
Abstract
Purpose
The purpose of this study was to determine functional and subjective results of patients who received arthroscopic debridement for their TFCC Palmer 1B lesions and to compare their results with those of arthroscopic suture repair.
Methods
Between March 2007 and August 2011, 36 patients were diagnosed with Palmer type 1B tears and underwent arthroscopic debridement. 31 patients (15 males and 16 females) were followed up for an average of 26.7 months (±17.4 months) postoperatively. Their average age was 36.7 years (±12.7 years). Follow-up included the determination of range of motion (ROM), grip strength, pain, and wrist scores (modified Mayo wrist score (MMWS), Disabilities of the Arm, Shoulder and Hand questionnaire (DASH score)).
Results
Postoperative ROM averaged 99.2 % for the extension/flexion arc, 95.5 % for the radial/ulnar deviation arc, and 99.4 % for the pronation/supination arc of motion when compared with the contralateral wrist. The MMWS was rated excellent in 48 % of patients, good in 39 %, fair in 13 %, and poor in 0 %. The average DASH score was 17.02 (±14.92). There was a significant reduction in pain. The grip strength was 96.7 % (±15.8), pulp-to-pulp pinch 101.9 % (±17.4), and the ulnar variance −0.12 ± 1.69 mm.
Conclusions
Arthroscopic debridement of Palmer type 1B lesions in stable DRUJ yields satisfactory to excellent results. Our study showed similar results compared with the studies of arthroscopic suture repair with shorter postoperative care and fewer complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
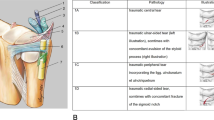
Injuries to the triangular fibrocartilage complex (TFCC) are a frequent cause of ulnar-sided pain and disability in the wrist, usually, as a result of a fall on the hyperextended wrist or a violent traction and twisting injury of the wrist [1, 2]. Palmer classified disorders of the TFCC in two basic categories: traumatic (Class 1) and degenerative (Class 2) [3]. These were subdivided into different types, depending on the location of the tear and the presence or absence of chondromalacic changes. Class 1 traumatic lesions are subdivided into four types according to the tear’s location. Type 1B injuries are peripheral tears located at the ulnar end of the TFCC [3].
The nonoperative treatment options for TFCC tears include rest, splinting, cortisone injections, and vocational changes [4]. Surgical treatment of TFCC tears includes debridement for central lesions (Palmer 1A) and open or arthroscopic suture repair [4–7], particularly for Palmer 1B tears [8–11].
However, there is still uncertainty about the best treatment option for type 1B TFCC tears.
It is known that the arthroscopic repair of TFCC Palmer 1B tears by means of suture yields satisfactory to excellent results [1, 4, 5]. Most of the treated patients experienced increased ROM, grip strength, and a significant reduction of pain [1, 4, 5]. However, suture repair is not free of complications. Nerve lesions and suture granulomas can occur and often a long postoperative care involving a long arm cast and a Bowers splint for total of 8 weeks are needed [1].
It has been also described that in cases with poor results a second surgery, such as an arthroscopic debridement, was required to improve the outcome from fair to excellent results [4].
Lubowitz and Poehling stated in their editorial [12], “Without a control group, how can we be sure that TFCC suture repair technique outcomes are preferable to other treatment options, like debridement, for example, or to no treatment at all?”
The arthroscopic debridement of TFCC lesions is a relatively straightforward, uncomplicated surgical treatment. The postoperative care is much shorter than that of suture repair and more convenient for patients as it entails minimal soft tissue trauma.
Arthroscopic debridement of a TFCC 1A tear (Central tear) has yielded good to excellent results in 80–85 % of patients who required no additional surgery [13].
Unfortunately, outcomes of arthroscopic debridement as treatment for TFCC Palmer 1B tears has to date not been thoroughly researched and described.
The purpose of this study was to determine functional and subjective results of after arthroscopic debridement in patients with TFCC Palmer 1B lesions and a stable DRUJ.
Our hypotheses were (1) that arthroscopic debridement of the TFCC 1B lesions results in satisfactory functional and subjective outcomes that are (2) comparable with those of arthroscopic suture repair.
Methods
This study design was approved by the institutional ethics committee. All patients were reviewed and evaluated by one individual who was independent and not part of the surgical team.
Patients
A retrospective analysis was performed on a cohort of patients who underwent arthroscopic debridement of TFCC Palmer 1B lesions between March 2007 and August 2011 in our clinic.
The inclusion criteria in this study were (1) a Palmer 1B tear confirmed by arthroscopy, (2) stable radioulnar joint (DRUJ), and (3) debridement as the chosen treatment. The exclusion criteria were as follows: (1) Palmer lesions other than type 1B; (2) arthroscopic suture of the TFCC; (3) instability of the DRUJ; (4) any previous wrist surgery; (5) any ligament injuries, and (6) osteoarthritis of the radiocarpal joint diagnosed by arthroscopy. Based on the results of Reiter et al. [1] a specific or restricted length of the ulna does not represent an exclusion criterion.
