
Abstract
Introduction: Osteonecrosis of the femoral head is a local destructive disease with progression into devastating stages. Left untreated it mostly leads to severe secondary osteoarthrosis and early endoprosthetic joint replacement. Core decompression by exact drilling into the ischemic areas can be performed in early stages according to Ficat or ARCO. Computer-aided surgery might enhance the precision of the drilling and lower the radiation exposure time of both staff and patients. The aim of this study was to evaluate the precision of the fluoroscopically based VectorVision® navigation system in an in vitro model. Materials and methods: Thirty sawbones were prepared with a defect filled up with a radiopaque gypsum sphere mimicking the osteonecrosis. Twenty sawbones were drilled by guidance of an intraoperative navigation system VectorVision® (BrainLAB, Munich, Germany) and 10 sawbones by fluoroscopic control only. Results: No gypsum sphere was missed. There was a statistically significant difference regarding the three-dimensional deviation (Euclidian norm) as well as maximum deviation in x-, y- or z-direction (maximum norm) to the desired mid-point of the lesion, with a mean of 0.51 and 0.4 mm in the navigated group and 1.1 and 0.88 mm in the control group, respectively. Furthermore, significant difference was found in the number of drilling corrections as well as the radiation time needed: no second drilling or correction of drilling direction was necessary in the navigated group compared to 1.4 in the control group. The radiation time needed was less than 1 s compared to 3.1 s, respectively. Conclusion: The fluoroscopy-based VectorVision® navigation system shows a high feasibility of computer-guided drilling with a clear reduction of radiation exposure time and can therefore be integrated into clinical routine. The additional time needed is acceptable regarding the simultaneous reduction of radiation time.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteonecrosis, also known as avascular necrosis or aseptic necrosis, is a serious disease mainly affecting patients between 30 and 50 years of age, particularly with progression into devastating stages. Pathogenesis is still unknown, but all discussed factors like corticosteroids, embolism or intravascular coagulation lead to ischemic death of the bony and marrow tissues, subchondral fractures and a progressive secondary osteoarthropathy after collapse of the articular surface. Osteonecrosis of the femoral head is the predominant localization of osteonecrosis in the adult population [17, 22]. Following Ficat and ARCO (Association Research Circulation Osseous), the disease progresses through stages which can be divided by size, location and diagnostic criteria [4, 7].
Like the pathogenesis, there is still controversy regarding the treatment of this condition. The effectiveness of conservative treatment remains uncertain, and surgical treatment demanded the extent of surgery depending on the stage of the disease [12, 13, 23, 26]. In early stages, many authors suggest core decompression by exact drilling into the ischemic areas [1, 22, 23]. This is said to improve symptoms by releasing pain through relieving of intraosseous pressure by the accompanying edema and furthermore by the improvement of the remodeling of the ischemic parts by breaking open the sclerotic bone and enabling blood circulation and revascularization. It can be done with or without additional pushing in of bony grafts [23, 25]. Later stages and already started osteoarthropathy usually have to be provided by arthroplasty [1, 23].
In core decompression, the precision of the drilling is essential for the outcome. The lesion on the one hand has to be decompressed effectively; on the other hand damage of the femoral cartilage should be strictly avoided within the procedure. Therefore, experience and spatial imagination of the surgeon is crucial, as well as the visualization itself. The latter mostly is performed by using an image intensifier, which is part of the standardized operation room. Most of those intensifiers visualize just one plane. This can cause a series of intraoperative X-rays and increased X-ray exposure not only of the patient, but also of the operation room team and furthermore puts sterility at risk.
Regarding this, new methods like the computer-aided navigation have been introduced to reduce this X-ray exposition and improve the precision of drilling. Computer-aided orthopedic surgery (CAOS) meanwhile is well established in different fields. CT-based, fluoroscopically assisted or imageless methods are used to simultaneously generate different planes of the therapeutic object to be treated [24].
Despite an increasing usage of computer-assisted surgery, only few studies regarding the accuracy have been described like drilling the pedicles of the spine, the talus or even the proximal femur, all dealing with different methods and navigation systems [2, 3, 14–16, 19].
