
Abstract
Introduction
Aneurysmal bone cyst is a benign lesion occurring in young patients which frequently recurs after treatment. Biopsy is mandatory for the diagnosis of a putative aneurysmal bone cyst as this lesion can be secondary to another underlying process including a malignant bone tumour. The histopathological features of aneurysmal bone cysts have been examined with the goal of finding relevant criteria for predicting favourable evolution or recurrence of the disease.
Patients and methods
Twenty-one biopsies of surgically treated aneurysmal bone cysts, from 21 patients, were analysed. Histomorphometry by two different methods (3,000- and 200-point-counting) and by two observers was performed to quantify the percentage of each tissue type in the cyst (cellular, fibrillar, osteoid). A healing index was developed by calculating a ratio of osteoid and fibrillar material divided by cellular tissue. Biopsies were also examined using two immunostains, cluster of differentiation 68 (CD68) and proliferating cell nuclear antigen (PCNA).
Results
The final outcome was healing for 16 aneurysmal bone cysts (healing group) and recurrence for the five others (recurrence group), after a mean follow-up of 4.43 years. The two groups differed significantly in the proportion of their cellular content and their healing index. The ratio of CD68 negative to CD68 positive cells was also significantly different between the two groups.
Conclusion
Biopsy should be considered as a helpful prognostic factor for aneurysmal bone cyst.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Biopsies are necessary to confirm diagnosis of aneurysmal bone cysts (ABC), since ABC can be secondary to a malignant bone lesion such as a telangiectasic osteosarcoma [1]. Percutaneous or surgical biopsies are possible, but more material can be obtained with surgical biopsy. Macroscopically, ABC appear as unclotted blood in cystic cavities surrounded by a variable amount of more fleshy, solid aggregates of tissue. The latter component is microscopically formed of spindled fibroblasts, stromal mononuclear cells and giant cells (osteoclast like) with possible strands of new bone (osteoid).
The natural progression of ABC is composed of four phases: osteolysis, expansion, stabilisation and healing [2, 3]. Detection generally occurs during the expansion or stabilisation phases. Spontaneous healing may be observed either without intervention [2, 3], or after biopsy [4–6]. Such occurrence highlights the intrinsic potential of the cysts for healing.
Multiple treatments have been proposed for ABC, including superselective embolisation, radiotherapy, calcitonin injection, Ethibloc® injection, curettage and bone grafting, osteoinduction method and wide excision. Rates of local recurrence after primary treatment other than “en bloc excision” are reported to range from 12 to 59% [5, 7–9].
Prognostic factors for risk of recurrence have been reported, and are male gender, young age and juxtaphyseal location [8, 10–13]. Biopsy was also regarded as a prognostic factor by Ruiter et al. [9], with mitotic index of 7 or higher related to recurrence. This correlation was not, however, verified by Freiberg et al. [14] in children. The aim of this study was to define histological patterns characteristic of the biological behaviour of the cyst that could predict healing or recurrence.
Materials and methods
Patient’s series
Twenty-one patients with ABC were treated in our institution between May 1991 and October 2004 with the surgical procedure described previously [7] (Table 1). The age of patients and location of ABCs are summarised in Table 1. Fifteen were radiographically aggressive and six active according to Campanacci’s criteria [4]. There were 10 males and 11 females with a mean age at the time of biopsy of 16.38 years (range 8–28 years). Eleven cysts were located in long bones (four at the distal femur, two at both the proximal humerus and the distal tibia, and one at each of the following locations: proximal femur, distal fibula, diaphyseal radius). Eight others cysts were located at the pelvis (6 ilio-pubic rami and 2 iliac wings). Two lesions were found, located at the calcaneus and the scapular glenoid.
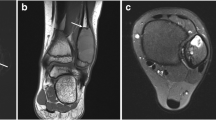
During surgery, the cyst was minimally opened to obtain a large sample of tissue for diagnosis. Biopsy was followed by implantation of an osteoinductive (demineralised bone powder supplemented with autologous bone marrow) or osteoconductive material (tricalcium phosphate cylinder). Imaging (magnetic resonance imaging) had been preoperatively analysed to choose the more appropriate location for biopsy (area of cyst activity). Twenty-one biopsies were available for histological analysis to confirm the ABC diagnosis, and were used for the present study.
Postoperative assessment
A postoperative evaluation was performed by a monthly radiograph for the first 3 months and every 6 months thereafter. The final outcome was classified as healing or recurrence according to clinical and radiographic criteria [7]. In the case of healing, the cyst enlargement ceased, and a peripheral osseous shell appeared around the ABC within the first 3 months postoperatively. The bone graft material was gradually replaced by progressive ossification of the cyst, and the lesion became non-painful. By the final evolution, the ABC was fully obliterated by homogeneous ossification (Fig. 1) or assumed a “soap bubble” appearance and remained stable [7]. In the case of recurrence, the cyst continued to demonstrate expansion, no peripheral shell appeared within 3 months, the bone graft material was progressively reabsorbed, and the lesion was still painful [7] (Fig. 2).

