
Abstract
Introduction: With the exception of forearm fractures, intramedullary techniques are preferred for osteosynthesis in the case of long-bone fractures. For the latter, however, the main problem remains insufficient stability against torsional forces resulting in high rates of non-union. This is why plate osteosynthesis by means of a DCP 3.5 or LC-DCP 3.5 is still being described as the standard procedure. Materials and methods: In a prospective study, 32 patients (33 forearms) with fractures of one or both forearm bones were treated by implantation of 40 intramedullary ForeSight™ nails (ulna: 23; radius: 17). Clinical and radiographic follow-up was performed at 6, 12, 26, and—if needed—52 weeks postoperatively. Time to follow-up was 31.4 months on average (range 24–44 months). Results: The average time to fracture healing for 36 fractures of 29 patients was 4.4 months. A free range of motion was seen in 86%, and only four forearms had a loss of pronation and supination. DASH score averaged at 13.7. There were few complications: non-union 1, delayed union 2, radioulnar synostosis 2, and infections 0. No refracture was seen after 19 implant removals so far. Average time needed per operation was 67 min, average time for fluoroscopy was 4.4 min. Conclusion: This intramedullary nail can do justice to the specific anatomical needs in the case of the forearm. Static interlocking guarantees adequate stability in all fracture types. The surgical technique is demanding. Nonetheless, this system can yield results of comparable quality to those of plate osteosynthesis. So far, no refractures after removal of the implants and no complications connected with the actual implants have been observed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Currently, long-bone shaft-fractures are preferably being treated by means of intramedullary nailing due to its superior biomechanical behaviour. Soon after Küntscher’s striking investigations had been finished, further nail developments (i.e. various interlocking possibilities, unreamed nailing techniques) led to a subsequent broadening of the spectrum of indications for these implants: Fracture locations now include metaphyseal regions, and high-grade open fractures are being stabilized with nails as well [11]. While all of this is true for the humerus, femur, and tibia, intramedullary nailing has not yet been able to establish itself for the treatment of fractures of the forearm due to a variety of unsolved problems. It is especially astonishing having in mind the fact that as soon as in 1913 Schöne [21] had published the possibility of “medullar casting” of the ulna by means of a silver rod measuring 2.8–4.0 mm in diameter. This was the first description of a nailing procedure following today’s nailing principles with an implant that is applied to the bone remote to the fracture site. Further developments [5, 22, 24] were neither able to be generally accepted, especially because of the limited spectrum of indications, the high rate of non-unions which is immanent to the procedure, and the additional need for plaster casting [14].
In contrast, plate osteosynthesis (DCP 3.5, or LC-DCP 3.5) allows immediate functional treatment postoperatively, and show mostly good results. Because of this, plate osteosynthesis is agreed to be the procedure of choice in the treatment of forearm fractures. However, there are disadvantages of the method as well: The need for a wide exposure of the fracture region, and especially the risk of a refracture after removal of the implant.
Functional integrity of the forearm is tightly connected with proper cooperation between ulna and radius in the distal and proximal radioulnar joint. Incongruity in these joints is caused by malalignment of either ulna or radius concerning length, axis, and torsion. It leads to the corruption of forearm rotation and can limit the function in adjacent joints. In terms of function, forearm fractures have to be looked at as “indirect” joint fractures with a need for adequate anatomical reduction [10, 13, 20]. This can usually be achieved more simply through open, direct reduction and stabilization, than through indirect measures.
Another related fact is the anatomical architecture of the forearm bones, especially of the radius, featuring an individually different bow shape in each patient. This is especially true for the frontal plane. Reconstruction of the original length of the radius, therefore, necessarily calls for reconstruction of the exact bow shape as well, since straightening the shape would cause lengthening of the radius. Any intramedullary implant, thus must be capable of adjusting to the non-straight anatomical form, excluding implants with merely straight designs.
The ulna/radius nail (ForeSight™ nail) now available seems to be featuring a concept that is able to compensate for biomechanical disadvantages and pitfalls of all former intramedullary devices. The purpose of this study was to prospectively evaluate the suitability of the ulna/radius nail (ForeSight™ nail) in radial and/or ulnar fractures.
