
Abstract
Introduction
This experimental study was performed to assess, whether or not, vitamin C, required during the collagen synthesis, would influence the Achilles tendon healing in a healthy rat model.
Materials and methods
The right Achilles tendons of 42 healthy female Wistar Albino rats were completely ruptured. The rats were randomly divided into the vitamin C and control groups and both groups included third, tenth and twenty-first day subgroups. One hundred and fifty milligrams (1.5 cc) of vitamin C and 1.5 cc % 0.9 NaCl were injected once for every 2 days for the vitamin C and control groups, respectively. Qualitative and quantitative microscopic comparisons of the repair tissues of both groups were made on the mentioned days.
Results
Angiogenesis was more evident on the third day in the vitamin C group. There was a significant difference between the control and vitamin C groups regarding the type I collagen production on the tenth day. The structure of the repair tissue was almost in the form of regular dense connective tissue at the end of twenty-first day in the vitamin C group. Mean collagen fiber diameter was considerably higher, and the number of active fibroblasts in the repair tissue was slightly elevated in the vitamin C group during the entire healing process.
Conclusion
High-dose vitamin C supplementation once for every 2 days has stimulating effects on the Achilles tendon healing because of early angiogenesis and increased collagen synthesis in a healthy rat model. Further studies are needed to make clear the mentioned encouraging effects of the vitamin C on the Achilles tendon healing.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tendons are composed of parallel bundles of collagen fibers (primarily type I) and rows of fibroblasts situated between these bundles. The most important function of the type I collagen, the main functional component of tendons, is to provide resistance to force, tension and stretch [11]. The Achilles tendon, formed by the merging of the tendons of the gastrocnemius and soleus, is the thickest and strongest tendon in the human body. Achilles tendon rupture is still a challenging problem, and the peak annual incidence of Achilles tendon rupture has been reported as 18 per 100,000 in the Scandinavian population [9].
The course of the tendon healing depends on several factors such as age, nutrition, systemic diseases, hormones, infections and vitamins. The results of some previous experimental studies have shown that the Achilles tendon healing can be improved by using several methods such as local injection of growth factors [2, 17], mesenchymal stem cells [5] or platelet concentrate [3] at the repair site, local application of extracorporeal shock wave therapy [10] or systemic use of some anti-inflammatory drugs [6]. The ascorbic acid requirement for proline and lysine hydroxylase activity during the collagen synthesis is well known, and the importance of this vitamin for matrix proteoglycan synthesis has previously been reported [1, 12]. However, an experimental or clinical study analyzing the relationship between the vitamin C use and the Achilles tendon repair process has not been performed yet. The authors initially hypothesized that vitamin C therapy could influence the Achilles tendon healing due to its essential function in the collagen synthesis and decided to assess whether or not high-dose supplementation of vitamin C would lead microscopic alterations in the Achilles tendon healing in a healthy animal model.
Materials and methods
Animals and tendon rupture pattern
In this study, principles of laboratory animal care and specific national laws were strictly followed. This study was initially approved by the local institutional board of ethics. Forty-two, 3-month-old, female, nonpregnant Wistar albino rats with a mean weight of 194 ± 19 g (153–209 g) were randomly divided into two groups as “vitamin C” and “control.” Then, both groups were randomly divided into three groups as “third day,” “tenth day” and “twenty-first day” (seven rats for each subgroup). Vitamin C and control groups were similar with respect to their mean weights. The rats were kept under standardized conditions with free access to rat food and water.
Under intramuscular ketamine (200 mg/kg) plus xylazine (1 mg/kg) anesthesia, complete rupture of the right Achilles tendon was performed by creating multiple percutaneous holes by full-thickness insertion of an 18-G needle through the Achilles tendon just 1 cm proximal to its insertion into the calcaneus and then applying forceful manual dorsiflexion of the ankle joint until the sensation of complete rupture of the tendon was felt. Immobilization was not used following the rupture, and the rats were allowed to move freely in their cages. Hundred and fifty milligrams of vitamin C (1.5 cc) for the “vitamin C group” and 1.5 cc % 0.9 NaCl for the “control” group were applied intraperitoneally just after the rupture and then once for every 2 days until the sacrification procedure. Ascorbic acid dose of 150 mg/day was previously considered a high dose in an experimental study made on 4-month-old guinea pigs [13]. According to the initially determined experimental protocol, 14 rats (seven study and seven control) were killed under intraperitoneal high-dose pentobarbital anesthesia on the third, tenth and twenty-first days. None of the rats died before the scheduled killing procedure.