The aim of this study was to evaluate the precision of core decompression with the VectorVision® navigation system (BrainLAB, Munich, Germany), in an in vitro model of osteonecrosis of the femoral head. Furthermore, the exposure time of radiation was measured to evaluate possible reduction of exposure time of both staff and patients. The overall time of the procedure was measured to evaluate possible lengthening by additional steps required by the navigation system.
Materials and methods
The navigation system used in this study (VectorVision® spine 5.5, BrainLAB) enables fluoroscopy-based intraoperative navigation. It is based on an optical tracking unit, which detects the reflecting marker spheres by an infrared camera (Fig. 1). Controlling of the system is done by a draped touch-screen monitor.

Overall view of the assembly: left side the positioned sawbone, fluoroscope, infrared camera and touch-screen monitor of the navigation system; right side the positioned sawbone with attached reference markers and the marker-device on the image intensifier
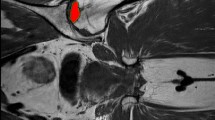
Thirty sawbones (Sawbones Europe, Malmö, Sweden) were used to carry out these experiments. Each sawbone was prepared by drilling the femoral head with a conical shaped drill, central implantation of a radiopaque gypsum sphere measuring 5 mm in diameter and closure of the remaining defect by bony cement. Twenty sawbones were drilled by guidance of an intraoperative navigation system VectorVision® (BrainLAB); 10 sawbones served as control and were drilled in a conventional drilling technique.
The sawbones were positioned in a special device in a manner mimicking a supine position of a patient lying on an operating table (Fig. 1). The procedure itself is based on the virtual connection of the fluoroscopic images and the position of the surgical instruments. For this purpose it is necessary to attach markers to the surgical instruments, the patient and the X-ray intensifier. Therefore, a reference array with passive reflecting marker spheres was rigidly attached to the lateral surface of each sawbone by a Schanz screw. Visualization of the femoral head with the gypsum spheres was carried out creating images in anteroposterior and axial position by a C-arm fluoroscope, which is connected to the navigation system. The C-arm itself is equipped with a device with reflecting markers to define the orientation of the C-arm in spatial orientation for the navigation system. After the two fluoroscopic images the image intensifier is moved out of the operation field and no further intraoperative images are needed.
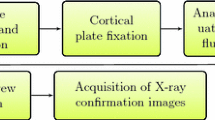
A standard drill is equipped with a marker-clamp and measured with a special calibration tool in order to inform the navigation system about the length, diameter and position of the tip of the instrument (Fig. 2). Next, the surgical instrument is visualized on the touch-screen monitor. By online control of the navigation system the drill is placed in the desired position (Fig. 3). Virtual connection of the position of all the reference markers enables the orientation of the drilling guide in the two fluoroscopic planes simultaneously.

Calibration of the drill attached with reference markers by a special calibration tool

Real-time visualization of drilling on the associated touch-screen
After computer-assisted drilling of the femoral head, the positioning of the drill was controlled by two perpendicular fluoroscopic images of the proximal femur cut with the drill left in situ to measure the distance between the mid-point of the target and the tip of the drill. The greatest distance from the target was taken for further statistical evaluation. Three-dimensional deviation was measured by calculating the three-dimensional diagonal line, the entry point of the drilling being the origin of the three-dimensional system of coordinates, with the x-axis in line with the drill starting at the entry point and ending in the target center and perpendicular y- and z-axes (L=√x 2+y 2+z 2). The time needed for the procedure was measured starting with the positioning of the bones and ending with removal of the bone. X-ray exposure time could directly be read on the image intensifier after creating the images, taking 1 s into calculation if less than 1 s was needed.
As mentioned above, serving as a control group, 10 identically prepared sawbones were drilled in a conventional technique just by the control of drilling direction of the same C-arm fluoroscope and image intensifier in two planes.
Statistical analysis
Statistical analysis was carried out using the t test for the procedure time needed and the Mann–Whitney rank sum test for the three-dimensional diagonal line and the greatest distance from the target, the radiation time needed and the number of drilling corrections needed, each comparing navigated to the control group. A P < 0.05 was considered to be of statistical significance.
