
Abstract
Introduction
We reviewed the mid-term outcome of GSB-III semi-constrained total elbow arthroplasty (TEA) and compared the results of patients with rheumatoid arthritis (RA) and those suffering from post-traumatic arthritis (PTA).
Patients
Forty-five patients with 54 replaced elbows, with an average age of 69 (range 49–84) were clinically [using Mayo Clinical Performance Index (MCPI) and Liverpool Elbow Score (LES)] and radiographically assessed. The average follow-up was 54 (range 20–103) months.
Results
Based on MCPI 82% of patients had excellent or good outcome. This figure was 88% for RA and 64% for PTA group (P = 0.22). Overall MCPI was 83.7(± 19) and LES 7.5 (± 1.8). Neither the MCPI (P = 0.39) nor the LES (P = 0.95) were statistically different between the RA and PTA groups. The mid-term outcome of GSB-III TEA is satisfactory.
Conclusion
The recommendation of TEA, including in patients with PTA, is supported.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Total elbow arthroplasty (TEA) is a reliable method of managing pain and instability in patients with inflammatory arthritis involving the elbow joint. This is partially due to the fact that these patients often have multiple joint involvements and are relatively physically low-demand. On the contrary patients with, post-traumatic arthritis (PTA) of the elbow joint are relatively high-demand as their other joints are usually not involved and such patients therefore like to get back to their pre-injury level of activity. Hence it is argued that the outcome of TEA in PTA can be disappointing when compared to the rheumatoid arthritis (RA) patients.
The available prostheses are broadly classified into linked and unlinked devices. Semi constrained linked implants are widely used and favoured as their stability does not purely rely on the available bone stock and strong, healthy ligaments, both of which are deficient in RA.
The GSB-III (Gschwend–Scheier–Bähler) is a linked implant with both coronal and sagittal planes sloppiness. It was designed by the Schulthess Clinic Group in the late 70s. The bearing surface is of metal on polyethylene with a non-constrained humeral–ulnar connection. Although the medium and long-term results published by the original designers of the implant are encouraging [8] conflicting reports exist by independent reviewers [21].
We as an independent centre report the medium-term follow-up of the mark III GSB prosthesis in our cohort of patients and compare the results of RA to PTA patient. We also report the Newcastle approach to the elbow for the first time.
Materials and methods
Between 1996 and 2004, 51 patients underwent GSB III TEA in our unit. All had the operation by or under direct supervision of the senior author. Thirty-five were suffering from RA, and 16 from PTA. Inclusion criteria in the RA group were intractable pain unresponsive to non-operative management, absence of active infection, acceptable soft tissue around the dorsal aspect of the elbow, Larsen radiographic score of 3–5 [14], adequate blood supply, intact extensor mechanism and a patent humeral intra-medullary canal not obstructed by a long stem total shoulder replacement implant. The criteria for PTA group were absence of active infection, healthy soft tissue, intact extensor mechanism, radiographic evidence of osteoarthritis with intractable pain unresponsive to non-operative management. In all the patients in the PTA group the pain was interfering with work and activities of daily living. From the initial cohort, three were dead at the time of follow up (four elbows) and three patients were not available for the review (one with RA and two with PTA). This left 45 patients with 54 elbow replacements. A total of 34 were female and 11 were male, with an average age of 69 at surgery (range 49–84 years). The average time of follow up was 54 months (20–103). Table 1 shows the demographic data as divided by the diagnosis.
All patients underwent total elbow replacement using the Newcastle surgical approach to the elbow and the implants were inserted according to the manufacturer’s recommendation. Antibiotic augmented cement was used. After the operation a splint was applied with the elbow in 90° of flexion for 2 weeks until the wound was healed when the rehabilitation was commenced.