Aneurysmal bone cyst of the great trochanter (case 15). a Radiograph before the procedure; b 1 month after the procedure, the implanted material is visible; c at latest follow-up (5.5 years) the cyst is fully obliterated

Aneurysmal bone cyst of the fibula (case 19). a Radiograph 6 months before the surgical procedure; b radiograph at the time of the procedure; c 1 month after the procedure, the demineralized bone powder is still visible into the cyst; d after 5 months, there is a resorption of the powder and no sign of healing
Histological evaluation
All tissue fragments were fixed in 10% formalin, paraffin-embedded and cut into 2–4 blocks. 6-μm thick sections were stained with Hematoxylin-Eosin (HE). The slides were reviewed blindly and consecutively without knowledge of either the final outcome or the patient characteristics.
To view the entire biopsy area, an integrated ocular with a 100 point-grid was used, and the grid moved over successive non-overlapping areas until 3,000 different points were reached. Three components of the ABC were defined (Fig. 3), evaluated over the whole biopsy, and expressed as percentages. The cellular component (C) included stromal cells and giant cells. Giant cells were easily detected as they contain several nuclei. Stromal cells are mononuclear, with a round or oval nucleus and a scarce or absent intercellular matrix. The total percentage of cellular component (C) was obtained by adding the stromal and giant cell counts. The fibrillar component (F) was comprised of fibroblasts and collagen. Fibroblasts are elongated cells characterised by an oval nucleus and a spindle cytoplasm, embedded into a collagenous extracellular matrix. Dense collagen is occasionally present, with abundance of enlarged thick collagenous fibres. The total count of the fibrillar component (F) was obtained by adding the fibroblasts, collagenous matrix and dense collagen. The osteoid component (O) was organic bone matrix deposited by osteoblasts.

The three components of an aneurysmal bone cyst. a Cellular component with associated giant cells and stromal cells: black arrow stromal cell; white arrow giant cell. b Fibrillar component, composed of spindle fibroblast (white arrow) embedded into collagenous matrix (black arrow). c Osteoid component. Organic bone matrix with the osteoid (black arrows), surrounded by osteoblasts (HE staining, magnification 600×)
As the technique of 3,000-point counting was time-consuming and difficult to apply routinely, a more rapid technique of 200-point counting was tested by two observers and compared with the first technique. In this second method, another grid was used with 21 lines and 42 intersections. The grid was moved consecutively over the whole biopsy until 200 different significant counts, belonging to one of the three predefined categories of C, F or O, were achieved.
Assuming that osteoid and fibroblastic components would be favourable to healing, and that the cellular components would be associated with recurrence, a ratio of (O + F)/C was calculated for both methods. This ratio is the sum of the osteoid component and the fibrillar component divided by the proportion of cellular component and is referred to as the healing index.
Immunostaining
Cluster of differentiation 68 (CD68) is a glycoprotein that binds to low-density lipoprotein and is expressed only on macrophages. Proliferating cell nuclear antigen (PCNA) is an antigen that is expressed in the nucleus during the DNA synthesis phase of the cell cycle [15]. Commercially available antibodies were used to detect macrophages (anti-CD68) and proliferating cells (anti-PCNA) (Fig. 4), using the 21-line grid. Only the investigated tissue was counted for C, F or O, and was considered positive when marked or negative when unmarked. Counting proceeded until 200 significant different points were acquired.