Results
The distances of the tip of the drill to the desired mid-point of the lesion are shown in Tables 1, 2, 3 and 4, as well as the number of drilling corrections needed and the time needed for procedure and radiation exposure. The mean length of the three-dimensional diagonal line was 0.51 for the navigated group compared to 1.1 in the control group (Tables 1 and 2). Taking the greatest distance for each drilling (Tables 2 and 3), the mean precision of the drilling was 0.4 mm for the navigated group and 0.88 mm for the non-navigated control group. The mean procedure time was 5.05 min for the navigated group and 4.14 min for the non-navigated control group. The mean radiation exposure time was less than 1 s for the navigated group and 3.1 s for the non-navigated control group. No gypsum sphere was missed and, regarding the greatest distance to the desired mid-point of the gypsum sphere, just one was missed by more than 1 mm in the navigated group compared to three in the control group. No second drilling or correction of drilling direction was necessary in the navigated group compared to a mean of 1.4 drilling corrections (range from 0 to 3) in the control group (Tables 1 and 2).
Taking the greatest distances of the drillings into calculation, the precision in reaching the desired mid-point of the target in the navigated group and the control group is shown in Table 5, the distances from the target thereby being grouped into zones.
Discussion
Arlet and Ficat described the technique of core decompression in 1964 [7]. Up to now, this procedure is still widely accepted and performed, although a disparity exists between the various reports on outcome; success rates range from 33 to 92% with an overall success rate between 60 and 70% [1, 5, 6, 10–12, 21, 23, 26]. It is meanwhile generally accepted that core decompression should be solely performed in early stages of the disease and further dependent on the size of the necrotic lesion [1, 12, 23, 26].
Accuracy in achieving the desired point and course is essential. Fractures after drilling, which are likely to occur more often after multiple drilling corrections, as well as injuries of the cartilage by penetrating and failure by missing the lesion have been described [1, 3, 23]. Furthermore, in conventional technique exact location of the drill or wire by multiple checks of drilling course and depths causes enormous X-ray exposition of both patient and operation room staff. These side effects associated with drilling corrections particularly gain importance in obese patients and their surrounding tissues which make spatial orientation considerably difficult. Concerning these facts, it is desirable to minimize the side effects of the surgery as well as imaging time and radiation dosage.
Computer-assisted orthopedic surgery meanwhile is well accepted in several surgical fields, as it could improve precision and also minimize X-ray exposition [15, 16, 24]. Different methods like the CT-based, fluoroscopically assisted or imageless methods are used to simultaneously generate different planes of the therapeutic object to be treated [24]. As a fluoroscope is a standard piece of the equipment of an operation room and surgeons are well adapted to its visual informational content, fluoroscopic navigation was developed [9, 14, 20]. This method does not require registration like the CT-based system and reduces both imaging time and radiation dosage. Visualization of the necrotic lesions can be a possible drawback in the usage of the fluoroscopically guided navigation as the necrotic lesions can be made visible first with MRI, then CT and only later fluoroscopically. Thus, to treat the lesions in earliest stages, a CT-guided or, even better, MRI-guided system should be used which usually is not available in most institutions.
Regarding the precision of navigated drilling, which is either therapeutic itself or the first crucial step in orthopedic procedures paving the way for later osteotomies or milling, only few studies exist despite emerging and spreading systems and use [3, 8, 15, 16]. The authors reported clinically acceptable results in precision with an average distance from the given target of 2–4 mm [2, 3, 15, 16]. Those distances are consistent with CT-based navigated drillings with further application of special individual fixing methods [18]. Despite those reports, keeping in mind the spreading use of different systems one should further regard that in these studies methods differ and different navigation systems are used which cannot directly be compared and generalized. Furthermore, the bending of a wire or the tip of a thin drill could falsify the measured distances from the target, as just their length and their indirect orientation by positioning of the drilling guide are detected.