Histological procedure
Tissue samples, obtained from the control and vitamin C groups, were fixed for 72 h in 10% neutral formalin solution and then were applied the routine histological procedure. Three serial histological sections (4–5 μm thickness) from each rat were obtained and were stained with Masson trichrome to examine the microscopic structure of the repair tissue. Besides this, immunohistochemical examination was performed by staining the sections with mouse monoclonal type I collagen antibody (Oncogene Research Products, San Diego, CA, USA) to detect the type I collagen production [16].
Morphometric evaluation of the repair tissue between the ruptured tendon endings was performed at a magnification of 40× (Eclipse E 400; Nikon, Kawasaki, Kanagawa, Japan). Five randomly selected microscopic areas from each histological section (15 images per rat) were evaluated using an image analyzer software (Image-Pro®Plus; Media Cybernetics, Inc., Silver Spring, MD, USA) by the first two authors (SÖ, TP) concomitantly, to avoid any bias. The mentioned authors did not know the group and subgroup of any specimens, which they were investigating.
The entire repair process was evaluated using several morphometric parameters including structure of the entire repair tissue, revascularization, type I collagen production, type I collagen fiber diameter, number of whole fibroblasts and active fibroblasts.
Grading scale for the morphometric and immunohistochemical analysis
The structure of the repair tissue was initially graded as “no connective tissue,” “loose connective tissue,” “irregular dense connective tissue” or “regular dense connective tissue.” Revascularization in the repair tissue was initially graded as “absent,” “few,” “moderate” or “significant.” In the central zone of the repair tissue, diameters of randomly selected 20 consecutive collagen fibers were measured in micrometers, and number of whole fibroblasts and number of active fibroblasts were recorded in each sample. Active fibroblast was initially defined as the fibroblast having an abundant and irregularly branched cytoplasm with an ovoid, large and pale-staining nucleus, fine chromatin and a prominent nucleolus [8]. Type I collagen production in the repair tissue was initially graded as “absent,” “few,” “moderate” or “significant.” Intraobserver or interobserver validity of the grading scale was not assessed.
Statistical analysis
The t test for independent samples was used to compare the collagen fiber diameter means, and the chi-square test and the Fisher’s exact test were used to compare the entire repair tissue structure, revascularization, type I collagen production, total fibroblast and active fibroblast ratios. A P value less than 0.05 was considered significant.
Results
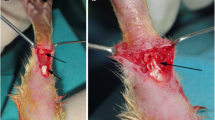
Third day (Tables 1 and 2, Fig. 1a, b)
The mean collagen fiber diameter (P < 0.001), revascularization (P = 0.01) and the total number of fibroblasts (P = 0.042) were significantly higher in the repair tissue of the vitamin C group when compared with those of the control group (Tables 1 and 2, Fig. 1). The number of active fibroblasts was also somewhat higher in the vitamin C group (P = 0.091). The other investigated parameters were found to be similar in both groups.

Third day control group; fibroblasts (fb) and collagen fibers (co) are seen in the repair tissue; Masson trichrome, ×40. b Third day vitamin C group; when compared with the third day control group, collagen fiber diameter (co) and number of total and active fibroblasts (fb) are higher and revascularization process (rv) is more evident in the repair tissue; Masson trichrome, ×40
Tenth day (Tables 1 and 2, Fig. 2a, b)
The mean collagen fiber diameter (P < 0.001) was significantly higher, and type I collagen production (P = 0.021) in the repair tissue was significantly more noticeable in the vitamin C group (Fig. 2). No significant difference between the groups was seen regarding the other investigated parameters.

a Tenth day control group; weak type I collagen production is seen; anti-type-I collagen, ×40. b Tenth day vitamin C group; when compared with the tenth day control group, type I collagen production (⇒) is very prominent; anti-type-I collagen, ×40
Twenty-first day (Tables 1 and 2, Fig. 3a, b)
The mean collagen fiber diameter (P < 0.001) was significantly higher in vitamin C group (Fig. 3). No significant difference between the groups was seen regarding the other investigated parameters. It was observed that the repair tissue was almost in the form of regular dense connective tissue in the vitamin C group.