Materials and methods
Implant
The solid steel nail that can be used for radius and ulna alike, allows for static interlocking. It comes with the diameters 4 and 5 mm, and has lengths ranging from 20 to 26 cm in 2 cm steps. The base of the nail is widened to 6 mm to enable the attachment of the aiming device for interlocking. The interlocking hole at the nail base has a diameter of 2.7 mm, while at the nail tip two perpendicular holes with a diameter of 1.9 mm each can be used. To interlock the nail, two screws come into action: The hole at the base needs a 2.7 mm fully threaded screw, the screw for the tip has a core diameter of 1.9 mm and a unicortical 2.7 mm thread.
Surgical technique
To fulfil their anatomical demands, especially concerning the reconstruction of the radial bow, the straight nails must be bent before insertion. In correlation to X-rays of the contralateral forearm, the curvatures of both forearm bones have to be predesigned in both planes by means of malleable nail templates. After sterilization of the templates, the suitable nail is being adapted intraoperatively to the templates according to the patient’s anatomy by means of a nail bender.
The nail is inserted through an incision of 1–2 cm, for the ulna centrally above the olecranon. For the radius, the entry portal lies on radial side of Lister’s tubercle in the bed of the extensor carpi radialis tendons. Protecting the peripheral division of the radial nerve, the intramedullar cavity is being opened by means of a 1.9 mm Kirschner wire and then being widened for the first 2 cm with a cannulated 6.0 mm reamer to fit the basis of the nail. By manual reaming without guide wire (starting with 3.0 mm and gradually increasing by 0.5 mm), the intramedullar cavity is widened further until the width of the canal lies 0.5–1.0 mm above the projected diameter of the nail. If closed reduction is not possible, it can be achieved by open reduction or percutaneous manipulation with a standard reduction forceps adjacent to the fracture line. After the nail has been adjusted to the individual anatomy, it can be inserted by hand or gently hammered into place using a slotted hammer. According to the fracture pattern, interlocking can then be performed either in a dynamic or static mode. Guides are used to facilitate locking the driving end of the nail while the locking screws at the nail tip are placed using the free-hand technique utilizing an image intensifier.
Patients
A prospective study was performed from June 1997 to December 2000 with 40 nails being inserted into 33 forearms of 32 patients. Included in this study were all patients, in which only the forearm was injured. Patients, which had sustained a polytrauma were only included, if this time-consuming operation did not have a negative influence on their other injuries. Seventeen nails were used for radial, 23 for ulnar fractures. In 23 forearms, fractures of only one forearm bone was seen (radius: 8, ulna: 15), in ten patients both forearm bones were fractured. The latter underwent nailing of both bones in seven cases. The remaining three were stabilized with a combination of a nail for the first and a plate osteosynthesis for the second bone for the following reasons: extensive soft-tissue injury with exposure of the fracture, and localization of the radial fracture in the distal fourth of the shaft. Fresh fractures were seen in 32 cases (among these a case of refracture after on-time removal of the plate, and another case of pathologic fracture), the remaining case featured a radial shaft fracture several weeks of age, that had elsewhere been stabilized with malalignment by means of a Kirschner wire. The average age of patients was 36.7 years (range 16–84), the distribution of gender showed a preference of the male sex with 23/9 cases. The left arm was fractured in 19 cases, the right one in 14. According to the classification of the AO/ASIF [16], 55% of the fractures could be categorized as type A (including 2 Galeazzi fractures, type A2.3), 32% were type B fractures (including 1 Galeazzi fracture, type B3.3), and 13% type C (Fig. 1). 84% of the fractures were closed, 30% of these showed only a mild or moderate degree of soft tissue damage. 16% of the injuries were open (grade I: 1; grade IIIA: 4) [6].

Fracture type (AO/ASIF) for 33 forearms (32 patients)
The majority of fractures were located in the mid-shaft area (73%). Only seven patients had suffered from isolated injuries of their forearms. Fourteen patients (44%) were polytraumatized, ten had additional injuries requiring surgery, another 13 had suffered additional head injuries. Thirty-six nails were interlocked in a static manner, four in a dynamic one.