This study was performed to evaluate the precision of core decompression with the VectorVision® navigation system in an in vitro model of osteonecrosis of the femoral head. Drilling could be performed by visualization of the aiming of the target on the navigation system-associated screen. Analogous to former described publications, first we could find a high reproducibility in hitting the target with remarkable precision; we could even state a higher precision or lesser average distance from the target. The three-dimensional distance in the navigated group was less than half of the distance reached in the control group. Regarding the greatest distance to the desired mid-point of the gypsum sphere, just one was missed by more than 1 mm in the navigated group compared to three in the control group. Furthermore, although no gypsum sphere was missed in both groups, there was a clear tendency for higher precision in the navigated group with 14 out of 20 drills in a zone of less than 0.5 mm distance from the mid-point compared to 2 out of 10 in the control group. No second drilling or correction of drilling direction was necessary in the navigated group which seems to be the most important finding here, as multiple drilling corrections could weaken the bone as mentioned above. In contrast, a mean of 1.4 drilling corrections (range from 0 to 3) were needed in the control group which is even low due to the lacking surrounding tissue in our in vitro experiment. Secondly and maybe most noteworthy, we could state a clear reduction of exposure time to radiation compared to conventional techniques, in which the drilling and every possible correction must be controlled in at least two different X-ray planes. Less than 1 s was needed to acquire the initial radiographs in two planes for calculating the geometry construct in the navigated group which was significantly less than the mean time needed in the conventional drilling group. Third, the additional time needed with navigation due to both placement of reference tool, frames and diodes as well as calibration of the drill is acceptable or even negligible, particularly when compared to the additional time needed due to possible correction of drilling direction and its controlling by X-ray in two planes with the conventional drilling method. All these described findings are particularly important under in vivo conditions with regard to the surrounding tissues especially in obese patients, where spatial orientation is harder, mostly making drilling corrections necessary.
Of course, our findings present in vitro conditions and therefore cannot be directly extrapolated to the in vivo circumstances, but certainly show the clear trend towards the above-mentioned advantages like improvement of precision with simultaneous reduction of radiation exposure time. Clinical trials have to be awaited for final statements.
Conclusion
The analysis of precision of the VectorVision® navigation system shows the feasibility of hand-guided drilling by navigation with high accuracy with clear reduction of radiation exposure time and therefore will be integrated into clinical routine. The mean distance of the aimed target of 0.4 mm is remarkably low and meets realistic demands on orthopedic surgery. The additional time needed is acceptable regarding the simultaneous reduction of radiation time compared to conventional techniques.
References
Aigner N, Schneider W, Eberl V, Knahr K (2002) Core decompression in early stages of femoral head osteonecrosis—an MRI-controlled study. Int Orthop 26:31–35
Arand M, Hartwig E, Hebold D, Kinzl L, Gebhard F (2001) [Precision analysis of navigation-assisted implanted thoracic and lumbar pedicled screws. A prospective clinical study]. Unfallchirurg 104:1076–1081
Arand M, Schempf M, Kinzl L, Fleiter T, Pless D, Gebhard F (2001) [Precision in standardized Iso-C-Arm based navigated boring of the proximal femur]. Unfallchirurg 104:1150–1156
ARCO (Association Research Circulation Osseous)-Committee on Terminology and Staging (1993) Bone circulation and vascularization in normal and pathological conditions. In: Schoutens A, Arlet J, Gardeniers J et al (eds) The ARCO perspective for reaching one uniform staging system of osteonecrosis. ARCO, New York, pp 375–380