The Newcastle surgical approach to the elbow [18]: The patient is placed in the lateral decubitus position with the arm supported on a well-padded gutter. A tourniquet is applied. Intravenous antibiotics are given prior to inflation of the tourniquet and continued post-operatively for 24 h. The incision starts 10–12 cm proximal to the tip of the olecranon, skirting either on the medial or lateral part of the olecranon itself, ending at the subcutaneous border of the ulna, 8–10 cm distal to the tip of the olecranon. Fascio-cutaneous skin flaps are raised and held in position using two proximal and two distal stay sutures. The ulnar nerve needs to be identified proximally, decompressed at the level of the two heads of FCU and left in its bed. In the proximal part of the wound a transverse incision is made through the triceps aponeurosis, taking care not to cut the muscle tissue, and is directed towards the lateral aspect of the arm over the fascia of the anconeus to the subcutaneous border of the ulna. Then the proximal aponeurosis is freed from the raphe and retracted using a stay suture. Anconeus is raised from the ulna by sharp dissection, and the incision is continued along the muscle fibres of the lateral head of the triceps on the radial aspect of the raphe. The lateral head and anconeus are raised as one from the underlying bone. The raphe is cut obliquely 2 cm proximal to the olecranon and retracted distally. The long and deep heads of triceps are raised from the medial supracondylar ridge of the humerus as far as the tip of the medial epicondyle. The joint is now dislocated, and the radial head is removed using a power saw with protection of the surrounding soft tissue.
Soft tissue closure begins by dividing the stay sutures, the tension in triceps is used to tension the repaired raphe and therefore the extensor mechanism of the elbow joint itself is correctly restored. Anconeus is then repaired by suturing the muscle to its deep fascia using horizontal mattress stitches. The lateral head of triceps is stitched back to the raphe. The other two heads of triceps are sutured to the ulnar border of the raphe. The aponeurosis is laid into position and repaired starting from the fascia of anconeus. The ulnar nerve is left in its bed, left decompressed but not transposed. A wound drain is inserted, the subcutaneous layers are closed, employing the deep part of the superficial fascia which is elastic. Staples are used to close the skin.
All the patients were called back for clinical and radiographic review by an independent observer. The Mayo Clinical Performance Index (MCPI) [17] and Liverpool Elbow Score (LES) [19] were used. Functional outcome and pain were categorised using the MCPI and the two groups were compared. Ulnar nerve dysfunction was classified according to the method of LES. Triceps function was evaluated and disruption was defined as a grade II or less of the extensor mechanism strength on the MRC scale [11]. Antero-posterior and medio-lateral radiographs of the elbow joint were taken and compared to the immediate post-operative films. The adequacy of cementation on the post-operative films was assessed and any evidence of radiological loosening on the latest radiograph was recorded [21]. The case notes were reviewed and intra and post-operative complications were recorded. Revision or failure was noted. One patient who had had the humeral component revised 4 years after the initial surgery was dead at the time of the follow-up.
Statistics
Chi-square test, Fisher exact test and unpaired Student’s t test were used when appropriate. All statistical analyses were performed using NCSS/PASS 2004 (number cruncher statistical systems, Kaysville, UT, USA). The level of significance was defined as 0.05.
Results
Pain
Only one patient in the RA group complained of severe pain at follow up. Severe pain was defined as that requiring regular analgesics. Thirty-five elbows had no or mild pain in this group (88% of cases) and four had moderate (9%). In the post-traumatic group no patient had severe pain, three had moderate (21%), two mild (15%) and nine (64%) no pain at all. When the two groups were compared, no statistically significant difference was observed (P = 0.63).
ROM
Range of movement was recorded and the two groups compared. There was no statistical difference between the two groups with the exception of a greater range of pronation in patients with PTA (P = 0.04; Table 1).
Function and outcome scores
The MCPI was greater in the group with RA, but the difference was not significant (P = 0.39). The LES in the two groups were the same (Table 1). When the outcome was categorised on the basis of the MCPI, 81% of the patients had a good or an excellent outcome. This figure was 88% for the patients with RA and 64% with PTA. No statistically significant difference was observed (P = 0.22; Table 1).
Ulnar nerve dysfunction
Sensory and motor function of the ulnar nerve in each replaced elbow was assessed. No deficit was observed in the patients with RA. Of those with PTA two cases of ulnar deficit were observed, one permanent sensory and one permanent motor with no disabilities. According to the case notes, both of these patients had the same ulnar nerve dysfunction prior to surgery. Although in each case the nerve was inspected and decompressed, the function failed to improve post-operatively (Table 1). No statistically significant difference was observed between the two groups (P = 0.056).