Immunostaining with CD68. a Area of a biopsy with predominance of fibroblastic tissue and poor CD68 staining. b Biopsy showing numerous giant cells and stromal cells stained with CD68 (magnification 20×)
Statistical analysis
Two groups of ABC were compared: 16 healed and 5 recurred. The proportions of histologic tissue and the measured (O + F)/C ratios were compared between the two groups using the non-parametric Mann–Whitney test. To compare the categorical data of the two groups, a non-parametric Fisher’s exact test was performed. To study reliability between the two methods and the two observers, Cohen’s kappa statistic was used [16]. A Z test was performed on the kappa results to detect significant difference between the two observers. The hypothesis that two kappas were equal was rejected if Z was >1.96 (95% confidence level test). P values less than 0.05 were considered significant.
Results
The mean follow-up for ABC patients was 4.43 years (range 2–8.85 years) (Table 1). The biopsies confirmed that lesions corresponded to a primary aneurysmal bone cyst in all cases. Sufficient material was available from the 21 surgical biopsies for histological analysis. The available areas of tissue sections varied between 15 mm2 and 2 cm2. Final evaluation was healing for 16 ABCs and recurrence for the other five (Table 1). All cases of recurrence were obvious after 6 months of follow-up, and no recurrence occurred after 6 months.
Comparing the healing group and the recurrence group, no significant differences were found for mean age, sex ratio, mean follow-up, radiological aspect or open growth plates. The healed ABCs had a predominant or equivalent osteoid component (Fig. 5) compared to the cellular component, while the recurred ABCs had a predominant cellular component (Fig. 6). A very significant difference was found for proportion of osteoid component (P = 0.001), and percentage of cellular component (P = 0.0001) (Fig. 7). The fibrillar component percentage was not significantly determining (P = 0.091).

Two biopsy fragments of a healing ABC. a Predominant fibrillar component. b Predominant osteoid tissue relative to cellular component (HE staining, magnification 600×)

Two biopsy fragments from a recurring ABC. Stromal cells and giant cells were predominant. No osteoid component was present (HE staining, magnification a 200×; b 700×)

Mean proportion of the three histological components in the healing and recurrence groups
Healing index differences were significant with both the 3,000- and 200-point counting methods (Fig. 8). Using a healing index cut-off of ≥1.2 gave substantial or almost perfect agreement with the final evaluation as healing or recurrence [17]. Kappa values were 1 and 0.877 for 3,000-point-counting and 200-point-counting for observer 1, and 0.674 for 200-point-counting for observer 2. Kappa values for observer 1 and observer 2 were not significantly different. The positive predictive value for healing was 100, 94 and 81%, respectively. The negative predictive value for recurrence was 100%.

Mean healing index ratio of healing and recurrence groups
CD68 staining and the negative cells/positive cells ratio gave highly significant agreement with the 200-point counting (Fig. 9). Choosing a ratio of ≥4.1 as a cut-off value, agreement with final evolution was almost perfect (Kappa value = 1). The positive predictive value for healing and the negative predictive value for recurrence were 100%. No significant results were found using PCNA staining.