Thirty-six patients with Palmer 1B lesions and stable DRUJ were treated with arthroscopic debridement. Two patients were excluded due to the exclusion criteria (radius fracture, avascular necrosis of the lunate). Three patients were lost to follow-up.
A total of 31 patients could be examined (15 men, 16 women) for follow-up. Average age at the time of operation was 36.7 years (±12.7). The dominant hand was operated in 17 cases (54.8 %). The average follow-up time was 26.7 months (±17.4). Nineteen patients had a profession requiring the wrist to withstand heavy loads. Injury mechanisms that caused an ulnar-sided wrist pain included an acute event or injury in 21 cases (67.7 %). Ten patients described an insidious onset of symptoms. The average duration between accident or onset of symptoms and arthroscopy was 10.4 months (±14.4).
For more details see Table 1.
Clinical examination
Preoperatively, all patients were prescribed anti-inflammatory medication and physical therapy, and some patients wore a forearm splint for 3 weeks. In all cases, conservative treatment failed to alleviate symptoms. Every patient presented a stable DRUJ during the clinical examination before and after the arthroscopic debridement. This was demonstrated by the absence of an increased dorsal-palmar translation when compared with the contralateral side (negative “piano key” or “ballottement” test).
Radiological examination
Radiographic outcome analysis included radiographs with pronated anteroposterior and true lateral views of the wrist. The ulnar variance (UV) was measured using the method of perpendiculars with the standard zero rotation view (Fig. 1) [14]. However, one patient refused to receive the X-ray examination, so the radiological examination included only 30 patients.

Ulna length determination
Arthroscopic debridement
The operative technique was conducted under regional or general anesthesia. A pneumatic tourniquet was routinely used with a mean pressure of 300 mm Hg.
Four hand surgeons performed all arthroscopic debridements. Wrist distraction was provided by a wrist traction that maintained approximately 10 pounds of distraction throughout the procedure via finger traps placed on the index, middle, and ring fingers. A 2.7-mm arthroscope was introduced in accordance with the standard technique through the 3/4 and 6R portals. The diagnosis of the TFCC 1B lesions was confirmed using a probe (Fig. 2a). The debridement of the Palmer 1B lesions was performed using an arthroscopy shaver (Richard Wolf, Knittlingen, Germany) and grasping forceps. This was done with great care so as to not injure the dorsal and palmar radioulnar ligaments (Fig. 2b). Afterwards, the patients received an intra-articular corticosteroid injection.

a Typical Palmer 1B lesion with an inserted probe. b Arthroscopic view of the TFCC following arthroscopic debridement of the Palmer 1B lesion
Postoperative care
As postoperative care, a compressive dressing and forearm splint were applied for 10 days.
Grip strength
Grip strength was determined using the Jamar dynamometer at level two (Sammons Preston, Bollingbrook, IL). Patients were asked to grip the dynamometer three consecutive times with each hand, and an average was taken. Grip strength data are reported as a percentage of the contralateral side [15].
ROM
Postoperatively, wrist range of motion (ROM) was measured with a standard goniometer. ROM of the operated wrist was compared with ROM of the contralateral side. The ROM included wrist extension, flexion, radial and ulnar deviation, and forearm rotation. The results were reported as percentages of the contralateral wrist.
VAS pain scale
Exertional wrist pain was assessed using a visual analog scale (VAS) following the operation. Additionally, the patient was asked to recall and indicate the level of pain prior to arthroscopy. The VAS started at 0, signifying no pain, and ended with a value of 10, equalling extreme pain [1].
Mayo score
Functional outcome was determined using the modified Mayo wrist score (MMWS) [16, 17].
DASH score
Subjective results were measured using the Disabilities of the Arm, Shoulder, and Hand questionnaire (DASH) score. This is a standardized instrument which captures a patient’s own assessment of upper extremity disability and consists of 30 items, each scored on a scale of 1–5. A higher score indicates a greater number of symptoms and greater disability [18, 19].
Statistical analysis
Ordinal and nominal data are described by absolute and relative frequencies. Continuous data are expressed by average, standard deviation, minimum, and maximum. The differences were investigated using the paired t test. Relations between different variables were investigated using Pearsons correlation coefficient.
Statistical analyses were performed using SPSS (version 11.0; SPSS, Chicago, IL) and SAS for Windows (version 9.2; SAS Institute, Cary, NC). Because of the hypothesis-generating nature of our study, an adjustment for multiple testing was not done. The results of all statistical tests have to be interpreted in an exploratory sense. p < 0.05 was considered significant.