Camp JF, Colwell CW Jr (1986) Core decompression of the femoral head for osteonecrosis. J Bone Joint Surg Am 68:1313–1319
Fairbank AC, Bhatia D, Jinnah RH, Hungerford DS (1995) Long-term results of core decompression for ischaemic necrosis of the femoral head. J Bone Joint Surg Br 77:42–49
Ficat RP (1985) Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment. J Bone Joint Surg Br 67:3–9
Gautier E, Bachler R, Heini PF, Nolte LP (2001) Accuracy of computer-guided screw fixation of the sacroiliac joint. Clin Orthop Relat Res Dec:310–317
Hofstetter R, Slomczykowski M, Sati M, Nolte LP (1999) Fluoroscopy as an imaging means for computer-assisted surgical navigation. Comput Aided Surg 4:65–76
Kristensen KD, Pedersen NW, Kiaer T, Starklint H (1991) Core decompression in femoral head osteonecrosis. 18 Stage I hips followed up for 1–5 years. Acta Orthop Scand 62:113–114
Meyers MH (1988) Osteonecrosis of the femoral head. Pathogenesis and long-term results of treatment. Clin Orthop Relat Res Jun:51–61
Mont MA, Carbone JJ, Fairbank AC (1996) Core decompression versus nonoperative management for osteonecrosis of the hip. Clin Orthop Relat Res Mar:169–178
Mont MA, Fairbank AC, Krackow KA, Hungerford DS (1996) Corrective osteotomy for osteonecrosis of the femoral head. J Bone Joint Surg Am 78:1032–1038
Nolte LP, Slomczykowski MA, Berlemann U, Strauss MJ, Hofstetter R, Schlenzka D, Laine T, Lund T (2000) A new approach to computer-aided spine surgery: fluoroscopy-based surgical navigation. Eur Spine J 9(Suppl 1):S78–S88
Ohnsorge JA, Portheine F, Mahnken AH, Prescher A, Wirtz DC, Siebert CH (2003) [Computer-assisted retrograde drilling of osteochondritic lesions of the talus with the help of fluoroscopic navigation]. Z Orthop Ihre Grenzgeb 141:452–458
Ohnsorge JA, Schkommodau E, Wirtz DC, Wildberger JE, Prescher A, Siebert CH (2003) [Accuracy of fluoroscopically navigated drilling procedures at the hip]. Z Orthop Ihre Grenzgeb 141:112–119
Ohzono K, Saito M, Takaoka K, Ono K, Saito S, Nishina T, Kadowaki T (1991) Natural history of nontraumatic avascular necrosis of the femoral head. J Bone Joint Surg Br 73:68–72
Rosenberger RE, Bale RJ, Fink C, Rieger M, Reichkendler M, Hackl W, Benedetto KP, Kunzel KH, Hoser C (2002) [Computer-assisted drilling of the lower extremity. Technique and indications]. Unfallchirurg 105:353–358
Schwarzenbach O, Berlemann U, Jost B, Visarius H, Arm E, Langlotz F, Nolte LP, Ozdoba C (1997) Accuracy of computer-assisted pedicle screw placement. An in vivo computed tomography analysis. Spine 22:452–458
Slomczykowski M, Hofstetter R, Burquin I, Nolte LP, Synder M (1998) [The method of computer-assisted orthopedic surgery based on two-dimensional fluoroscopy: the principles of action]. Chir Narzadow Ruchu Ortop Pol 63:443–450
Smith SW, Fehring TK, Griffin WL, Beaver WB (1995) Core decompression of the osteonecrotic femoral head. J Bone Joint Surg Am 77:674–680
Soucacos PN, Beris AE, Malizos K, Koropilias A, Zalavras H, Dailiana Z (2001) Treatment of avascular necrosis of the femoral head with vascularized fibular transplant. Clin Orthop Relat Res May:120–130
Steinberg ME, Larcom PG, Strafford B, Hosick WB, Corces A, Bands RE, Hartman KE (2001) Core decompression with bone grafting for osteonecrosis of the femoral head. Clin Orthop Relat Res May:71–78
Sugano N (2003) Computer-assisted orthopedic surgery. J Orthop Sci 8:442–448
Urbaniak JR, Harvey EJ (1998) Revascularization of the femoral head in osteonecrosis. J Am Acad Orthop Surg 6:44–54
Yoon TR, Song EK, Chung JY, Park CH (2000) Femoral neuropathy caused by enlarged iliopsoas bursa associated with osteonecrosis of femoral head—a case report. Acta Orthop Scand 71:322–324
Acknowledgments
The authors would like to thank the BrainLAB Company (Heimstetten, Germany) for providing the VectorVision® navigation system.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Beckmann, J., Goetz, J., Baethis, H. et al. Precision of computer-assisted core decompression drilling of the femoral head. Arch Orthop Trauma Surg 126, 374–379 (2006). https://doi.org/10.1007/s00402-006-0155-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-006-0155-0