a Twenty-first day control group; the structure of the entire repair tissue is in the form of irregular dense connective tissue; fibroblasts (fb) and collagen fibers (co) are seen in the repair tissue; Masson trichrome, ×40. b Twenty-first day vitamin C group; the healing process is almost complete and the structure of the repair tissue is in the form of regular dense connective tissue; Masson trichrome, ×40
Discussion
Like the other mesenchymal tissue repair processes, the tendon repair process has been an attractive topic for the scientists for many years. The authors could not be able to encounter with an in vivo or clinical study analyzing the effects of vitamin C on the Achilles tendon healing, which is still a challenging problem. As vitamin C plays an important role in collagen synthesis, its possible helpful effects on the Achilles healing cannot be underestimated. Moreover, it was previously stated that optimal flexor tendon maintenance by the vitamin C was dose-dependent in vitro [12]. Based on this observation, the authors chose a high-dose vitamin C supplementation protocol for better understanding the effects of vitamin C on the Achilles tendon repair process.
Outcome measures of previous studies, focused on the tendon healing process following different treatment protocols, are dissimilar [4]. We chose structure of the entire repair tissue, revascularization, type I collagen production, type I collagen fiber diameter, number of whole fibroblasts and active fibroblasts as outcome measures for this experiment, because we believed these were the main issues for the exact microscopic assessment of the tendon repair tissue. However, we recognized there were several limitations to our current study. In the present study, single vitamin C application protocol was performed, but this dose may be considered very high, and besides this, the effects of different dose protocols on the Achilles tendon healing might have been compared. Besides histopathological examination, biomechanical examination might have been performed. Moreover, besides the evaluation of the short-term effects of the vitamin C supplementation, the long-term effects might have been assessed. The management method of the Achilles tendon rupture (conservative rather than primary surgical repair or avoiding immobilization during conservative treatment) may also be considered one of the shortcomings of the present study, as this may affect the healing process. The relevance of this model to the human condition may be considered dubious, as postrupture regimen is hardly applicable to the human situation and vitamin C is usually administered orally in human medicine.
Fibroblasts initially produce procollagen, and after secretion of the procollagen from the fibroblast, the final collagen fibers are formed following several extracellular events. Vitamin C is needed in the hydroxylation of two amino acids (proline and lysine), forming the triple helix of collagen. In case of vitamin C deficiency, the final structure of the collagen molecule cannot be formed due to lack of hydrogen bonds [1, 11]. Besides the hydroxylation effect, in vitro positive effects of vitamin C on type I and III collagen synthesis, by enhancing the human fibroblasts’ gene transcription and elevating their mRNA levels, have been shown [14]. In the present study, the active fibroblasts, the markers of the intracellular production (procollagen synthesis), were slightly more intensified in the repair tissue during the entire healing process in the vitamin C group. Moreover, type I collagen expression, determined by the immunohistochemical examination and an objective parameter of the type I collagen concentration in the repair tissue, was more evident on the tenth day in the vitamin C group.
The diameter of the collagen fiber differs in size, but in dense regular connective tissue of a tendon that is subject to considerable stress, such as the Achilles tendon, it necessarily increases [11]. The diameter of the collagen fibers in the Achilles tendon was previously found decreased (36%) with respect to control group in healthy human Achilles tendon ruptures [7]. These observations can emphasize the close relationship between the mass of the collagen fibers and the occurrence of the Achilles tendon rupture. The findings of the present study revealed that the diameter of collagen fibers were considerably higher in the vitamin C group than that in the control group, which would lead to improvement in the strength of the repair tissue during the entire repair process.
It is well known that increased blood supply enhances the repair process in all kind of mesenchymal tissues. The beneficial effects of ascorbic acid on angiogenesis by enhancing the collagen type IV synthesis by human endothelial cells was previously stated [15]. In the present study, angiogenesis process was more evident in the vitamin C group than was in the control group at the early stage of the healing process.
In the present study, the structure of the repair tissue in the vitamin C group was nearly one grade away from the one in the control group on third, tenth and twenty-first days. At the end of twenty-first day, the structure of the repair tissue in the vitamin C group was almost in the form of regular dense tissue that is the main structure of a tendon. On the other hand, the structure of the repair tissue in the control group was mostly in the form of irregular dense tissue that is the main structure of the late repair tissue in tendon healing. These findings may also be considered the indicators of the accelerative effect of the vitamin C on the Achilles tendon healing process.