Results
Grip and pinch strength
Grip strength averaged 96.7 % (±15.8 %) of the contralateral side. Pulp-to-pulp pinch was 101.9 % (±17.4 %) of the contralateral side. No significant differences were found between the operated and healthy hand regarding pinch strength (p = 0.86).
However, a marginal significant difference (p = 0.05) was found in the grip strength between the operated (34.8 kg ± 13.9) and the contralateral (36.5 kg ± 14.1) side.
Further results are detailed in Table 2.
ROM
All patient’s ROM averaged at least 95.5 % (±10.8 %) of the contralateral side.
No significant differences were found between the operated and healthy wrist regarding ROM extension/flexion (p = 0.34) and pronation/supination (p = 0.26). However, a significant difference (p = 0.03) was found in radialinclination/ulnarinclination between the operated (49.87º ± 7.6) and the contralateral (52.26º ± 8.4) wrist. Further results are detailed in Table 3.
VAS pain scale
The preoperative VAS values averaged 7.6 mm (±1.7) and were significantly reduced to 2.3 mm ± 1.8 (p < 0.01). Further results are detailed in Table 3.
Mayo score
The MMWS averaged 90 points (±9.1), and ranged between 70 and 100. For more detail, please see Tables 2, 4.
DASH score
The DASH score averaged 17 points (±14.92), and ranged between 1 and 73 (Table 3).
Discussion
The main findings of this study were that the arthroscopic debridement of TFCC Palmer 1B tear in patients with stable DRUJ yields good to excellent results when Mayo and DASH Scores are evaluated. These results are comparable with those of arthroscopic suture studies [1, 2, 4, 6].
ROM
The extent of pronation and supination is a relevant indicator of the constitution of the TFCC and DRUJ. In this study, the pronation supination arc of motion was 99.4 % ± 3 when compared with the contralateral side. However, no significant differences were found between the operated and healthy wrist regarding the pronation—supination arc of motion (p = 0.26).
Wrist ROM was similar, and in some cases even better, than the ROM results described in the arthroscopic suture repair studies. For example, Wysocki et al. [6] found that pronation was 98 % (80º ± 6º) and supination 96 % (79º ± 6º) of the contralateral side. Reiter et al. [1] found that the pronation-supination arc of motion averaged 98 % (171º ± 19º) of the unaffected side. Haugstvedt reported an average of 97 % (range 75–108 %) [20]. Please see Table 4 for more details.
Grip and pinch strength
In this analysis the postoperative grip strength was 97 % of the contralateral hand and is higher when compared with the postoperative results of arthroscopic suture repair studies. For example, Wysocki et al. [6] found grip strength to be 95 %, Yao et al. [5] 64 %, Reiter et al. [1] 85 % ± 22, and Estrella et al. [4] 82 %. More details are shown in Table 4.
VAS Pain scale
After the arthroscopic debridement, most patients described a significant improvement of symptoms and pain. Only one patient reported no change of symptoms.
DASH score and Mayo score
The results of this study show that its DASH score [1, 5, 6, 15, 21] and Mayo Score [1, 2, 4, 20, 22, 23] averages are also similar to those of arthroscopic suture repair studies.
These satisfactory to excellent outcomes in the Mayo score show the possibility that arthroscopic debridement replaces suture repair in cases of TFCC 1B tears with a stable DRUJ. None of the patients in this study presented with a poor postoperative result.
To date, suture repair of 1B tears has been considered to be the standard treatment option [1]. However, Estrella et al. [4] reported that a “second-look” arthroscopy was necessary to investigate persistent wrist pain in eight patients following suture. Four of these patients who received arthroscopic debridement reported “Fair to excellent” outcomes. We believe that this serves as an indication that arthroscopic debridement of TFCC 1B tears with stable DRUJ may suffice as treatment.
Complications
Complications due to arthroscopic debridement did not occur in this study. This is in contrast to suture repair studies, where some complications were observed, for example, suture granulomas, paraesthesia of the ulnar nerve, and extensor carpi ulnaris tendonitis [1, 8, 9, 11].
Limitations of the study
This study’s design was retrospective. We believe that a randomized blinded study that compares results of arthroscopic debridement with suture repair should be performed.
Conclusions
Arthroscopic debridement of Palmer type 1B lesions with stable DRUJ yields satisfactory to excellent results, which are comparable to those of arthroscopic suture repair. Additionally, debridement entails a shorter postoperative care and fewer complications than suture repair. No additional operations were required to improve symptoms.