With the exception of the three Galeazzi injuries, postoperative treatment regimen called for assisted exercise with unlimited active and passive motion of the elbow and wrist joint including forearm rotation without additional fixation by means of a plaster cast. Clinical and radiological follow-up was performed after 6, 12, 26, and 52 weeks, as well as after removal of the implant, which was generally done after 18 months at the earliest. In biplanar conventional radiographs, bony fusion was assumed if two independent observers found at least one of two cortices bridged in either plane. Delayed union was defined as the lack of bony fusion at 4 months postoperatively, as was non-union at 8 months.
Altogether, five patients could not be evaluated: two polytraumatized patients died from their associated injuries, one died from a co-existing malign disease, one had a change of procedure from nail to plate osteosynthesis for development of a non-union during follow-up, and another one was lost to follow up.
Thus, 34 nails (radius: 14, ulna: 20) in 28 forearms of 27 patients could be evaluated. The average period of follow-up was 31.4 months (range 24–44). Both, range of motion for the wrist- and elbow-joints, as well as the range of pro- and supination were evaluated according to the neutral-0–method and compared with the range of motion of the contralateral side in percentages. The functional result was determined by the use of the DASH score [9].
Results
Time to surgery was 7.0 days on average (range 0–68), whereas the one patient having undergone surgery after 68 days was the one who had been admitted from another hospital for correction of malalignment after Kirschner wiring. Seventy-eight percentage of all patients had undergone surgery within the first week after injury. Average amount of time per surgery performed was 67 ins. (range 27–150), total time of fluoroscopy needed per operation was 4.4 ins. (range 1.4–14.9).
Fractures were radiologically consolidated on an average after 3.5 months (range 2.6–11.6). Twenty-three forearms (82%) healed uneventfully between 3 and 6 months.
Complications
No cases were observed, in which intraoperative complications forced the surgeon to change the operative technique. Delayed union occurred in two cases with fractured ulnae, one of them being a refracture after plate osteosynthesis. In these cases, complete consolidation was achieved after 10.2 and 11.6 months, respectively, with the second case requiring removal of the interlocking screws 7.3 months postoperatively. One case of non-union was seen after a fracture of the distal third of the radial shaft. This complication was due to a postoperatively remaining fragment-distraction of about 3 m. Complete consolidation was achieved by a change of procedure removing the nail and applying a plate.
Radio-ulnar synostosis was seen in two cases: a distal fracture of the ulna, and a Galeazzi type fracture in the fourth sixth of the shaft. Both cases underwent early removal of the implant (5.8 and 13.3 months postoperatively), and resection of the bridging callus. On follow-up, however, they both showed limited range of motion for pro- and supination.
No deep or superficial infections occurred.
A removal of the nails was performed within the scope of other follow-up operations such as a radioulnar synostosis or if it was the patients wish. Nineteen nails have been removed after an average time of 18.3 months (range 5.8–29.1), and no refractures have been observed. Follow-up time after implant removal ranged from 3.9 to 51.8 months (averaging 18.3 months); 14 patients have been followed longer than 12 months.
Functional result
Within the examination, the extension/flection of the elbow and wrist joints as well as forearm rotation were measured and the values compared with the contralateral arm. A mean value of the measurements was used.
Twenty-two of 28 forearms (79%) showed a nearly unlimited range of motion (90% or more) compared with the contralateral arm. The limitation of motion was mostly caused by a restriction of pro- and supination: only 19 of 28 forearms (68%) attained 90% or more of the opposite arm, seven forearms showed a range of motion of 75% or less. In the cases with radioulnar synostosis, forearm rotation was seen to be 25 and 50% of the observed in the contralateral arm after callus dissection had been performed.
DASH questionary could be evaluated in 26 patients (27 forearms) because of a mental handicap of one patient. The score (0–100; 0 meaning an unlimited function) revealed results ranging from 0 to 63 points, with 20 forearms (74%) reaching 0–19 points meaning a very good functional result. Worse results (>20 points) are due to the two patients with bridging callus, the one with rheumatoid arthritis, one with severe additional ipsilateral injuries, two patients with a combination of ulna fracture and comminuted fracture of the distal radius, and one patient with a both bone forearm fracture combined with a dislocation of the distal radioulnar joint (Fig. 2).