Infection
There were no cases of deep infection or triceps tendon disruption. One fracture of the lateral condyle occurred intra-operatively and was addressed by plate fixation. This patient had RA, had both elbows replaced and at the follow up was 5 years since the index operation with excellent outcome. The fracture has gone on to clinical and radiological union.
Revision
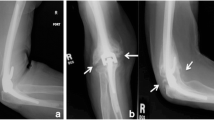
One case of bilateral disassembly was observed in the cohort, a patient with RA and bilateral elbow replacements. This patient also had a Girdlestone procedure on one of her hips. She was wheelchair bound and lived in a nursing home. Disassembly occurred on one side after five and the other after 6 years. Both sides were revised and at the time of the procedure the humeral and ulnar components were well fixed and the bearing surfaces failed to show any evidence of gross polyethylene wear. The humeral hinge mechanism was locked in extension on one side, which was unlocked, and a metal on metal extension on the ulnar peg was used in order to prevent further uncoupling. She has not experienced a further episode since. All the immediate post-operative radiographs were reviewed. One ulnar component in a patient with RA had an inadequate cementation and one in the PTA group had marginal cementation. On the humeral side, one component in each group had marginal cementation and all others were adequate (Fig. 1). A fresh set of radiograph was taken at the time of latest follow-up and was compared to the post-operative films. Only one case of gross loosening was observed. This was in a patient who subsequently underwent revision surgery. Two cases of asymptomatic “all around the prosthesis” lucency involving the humeral component were observed in the PTA group, and one in the RA group. No significant difference was seen between the two groups (P = 0.17 for the humeral and 0.55 for the ulnar components; Table 2).

Evaluation of cementation on the immediate post-operative radiographs according to the method of Schneeberger et al. [21]. No significant difference was observed (P = 0.81)
One patient in the RA group had gross loosening of the humeral component with scalloping of the cortex. As this patient was symptomatic, he underwent revision surgery 4 years after the index operation and the humeral component loosening was confirmed at the time of surgery. He subsequently died of unrelated causes. At the time of this study completed follow-up data was not available and he was therefore not included in this series of patients. No patient in the PTA group had the component revised or is awaiting such a procedure.
Discussion
The GSB-III is a linked, semi-constrained total elbow prosthesis with 4° of play in both valgus and varus directions in the coronal plane. The ulna strut of this device pistons freely in the humeral link mechanism, reducing the stresses on the interface. This free axial movement reduces the possibility of loosening due to pistoning of the ulna component as is described in the other well-known semi-linked elbow prosthesis [3]. This implant is designed to preserve more bone (GSB I philosophy), has anterior condylar flanges to prevent stress shielding of the condyles and humeral component failure (GSB-II philosophy) and has a low wear rate by employment of metal on polyethylene bearing surface (GSB-III) with sloppiness in three planes [7].
The initial GSB-III prostheses had an unacceptable high rate of disassembly [1]. This is reported as being due to extensive soft tissue release and an incorrectly placed centre of rotation of the joint. Changes implemented to the surgical technique have reduced the rate of this complication in the original designers’ series of patients. A longer ulna strut is now available should disassembly occur. Disassembly can be divided into two distinct types, early and late. The exact reproduction of the centre of rotation and appropriate soft tissue balancing are the two key factors to avoid early disassembly [9]. We did not encounter any early disassembly in our cohort. Late disassembly on the other hand is usually due to locking of the humeral hinge mechanism in extension [8]. This is reported to be an indication for humeral component revision even if it is not clinically loose [8]. We did observe this type of disassembly in one patient (bilateral GSB-III) 5 and 6 years after the operation as stated previously. At the time of surgery the whole humeral hinge mechanism on one side had become uncoupled from the axle, which was fixed back together. On the second side the hinge mechanism was indeed locked in extension due to soft tissue interposition, this was unlocked and the hinge washed out with saline. Neither of the humeral components was revised but a longer ulnar strut was used bilaterally as recommended by the developers’ published literature. At last review the patient was more than 1 year from the operations with good range of movement and fully satisfied.