References
Reiter A, Wolf MB, Schmid U et al (2008) Arthroscopic repair of Palmer 1B triangular fibrocartilage complex tears. Arthroscopy 24:1244–1250
Corso SJ, Savoie FH, Geissler WB, Whipple TL, Jiminez W, Jenkins N (1997) Arthroscopic repair of peripheral avulsions of the triangular fibrocartilage complex of the wrist: a multicenter study. Arthroscopy 13:78–84
Palmer AK (1990) Triangular fibrocartilage disorders: injury patterns and treatment. Arthroscopy 6:125–132
Estrella EP, Hung LK, Ho PC, Tse WL (2007) Arthroscopic repair of triangular fibrocartilage complex tears. Arthroscopy 23:729–737
Yao J, Lee AT (2011) All-arthroscopic repair of Palmer 1B triangular fibrocartilage complex tears using the FasT-Fix device. J Hand Surg Am 36:836–842
Wysocki RW, Richard MJ, Crowe MM, Leversedge FJ, Ruch DS (2012) Arthroscopic treatment of peripheral triangular fibrocartilage complex tears with the deep fibers intact. J Hand Surg Am 37:509–516
Moritomo H, Masatomi T, Murase T, Miyake J, Okada K, Yoshikawa H (2010) Open repair of foveal avulsion of the triangular fibrocartilage complex and comparison by types of injury mechanism. J Hand Surg Am 35:1955–1963
Iwasaki N, Minami A (2009) Arthroscopically assisted reattachment of avulsed triangular fibrocartilage complex to the fovea of the ulnar head. J Hand Surg Am 34:1323–1326
Iwasaki N, Nishida K, Motomiya M, Funakoshi T, Minami A (2011) Arthroscopic-assisted repair of avulsed triangular fibrocartilage complex to the fovea of the ulnar head: a 2 to 4-year follow-up study. Arthroscopy 27:1371–1378
Waterman SM, Slade D, Masini BD, Owens BD (2010) Safety analysis of all-inside arthroscopic repair of peripheral triangular fibrocartilage complex. Arthroscopy 26:1474–1477
Atzei A (2009) New trends in arthroscopic management of type 1-B TFCC injuries with DRUJ instability. J Hand Surg Eur 34:582–591
Lubowitz JH, Poehling GG (2008) Keeping up with the literature: knee ligament, wrist triangular fibrocartilage tear, and suture bridge rotator cuff technique questions. Arthroscopy 24:1203–1204
Bain GI, Munt J, Turner PC (2008) New advances in wrist arthroscopy. Arthroscopy 24:355–367
Fujitani R, Omokawa S, Lida A, Santo S, Tanaka Y (2012) Reliability and clinical importance of teardrop angle measurement in intra-articular distal radius fracture. J Hand Surg Am 37:454–459
Ruch DS, Papadonikolakis A (2005) Arthroscopically assisted repair of peripheral triangular fibrocartilage complex tears: factors affecting outcome. Arthroscopy 21:1126–1130
Cooney WP, Bussey R, Dobyns JH, Linscheid RL (1987) Difficult wrist fractures. Perilunate fracture-dislocations of the wrist. Clin Orthop Relat Res 214:136–147
Cooney WP, Linscheid RL, Dobyns JH (1994) Triangular fibrocartilage tears. J Hand Surg Am 19:143–154
Chen W, Wang J, Pan J, Zhang Q, Shao X, Zhang Y (2012) Primary results of Kienböck’s disease treated using balloon kyphoplasty system. Arch Orthop Trauma Surg 132:677–683
Kraus MD, Dehner C, Riepl C, Schöll H, Gebhard F (2012) A novel method of image-based navigation in fracture surgery. Arch Orthop Trauma Surg 132:741–750
Haugstvedt JR, Husby T (1999) Results of repair of peripheral tears in the triangular fibrocartilage complex using an arthroscopic suture technique. Scand J Plast Reconstr Surg Hand Surg 33:439–447
Millants P, De Smet L, Van Ransbeeck H (2002) Outcome study of arthroscopic suturing of ulnar avulsions of the triangular fibrocartilage complex of the wrist. Chir Main 21:298–300
Shih JT, Lee HM, Tan CM (2002) Early isolated triangular fibrocartilage complex tears: management by arthroscopic repair. J Trauma 53:922–927
Tünnerhoff HG, Haussmann P (2001) What are the indications for arthroscopic repair of ulnar tears of the TFCC? Handchir Mikrochir Plast Chir 33:239–244
Conflict of interest
All authors had no financial interest, commercial associations or financial relationships at the time of submission.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cardenas-Montemayor, E., Hartl, J.F., Wolf, M.B. et al. Subjective and objective results of arthroscopic debridement of ulnar-sided TFCC (Palmer type 1B) lesions with stable distal radio-ulnar joint. Arch Orthop Trauma Surg 133, 287–293 (2013). https://doi.org/10.1007/s00402-012-1643-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-012-1643-z