The main advantages of the vitamin C use are that, it is cheaper and has no major adverse effects except its dose- and time-dependent in vitro and in vivo mutagenic effects [13]. However, there are only experimental studies, indicating the effectiveness of vitamin C on the tissue repair procedure, but not any controlled clinical studies. Based on the encouraging results of the present experimental study, it cannot be possible to recommend the routine use of the vitamin C in the daily clinical practice. Further prospective, randomized, double-blinded clinical studies with long-term follow-up are needed to clarify the stimulating effect of the vitamin C on the Achilles tendon healing in humans.
In conclusion, parenteral supplementation of high-dose vitamin C once for every 2 days accelerates the Achilles tendon healing in a healthy rat model. The microscopic qualitative and quantitative improvement in the repair process, caused by the vitamin C use, appears to depend on the enhancement of angiogenesis at the early stage and of type I collagen synthesis during the entire repair process.
References
Alcantra-Martos T, Delgado-Martinez AD, Vega MV, Carrascal MT, Munuera-Martinez L (2007) Effect of vitamin C on fracture healing in elderly osteogenic disorder shionogoi rats. J Bone Joint Surg Br 89:402–407
Aspenberg P, Forslund C (1999) Enhanced tendon healing with GDF 5 and 6. Acta Orthop Scand 70:51–54
Aspenberg P, Virchenko O (2004) Platelet concentrate injection improves Achilles tendon repair in rats. Acta Orthop Scand 75:93–99
Bruns J, Kampen J, Kahrs J, Plitz W (2000) Achilles tendon rupture: experimental results on spontaneous repair in a sheep-model. Knee Surg Sports Traumatol Arthrosc 8:364–369
Chong AK, Ang AD, Goh JC, Hui JH, Lim AY, Lee EH, Lim BH (2007) Bone marrow-derived mesenchymal stem cells influence early tendon-healing in a rabbit achilles tendon model. J Bone Joint Surg Am 89:74–81
Forslund C, Bylander B, Aspenberg P (2003) Indomethacin and celecoxib improve tendon healing in rats. Acta Orthop Scand 74:465–469
Jarvinen TAH, Jarvinen TLN, Kannus P, Jozsa L, Jarvinen M (2004) Collagen fibres of the spontaneously ruptured human tendons display decrease thickness and crimp angle. J Orthop Res 22:1303–1309
Junqueira LC, Carneiro J (2003) Basic histology: text and atlas, 10th edn. Lange Medical Books/McGraw-Hill, New York
Leppilahti J, Puranen J, Orava S (1996) Incidence of Achilles tendon rupture. Acta Orthop Scand 67:277–279
Orhan Z, Ozturan K, Guven A, Cam K (2004) The effect of extracorporeal shock waves on a rat model of injury to tendo Achillis. A histological and biomechanical study. J Bone Joint Surg Br 86:613–618
Ross MH, Kaye GI, Pawlina W. Histology (2003) A text and atlas with cell and molecular biology, 4th edn. Lippincott Williams & Wilkins, Philadelphia
Russell JE, Manske PR (1991) Ascorbic acid requirement for optimal flexor tendon repair in vitro. J Orthop Res 9:714–719
Shamberger RJ (1984) Genetic toxicology of ascorbic acid. Mutat Res 133:135–159
Tajima S, Pinnell SR (1996) Ascorbic acid preferentially enhances type I and III collagen gene transcription in human skin fibroblasts. J Dermatol Sci 11:250–253
Telang S, Clem AL, Eaton JW, Chesney J (2007) Depletion of ascorbic acid restricts angiogenesis and retards tumor growth in a mouse model. Neoplasia 9:47–56
Van der Loos CM, Marijianowski MH, Becker AE (1994) Quantification in immunohistochemistry: The measurement of the ratios of collagen types I and II. Histochem J 26:347–354
Zhang F, Liu H, Stile F, Lei MP, Pang Y, Oswald TM, Beck J, Dorsett-Martin W, Lineaweaver WC (2003) Effect of vascular endothelial growth factor on rat Achilles tendon healing. Plast Reconstr Surg 112:1613–1619
Acknowledgments
The authors thank Mustafa Karaköse, MD, for his kind help during the experimental procedure in rats.
Author information
Authors and Affiliations
Corresponding author
Additional information
Gazi University Scientific Research Project Foundation provided the financial support for this study (project no. 01/2003-01).
Rights and permissions
About this article
Cite this article
Ömeroğlu, S., Peker, T., Türközkan, N. et al. High-dose vitamin C supplementation accelerates the Achilles tendon healing in healthy rats. Arch Orthop Trauma Surg 129, 281–286 (2009). https://doi.org/10.1007/s00402-008-0603-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-008-0603-0