterior longitudinal ligament. The procedure is obviously effective for CSM. Anterior fixation improves the cervical spine stability, greatly increases the fusion rate, and maintains the intervertebral height and cervical physiological curvature, reducing the complications of postoperative graft collapse and loss of physiological curvature [12, 17]. For one or two levels of CSM, the anterior approach is preferred because of its minimally invasive and direct oppression removal, which has been approved by most scholars [18, 19]. A widespread controversy exists in terms of surgical options for the three levels of CSM. According to some related studies, in cases of more than two levels, the posterior approach seems to be more suitable because of the subsequent swallowing difficulty and construct failure [12, 20, 21]. Other studies show that the anterior approach can improve the rate of osseous fusion, especially in cases of a three-disc-level fusion [9, 22]. In general, an adequate anterior decompression of the oppression in front of the spinal cord can improve the clinical outcome. When the anterior decompression is invalid, or if the cervical spondylosis with spinal stenosis or decompression range exceeds three levels, the posterior decompression or anterior and posterior combined approach is usually chosen [23]. In the current study, the anterior approach was applied in eight patients with three segments that underwent one- or two-level corpectomy and three-level cervical discectomy and fusion, with the postoperative follow-up effect being satisfactory.
Anterior decompression has obvious advantages for cervical discectomy, but a controversy exists on whether the OPLL should be removed or not [24, 25]. In this study, OPLL was resected in the anterior approach to the front of the spinal dura mater with thorough decompression. Postoperative MRI confirmed that the effect of the anterior decompression and removal of OPLL was obvious and that the pathogenetic condition of all patients improved at varying degrees. The fineness rate of JOA scores was 86.52 %, and none of the patients turned up to have a new clinical symptom during the long-term follow-up. During operation, we found that the posterior longitudinal ligament of the cervical spine thickened and became ossified because of the longer CSM disease duration. The posterior longitudinal ligament was resected to enable radical decompression. Specifically, CT scan or MRI of the segmental lesions showed a Pavlov ratio of ≤0.8 [26]. The postoperative cervical curvature and intervertebral height were recovered to a certain extent without bone grafting complications. During the postoperative follow-up process, the loss of cervical curvature and intervertebral height was not found, and the cervical curvature and intervertebral height could be long-term maintained, which ensure efficacy in the long-term follow-up.
All the 89 patients with CSM in our retrospective study had anterior oppression, which was treated with anterior decompression. For the patients with cervical herniated disc in one segment or two segments, we opted to remove the herniated disc tissue and to introduce an auto-iliac bone graft and titanium mesh with internal fixation or cage fusion in one segment to prevent intervertebral instability. Cervical corpectomy has some advantages, such as sufficient exposure and thorough decompression, when applied to patients with adjacent segment disc herniation with osteophytes on the posterior vertebral margin or spinal cord compression under thickening OPLL. For the patients with a cervical herniated disc in two segments or three segments with osteophytes on the posterior vertebral margin or spinal cord compression under thickening OPLL, removal of the intervertebral disc only could not decompress sufficiently. Thus, we opted for the one- or two-level corpectomy decompression and removal of the osteophytes on the posterior vertebral margin and thickening OPLL, along with the auto-iliac bone graft or titanium mesh with internal fixation. Moreover, the careful intraoperative hemostasis and postoperative drainage performed prevented postoperative hematoma, which has an important function in the prognosis.
Our follow-up study of more than 5 years shows that the anterior surgery is effective, which is associated with selecting the right anterior cervical decompression. For a simple cervical disc herniation or protrusion, ACDF with internal fixation and interbody fusion with cages can be performed. If the intervertebral instability is present, titanium plate fixation should be added. In patients with vertebral osteophyte formation or with OPLL, anterior one- or two-level corpectomy decompression plus auto-iliac bone graft or titanium mesh with internal fixation (ACCF) can be performed. If a clamp-like oppression from the anterior and posterior exists, the anterior approach and posterior approach should be performed successively or simultaneously. Moreover, the choice of internal fixation has an essential function in postoperative cervical stability, such as corpectomy and autograft with internal fixation and titanium mesh with internal fixation. Plate fixation can prevent graft displacement, increase the stability of the cervical spine postoperatively, and enhance bone fusion. In our study, the fusion rate reached 100 % with good stability. During the long-term follow-up, no pseudarthrosis and no internal fixation loosening, detachment, and fracture occurred postoperatively. C2–C7 angle and cervical intervertebral height were also recovered in varying degrees. Satisfying postoperative JOA and SF-36 scores were also reached.