DASH score for 27 forearms (26 patients)
Discussion
The problem of intramedullary forearm osteosynthesis
Biomechanical investigations [10] showed that the ulna is mainly responsible for stabilizing the forearm in respect to axial and torsional bending, meaning that biomechanical requirements for intramedullary implants are the lowest for isolated fractures of the radial shaft, increased for isolated ulnar fractures, and are the highest in combined fractures of both forearms. This is especially true for stability towards torsional forces, but for compressive forces as well; a fact, that comes into account in the treatment of C-type fractures. These biomechanical requirements for an intramedullary implant, complicated by the anatomical limitations of narrow intramedullar canals at the forearm, prevented gross establishment of intramedullary implants, despite many theoretical advantages including less-invasive therapy, integrity of the bone-soft tissue-complex, little cosmetic damage, little risk of refracture after removal of the implant.
Currently available implants suffer from insufficient torsional stability and require additional immobilization in a cast: a fact that—in adults—leads to worse functional results. In contrast, unacceptably high rates of non-unions (7% and more) [22] have been reported without additional immobilization. In these nail systems, torsional stability is theoretically provided by the nail profile. An obviously more stable type of stabilization is gained by bundle nails with a non-union rate of 3%. The nailable spectrum of injuries in respect to fracture location, however, is smaller due to the biomechanical principle of elastic capturing. Additionally for these implants, axial stability depends mainly on the fracture pattern, which is why C-type fractures usually are excluded [24].
This problem of stability after intramedullary osteosynthesis has led to the fact that plate osteosynthesis—preferably with DCP 3.5 or LC-DCP 3.5—so far has been favoured as the standard procedure in the treatment of fractures of the forearm.
Fracture healing
The time to bony consolidation experienced in our patients did not differ from that after plate osteosynthesis, bundle nailing, or interlocking nailing [3, 5, 24]. In three cases with ulna fractures located in the distal third, we could observe blurry areas of endosteal osteolysis adjacent to the distal tips of the implants (Fig. 3). We believe these morphological alterations are due to a certain lack of stability. One of these cases resulted in non-union, another one developed delayed union, the third one showed bony consolidation after 3.1 months.

Conventional X-ray with instability of the nail osteosynthesis showing endosteal osteolysis
For both plate osteosynthesis and bundle nailing, rates of non-union have been reported to be around 3% [3, 7, 17, 24]. Using the interlocking nail, we saw one case of non-union out of all cases followed-up so far. This patient, who sustained an open fracture of the distal part of his radial shaft, was treated by exchange plating. Both the fact of a hypertrophic type of non-union and the breakage of the distal interlocking screw after 6 months indicate insufficient stability of the osteosynthesis. It has to be mentioned, however, that this patient went back to full work as a butcher 8 weeks after surgery against surgical advice. According to our experience so far, we believe that currently published rates concerning non-unions of other nailing systems [22] can be reduced significantly by this implant and that it competes equal to plate osteosynthesis in this respect.
Radioulnar synostosis
Pathogenesis for the development of bridging callus after fracture of one or both forearm bones is not yet fully understood. Reasons could be primary damage to soft tissues, type of surgical approaches, bone grafting, or severe head- and brain-trauma [1]. The AO-/ASIF-multicenter-study describes a frequency of synostosis of 2.6% after plating [17], and of 2.1% after bundle nailing [24]. In our own patient clientele, we experienced two cases of bridging callus: one after a distal fracture of the ulnar shaft, another after a Galeazzi-type of fracture. Both the patients were multiply injured and had sustained head- and brain-trauma. The first patient developed further heterotopical ossifications throughout his injured areas (shoulder, thigh, abdomen after laparatomy). Implant-related development of synostosis, therefore, cannot be seen so far.
Refracture
Forearm plating is usually associated with refractures within 6–8 months after plate removal when evaluating typical complications. Published rates range from 0 to 22% [2–4, 7, 8]. Factors supporting this complication are the implant (DCP 4.5, semi-, or one-third tubular plates), premature removal of the implant, as well as multi-fragment, or defect fractures. DCP 3.5 and LC-DCP 3.5 have reported best results in that respect [3, 7, 12, 18]. However, a frequency of approximately 5% is to be expected. Atrophy of cortical bone in the plate bed along with drill holes for screws will cause weakening of the stability of forearm bones, both of which have relatively small diameters. This is complicated by remaining defects and the osteosclerotic incorporation of fragments with little or no blood supply (Fig. 4). Some authors [2, 15] therefore suggest to refrain from removal of the implants, whereas others [12, 19] reject this option due to the risks connected especially for young patients which recruit the majority for this injury.