The outcome of GSB-III varies in the literature. Apart from the initial higher rate of infection and disassembly in the developers’ series, the medium and long-term outcome are acceptable and comparable to lower limb joint replacements [8]. Reviews from independent centres varies from good results comparable to Gschwend et al. series [2, 12, 13] to conflicting reports with high rate of loosening [5, 21]. Our results as an independent centre are in favour of the Schulthess Clinic Group. At the latest follow-up with an average of 5 years, 82% of the patients in the studied cohort had and excellent or good outcome according to the MCPI. The fact that during the follow-up period only one of the elbows needed revision is very encouraging, specifically when compared to the recent reported survival analysis of the well-known Coonrad–Morrey prosthesis [22].
One of the main issues with total elbow replacement is patient selection. Historically this procedure was advocated for patients with predominantly inflammatory arthritis and more specifically for those with RA. Multiple joint involvement, low levels of mobility and physically low-demand lifestyles were thought to favour longevity of the implant. However this is not always the case, as multiple joint involvement, in particular lower limb joints, can make the patient dependant on walking aids. In such patients part of the body weight is shared by the upper limbs and results in higher loads across a replaced elbow. In our cohort we encountered only one patient with late disassembly of the prosthesis. This patient with RA and bilateral elbow replacements was wheelchair bound and was living in a nursing home. Unfortunately she disassembled both of the elbows 5 and 6 years after the primary procedure (each side once). The fact that both of her upper limbs were used by the staff in order to take her in and out of the wheelchair may have contributed to this complication.
On the other hand, patients with PTA were reported to have a higher rate of complications and a higher revision rate [6, 9, 20]. In this group physically lower demand patients and specifically those over 60 years of age were defined as “ideal candidates” [16]. However a recent Meta-analysis of the English literature failed to show a significant difference in the outcome of patients with RA and PTA [15].
In our cohort, patients with PTA had a statistically significant greater amount of pronation. This is probably due to lack of distal radio-ulnar joint involvement, as we invariably removed the radial head with the Newcastle surgical approach to the elbow. This aside, no other significant difference was observed between the two groups. Patients with RA scored higher on the MCPI, but this was not statistically significant. Ulnar nerve dysfunction was mainly observed in the PTA group. Both of the patients (one with permanent sensory and one with permanent motor) had the same symptoms prior to the operation, perhaps as a consequence of the initial trauma. At the time of replacement surgery the nerves were decompressed, inspected and left in their bed. Apart from perineural scarring nil else was observed. Unfortunately no recovery was encountered post-operatively. In general, higher rates of ulnar nerve dysfunction in patients with PTA can be due to the initial trauma or subsequently failed surgical management.
Literature suggests a 14% rate of radiographic lucency. In our cohort we observed an overall rate of 11% with gross loosening rate of 2% (the case with failed humeral component and subsequent revision surgery). No significant difference was observed between the two groups. Amongst the six joints with various stages of lucency only one (gross lucency) was symptomatic. This highlights the fact that the majority of radiographic lucencies are asymptomatic and reconfirms the importance of regular clinical and radiographic surveillance as suggested by the Schulthess Clinic Group [9]. The initial cementation is an important determinant for prevention of lucency and loosening. First generation cementation can be a reason for higher rate of loosening and failure [21] and advanced cementation technique has been shown to increase the load to failure of the humeral component [4].
Appropriate soft tissue balancing as achieved by the preservation of the collateral ligaments decreases the extreme of laxity observed with more radical approaches. Although the GSB-III is a linked prosthesis, abnormally high level of stress theoretically increases the wear rate. This can be reduced by meticulous surgical technique [10]. Our cohort shows a satisfactory mid-term survivorship of this implant. This is perhaps due to a combination of soft tissue balancing, reproduction of the centre of rotation of the joint and employment of advanced cementation techniques. We did not observe any evidence of clinical loosening in the patients with PTA. This is in contrary to the higher rates reported previously.
The Newcastle surgical approach to the elbow is a posterior muscle preserving surgical approach which gives an excellent exposure to the joint. We invariably identify and decompress the ulnar nerve, but transpose it only if it is unstable in its bed at the end of the procedure when the range of movement is checked. The triceps raphe is cut obliquely 2 cm proximal to the tip of the olecranon and repaired afterward by a Kessler stitch. No case of triceps disruption was observed with a mean of 5 years follow up. As this approach gives an excellent exposure and there is no risk of disruption of the triceps extensor mechanism, based on our data we recommend its use for TEA.