Mean negative/positive CD68 cell ratio of healing and recurrence groups
Inter-observer agreement was substantial (Kappa = 0.788) between observer 1 and observer 2, meaning that the method was reproducible. Inter-method agreement between 200-point counting for observer 1, 3,000-point counting, and CD68 staining was almost perfect (Kappa value = 0.877), meaning that the three methods are concordant.
Discussion
Only a few studies report on factors influencing the risk of recurrence after treatment for ABC. Biopsy is generally regarded only as a means of diagnosis. In this investigation, biopsy was evaluated as a potential prognostic factor.
The rare occurrence of spontaneous healing of ABC demonstrates the intrinsic potential for self-bone healing, by gradual ossification of the septa. This repair is initiated in the wall and septa with osteoid formation. Critical for assessing prognosis is determining the exact phase of cyst evolution, either lytic, expansion, stabilisation or healing. A cyst that has already entered the stabilisation or healing phases is more prone to healing regardless of treatment. On the contrary, if the cyst is in the lytic or expansion phase, the recurrence risk is major.
Using a 100 point-grid to obtain 3,000 different points is time-consuming. However, a pathologist could use the more rapid method of 200-point counting to define the predominant component in the biopsy and to determine an approximate (O + F)/C ratio. Staining with CD68 increased the positive predictive value as it permitted a better identification of macrophagic cells. The series in this study was small, but the results were statistically highly significant and should warrant further clinical testing.
Gibbs et al. [8] and Zehetgruber et al. [13] associated a young age, open growth plates and male gender with an increased risk of local recurrences. In our series, three of the five patients were females. Three of the five recurrences occurred with open growth plates, but this difference was not significant. The mean age was not significantly different between the two groups. In our series, the preoperative radiological aspect of ABC (aggressive or active) was not useful in predicting the final outcome after surgery, because no significant difference was found between the two groups. All recurred cases had an aggressive radiological aspect, as did 10 of the 16 healed cases. In contrast, biopsy appeared to be an efficient prognostic factor. Since biopsy is generally performed to confirm diagnosis and to exclude malignant bone lesion, it could also be easily used for prognosis. Magnetic resonance imaging was used preoperatively to locate the biopsy in an area of cyst activity avoiding areas of healing or latency. Although this series was small, high significant differences were found between the healed and recurred cases by evaluating the osteoid and cellular components. When the cellular component was predominant, the cyst was prone to recurrence after surgery. In our series, no recurred ABC had a predominant osteoid component, and all had a significant cellular component. On the contrary, if the osteoid component was predominant, the cyst was probably in the healing phase and the prognosis appears to be good.
In conclusion, the healing index, defined as the (O + F)/C ratio, is proposed as a histological prognostic factor for recurrence or healing in the treatment of ABC. In cases of good prognostic value (ratio >1.2), a minimally invasive procedure as previously described [7] could be recommended.
References
Murphey MD, wan Jaovisidha S, Temple HT, Gannon FH, Jelinek JS, Malawer MM (2003) Telangiectatic osteosarcoma: radiologic-pathologic comparison. Radiology 229:545–553. doi:10.1148/radiol.2292021130
Dabska M, Buraczewski J (1969) Aneurysmal bone cyst pathology, clinical course and radiologic appearances. Cancer 23:371–389. doi:10.1002/1097-0142(196902)23:2<371::AID-CNCR2820230213>3.0.CO;2-2
Malghem J, Maldague B, Esselinckx W, Noel H, De Nayer P, Vincent A (1989) Spontaneous healing of aneurysmal bone cysts. A report of three cases. J Bone Joint Surg Br 71:645–650
Campanacci M, Capanna R, Picci P (1986) Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res 204:25–36
Marcove RC, Sheth DS, Takemoto S, Healey JH (1995) The treatment of aneurysmal bone cyst. Clin Orthop Relat Res 311:157–163
Scott I, Connell DG, Duncan CP (1986) Regression of aneurysmal bone cyst following open biopsy. Can Assoc Radiol J 37:198–200
Docquier PL, Delloye C (2005) Treatment of aneurysmal bone cysts by introduction of demineralized bone and autogenous bone marrow. J Bone Joint Surg Am 87:2253–2258. doi:10.2106/JBJS.D.02540
Gibbs CP, Hefele MC, Peabody TD, Montag AG, Aithal V, Simon MA (1999) Aneurysmal bone cyst of the extremities. Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 81:1671–1678
Ruiter DJ, van Rijssel TG, van der Velde EA (1977) Aneurysmal bone cysts: a clinicopathological study of 105 cases. Cancer 39:2231–2239. doi:10.1002/1097-0142(197705)39:5<2231::AID-CNCR2820390541>3.0.CO;2-Q
Basarir K, Piskin A, Guclu B, Yildiz Y, Saglik Y (2007) Aneurysmal bone cyst recurrence in children: a review of 56 patients. J Pediatr Orthop 27:938–943
Dormans JP, Hanna BG, Johnston DR, Khurana JS (2004) Surgical treatment and recurrence rate of aneurysmal bone cysts in children. Clin Orthop Relat Res 421:205–211. doi:10.1097/01.blo.0000126336.46604.e1
Lin PP, Brown C, Raymond AK, Deavers MT, Yasko AW (2008) Aneurysmal bone cysts recur at juxtaphyseal locations in skeletally immature patients. Clin Orthop Relat Res 466:722–728. doi:10.1007/s11999-007-0080-8
Zehetgruber H, Bittner B, Gruber D, Krepler P, Trieb K, Kotz R, Dominkus M (2005) Prevalence of aneurysmal and solitary bone cysts in young patients. Clin Orthop Relat Res 439:136–143. doi:10.1097/01.blo.0000173256.85016.c4
Freiberg AA, Loder RT, Heidelberger KP, Hensinger RN (1994) Aneurysmal bone cysts in young children. J Pediatr Orthop 14:86–91
Sim J, Wright C (2005) The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther 85(3):257–268
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174. doi:10.2307/2529310
Conflict of interest statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Docquier, PL., Delloye, C. & Galant, C. Histology can be predictive of the clinical course of a primary aneurysmal bone cyst. Arch Orthop Trauma Surg 130, 481–487 (2010). https://doi.org/10.1007/s00402-009-0887-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-009-0887-8