Anterior interbody fusion can easily cause adjacent segment degeneration [27], which should be paid attention to. In a study by Ishihara et al. [28], adjacent segment degeneration was considered a natural degeneration process in more than 2 years of follow-up of 11 patients who underwent the anterior approach. In another study by Schwab et al. [29], cervical fusion reduced the number of vertebrae with active function. To maintain the scope of activities of the cervical spine, the body increases the activity of the adjacent fused vertebral segments to compensate, causing adjacent segment degeneration. In the clinical study of Xu et al. [30], both natural degeneration and biomechanical changes after fusion caused adjacent segment degeneration of 107 patients who underwent anterior approach through long-term follow-up; the latter change was the main reason for the segment degeneration. Similar results were observed in a study by Matsumoto et al. [31], in which fusion was the main reason for the adjacent segment degeneration. In our study, 12 patients appeared to have asymptomatic adjacent segment degeneration through long-term follow-up. The correlation between degeneration and interbody fusion required further observation.
At present, anterior decompression with internal fixation is still the most widely used surgical approach, and choosing the correct and effective decompression is the fundamental guarantee to achieve the intended purpose. According to the long-term follow-up results, the choice of the surgical approach in our study is reasonable. Further theoretical basis for the choice of the surgical approach is provided.
Conclusions
For CSM with compression coming from the front side, proper anterior decompression based on the specific conditions can directly eliminate the compression. It has an obvious effect of decompression through long-term follow-up.
References
Toledano M, Bartleson JD (2013) Cervical spondylotic myelopathy. Neurol Clin 31:287–305
Lebl DR, Hughes A, Cammisa FP Jr, O’Leary PF (2011) Cervical spondylotic myelopathy: pathophysiology, clinical presentation, and treatment. HSS J 7:170–178
Cabraja M, Abbushi A, Koeppen D, Kroppenstedt S, Woiciechowsky C (2010) Comparison between anterior and posterior decompression with instrumentation for cervical spondylotic myelopathy: sagittal alignment and clinical outcome. Neurosurg Focus 28:E15
Finn MA, Samuelson MM, Bishop F, Bachus KN, Brodke DS (2011) Two-level noncontiguous versus three-level anterior cervical discectomy and fusion: a biomechanical comparison. Spine (Phila Pa 1976) 36:448–453
Kim JS, Jung B, Arbatti N, Lee SH (2009) Surgical experience of unilateral laminectomy for bilateral decompression (ULBD) of ossified ligamentum flavum in the thoracic spine. Minim Invasive Neurosurg 52:74–78
Yamagata T, Takami T, Uda T, Ikeda H, Nagata T, Sakamoto S, Tsuyuguchi N, Ohata K (2012) Outcomes of contemporary use of rectangular titanium stand-alone cages in anterior cervical discectomy and fusion: cage subsidence and cervical alignment. J Clin Neurosci 19:1673–1678
Cheng SC, Yen CH, Kwok TK, Wong WC (2009) Mak KH (2009) Anterior spinal fusion versus laminoplasty for cervical spondylotic myelopathy: a retrospective review. J Orthop Surg (Hong Kong) 17:265–268
Rhee JM, Basra S (2008) Posterior surgery for cervical myelopathy: laminectomy, laminectomy with fusion, and laminoplasty. Asian Spine J 2:114–126
Yalamanchili PK, Vives MJ, Chaudhary SB (2012) Cervical spondylotic myelopathy: factors in choosing the surgical approach. Adv Orthop 2012:783762
Matz PG, Anderson PA, Groff MW, Heary RF, Holly LT, Kaiser MG, Mummaneni PV, Ryken TC, Choudhri TF, Vresilovic EJ, Resnick DK (2009) Cervical laminoplasty for the treatment of cervical degenerative myelopathy. J Neurosurg Spine 11:157–169
Guo Q, Ni B, Zhou F, Lu X, Yang J, Chen J, Yu Y, Zhu L (2011) Anterior hybrid decompression and segmental fixation for adjacent three-level cervical spondylosis. Arch Orthop Trauma Surg 131:631–636
Song KJ, Lee KB, Song JH (2012) Efficacy of multilevel anterior cervical discectomy and fusion versus corpectomy and fusion for multilevel cervical spondylotic myelopathy: a minimum 5-year follow-up study. Eur Spine J 21:1551–1557
Ba Z, Zhao W, Wu D, Shen B, Yu B, Wang Z (2012) Box cages packed with local decompression bone were efficient in anterior cervical discectomy and fusion: five- to 10-year follow-up. Spine (Phila Pa 1976) 37:E1260–E1263