Overall based on the presented data the mid-term outcome of GSB-III TEA is satisfactory. There was no significant difference between the patients with RA and PTA. The use of this prosthesis in either group is supported with good functional and radiological results.
References
Bell S, Gschwend N, Steiger U (1986) Arthroplasty of the elbow. Experience with the Mark III GSB prosthesis. Aust N Z J Surg 56:823–827
Cesar M, Roussanne Y, Bonnel F et al (2007) GSB III total elbow replacement in rheumatoid arthritis. J Bone Joint Surg Br 89:330–334
Cheung EV, O’Driscoll SW (2007) Total elbow prosthesis loosening caused by ulnar component pistoning. J Bone Joint Surg Am 89:1269–1274
Faber KJ, Cordy ME, Milne AD et al (1997) Advanced cement technique improves fixation in elbow arthroplasty. Clin Orthop Relat Res 334:150–156
Fink B, Krey D, Schmielau G et al (2002) Results of elbow endoprostheses in patients with rheumatoid arthritis in correlation with previous operations. J Shoulder Elbow Surg 11:360–367
Gschwend N (2002) Present state-of-the-art in elbow arthroplasty. Acta Orthop Belg 68:100–117
Gschwend N, Loehr J, Ivosevic-Radovanovic D et al (1988) Semiconstrained elbow prostheses with special reference to the GSB III prosthesis. Clin Orthop Relat Res 232:104–111
Gschwend N, Scheier NH, Baehler AR (1999) Long-term results of the GSB III elbow arthroplasty. J Bone Joint Surg Br 81:1005–1012
Gschwend N, Simmen BR, Matejovsky Z (1996) Late complications in elbow arthroplasty. J Shoulder Elbow Surg 5:86–96
Herren DB, O’Driscoll SW, An KN (2001) Role of collateral ligaments in the GSB-linked total elbow prosthesis. J Shoulder Elbow Surg 10:260–264
Hildebrand KA, Patterson SD, Regan WD et al (2000) Functional outcome of semiconstrained total elbow arthroplasty. J Bone Joint Surg Am 82:1379–1386
Jensen CH, Jacobsen S, Ratchke M et al (2006) The GSB III elbow prosthesis in rheumatoid arthritis: a 2- to 9-year follow-up. Acta Orthop 77:143–148
Kelly EW, Coghlan J, Bell S (2004) Five- to thirteen-year follow-up of the GSB III total elbow arthroplasty. J Shoulder Elbow Surg 13:434–440
Larsen A, Dale K, Eel M (1977) Radiographic evaluation of rheumatoid arthritis and related conditions by standard reference films. Acta Radiol Diagn (Stockh) 18:481–491
Little CP, Graham AJ, Carr AJ (2005) Total elbow arthroplasty: a systematic review of the literature in the English language until the end of 2003. J Bone Joint Surg Br 87:437–444
Morrey BF, Adams RA, Bryan RS (1991) Total replacement for post-traumatic arthritis of the elbow. J Bone Joint Surg Br 73:607–612
Morrey BF, Adams RA (1992) Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. J Bone Joint Surg Am 74:479–490
Pooley J, Singh R (2000) Elbow arthroplasty. Biomet Merck Limited, Swindon
Sathyamoorthy P, Kemp GJ, Rawal A et al (2004) Development and validation of an elbow score. Rheumatology (Oxford) 43:1434–1440
Schneeberger AG, Adams R, Morrey BF (1997) Semiconstrained total elbow replacement for the treatment of post-traumatic osteoarthrosis. J Bone Joint Surg Am 79:1211–1222
Schneeberger AG, Hertel R, Gerber C (2000) Total elbow replacement with the GSB III prosthesis. J Shoulder Elbow Surg 9:135–139
Shi LL, Zurakowski D, Jones DG et al (2007) Semiconstrained primary and revision total elbow arthroplasty with use of the Coonrad-Morrey prosthesis. J Bone Joint Surg Am 89:1467–1475
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Amirfeyz, R., Blewitt, N. Mid-term outcome of GSB-III total elbow arthroplasty in patients with rheumatoid arthritis and patients with post-traumatic arthritis. Arch Orthop Trauma Surg 129, 1505–1510 (2009). https://doi.org/10.1007/s00402-009-0876-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-009-0876-y