Grob D, Luca A (2010) Surgery for cervical stenosis: anterior cervical decompression, corpectomy, and fusion. Eur Spine J 19:1801–1802
Dean CL, Gabriel JP, Cassinelli EH, Bolesta MJ, Bohlman HH (2009) Degenerative spondylolisthesis of the cervical spine: analysis of 58 patients treated with anterior cervical decompression and fusion. Spine J 9:439–446
Jiang SD, Jiang LS, Dai LY (2012) Anterior cervical discectomy and fusion versus anterior cervical corpectomy and fusion for multilevel cervical spondylosis: a systematic review. Arch Orthop Trauma Surg 132:155–161
Hussain M, Nassr A, Natarajan RN, An HS, Andersson GB (2011) Biomechanical effects of anterior, posterior, and combined anterior-posterior instrumentation techniques on the stability of a multilevel cervical corpectomy construct: a finite element model analysis. Spine J 11:324–330
Fallah A, Akl EA, Ebrahim S, Ibrahim GM, Mansouri A, Foote CJ, Zhang Y, Fehlings MG (2012) Anterior cervical discectomy with arthroplasty versus arthrodesis for single-level cervical spondylosis: a systematic review and meta-analysis. PLoS One 7:e43407
Pitzen TR, Chrobok J, Stulik J, Ruffing S, Drumm J, Sova L, Kucera R, Vyskocil T, Steudel WI (2009) Implant complications, fusion, loss of lordosis, and outcome after anterior cervical plating with dynamic or rigid plates: two-year results of a multi-centric, randomized, controlled study. Spine (Phila Pa 1976) 34:641–646
Cunningham, Hershman S, Bendo J (2010) Systematic review of cohort studies comparing surgical treatments for cervical spondylotic myelopathy. Spine (Phila Pa 1976) 35:537–543
Gok B, Sciubba DM, McLoughlin GS, McGirt M, Ayhan S, Wolinsky JP, Bydon A, Gokaslan ZL, Witham TF (2008) Surgical treatment of cervical spondylotic myelopathy with anterior compression: a review of 67 cases. J Neurosurg Spine 9:152–157
Liu T, Yang HL, Xu YZ, Qi RF, Guan HQ (2011) ACDF with the PCB cage-plate system versus laminoplasty for multilevel cervical spondylotic myelopathy. J Spinal Disord Tech 24:213–220
Cabraja M, Abbushi A, Koeppen D, Kroppenstedt S, Woiciechowsky C (2010) Comparison between anterior and posterior decompression with instrumentation for cervical spondylotic myelopathy: sagittal alignment and clinical outcome. Neurosurg Focus 28:1–6
Wang X, Chen Y, Chen D, Yuan W, Zhao J, Jia L, Zhao D (2009) Removal of posterior longitudinal ligament in anterior decompression for cervical spondylotic myelopathy. J Spinal Disord Tech 22:404–407
Moses V, Daniel RT, Chacko AG (2010) The value of intraoperative ultrasound in oblique corpectomy for cervical spondylotic myelopathy and ossified posterior longitudinal ligament. Br J Neurosurg 24:518–525
Bapat MR, Chaudhary K, Sharma A, Laheri V (2008) Surgical approach to cervical spondylotic myelopathy on the basis of radiological patterns of compression: prospective analysis of 129 cases. Eur Spine J 17:1651–1663
Maldonado CV, Paz RD, Martin CB (2011) Adjacent-level degeneration after cervical disc arthroplasty versus fusion. Eur Spine J 20:403–407
Ishihara H, Kanamori M, Kawaguchi Y, Nakamura H, Kimura T (2004) Adjacent segment disease after anterior cervical interbody fusion. Spine J 4:624–628
Schwab JS, Diangelo DJ, Foley KT (2006) Motion compensation associated with single-level cervical fusion: where does the lost motion go? Spine 31:2439–2448
Xu BS, Zhang ZL, Le Huec JC, Xia Q, Hu YC (2009) Long-term follow-up results and radiographic findings of anterior surgery with cloward trephination for cervical spondylotic myelopathy. J Spinal Disord Tech 22:105–113
Matsumoto M, Okada E, Ichihara D, Watanabe K, Chiba K, Toyama Y (2010) Adjacent segment disease and degeneration after anterior cervical decompression and fusion. Neurosurg Quart 20:15–22
Author information
Authors and Affiliations
Corresponding author
Additional information
The two authors Jingfeng Li and Qixin Zheng contributed equally to this work.
Rights and permissions
About this article
Cite this article
Li, J., Zheng, Q., Guo, X. et al. Anterior surgical options for the treatment of cervical spondylotic myelopathy in a long-term follow-up study. Arch Orthop Trauma Surg 133, 745–751 (2013). https://doi.org/10.1007/s00402-013-1719-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-013-1719-4