Conventional X-ray of an ulnar refracture 18 months after plate removal
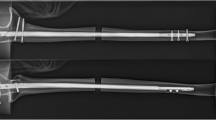
After intramedullary osteosynthesis, the fracture site is quickly remodelled by means of secondary, periosteal healing, as long as stability requirements are being kept. For bundle nailing, a refracture rate of 1% is published [24]. Street nail was shown to be 2.9% [22]. For ForeSight™ nail in our study, conventional X-rays at the time of bony healing showed solid osseous regeneration throughout (Fig. 5), which is why refractures have not been observed so far after removal of 19 nails, 14 of them having been followed for 8 months or more.

a–c Conventional X-rays of a forearm-fracture (a), six weeks postoperatively after intramedullary nailing (b), at time of implant removal; note: excellent bone remodelling visible (c)
Reduction
Anatomical reduction is essential for unimpaired function. Since most often reduction during intramedullary nailing procedures will be performed in an indirect manner, this step requires utmost attendance. Especially for the radius, the nail’s curvature must be individually adjusted to the anatomical situation to avoid malalignment. In other words, the nail corresponds to the anatomy, and not vice versa. Adjustment of the nail by means of the template is tricky and causes additional pre- and intraoperative endeavours. If performed correctly, however, it helps to avoid malalignment. Malalignment of more than 10° will cause functional impairment [13, 20]; in our series, none of the patients reached this limiting mark. Restoration of the correct length of forearm bones is essential as well, especially if the pattern of injury includes the distal or proximal radioulnar joint (Galeazzi-, Monteggia-type lesion). The possibility of static interlocking will secure the result of any reduction manoeuvre.
Twenty-four fractures could be reduced in a closed manner: two cases needed manipulation of the fragments adjacent to the fracture site by means of a standard reduction forceps, without opening the fracture site itself. Fourteen fractures were reduced openly, if the fracture itself presented open, or if closed reduction remained unsuccessful. No investigation so far has shown an influence of the type of reduction (closed; open) on the outcome of the injury; this is why we favour closed reduction, but do not hesitate to switch to open technique if the whole procedure threatens to run off an appropriate timeline. If reduction is performed in an open manner, avoidance of devascularization of fragments is crucial by all means.
Design of the implant—surgical technique
In contrast to preshaped nails, ForeSight™ nail enables an individual adjustment of the implant to the anatomy. This is why only one implant is needed for both forearm bones. This advantage goes along, however, with additional time needed pre- and intraoperatively to bend the nail. Beyond that, we suggest an X-ray of the uninjured forearm for fitting the templates. Classic technique of interlocking obviously guarantees enough stability against torsion, bending, and distraction/compression forces, even if early functional physiotherapy is employed postoperatively. With the exception of one broken screw no cases of implant failure were observed in our series so far.
Free hand technique using the image intensifier for interlocking at the tip site of the nail is tricky as well due to miniature anatomical scales. This grossly contributes to the average operative time which—especially at the beginning of our learning curve—was relatively long. Even more than that, this fact is mainly responsible for the times of which intraoperative fluoroscopy was applied. The instruments offered for distal interlocking does not seem to fully fit needs, which is why we preferred a radiolucent ankled drill-drive with 2.0 drill or 2.0 mm drill. Although maximum figures for total time needed per operation (150 min), and total time of intraoperative fluoroscopy (14.9 min) could be decreased going through our learning curve, a time of 4 min of fluoroscopy needed per operation remains realistic even for the experienced surgeon. Like all techniques that apply indirect methods, however, some of that time is needed for nail positioning and reduction.
Interlocking at the proximal radius can hurt the deep branch of the radial nerve: this fact has to be explained to the patient before an informed consent is given. To avoid iatrogenic damage to this nerve, interlocking should be performed no more than 3 cm distal of the radial head, coming from a radial direction, and holding the forearm in a neutral position for rotation [23]. In our series, we did not observe this complication. Damage of the ulnar nerve can be avoided by meticulous preparation at the olecranon for nail insertion. Damage of the superficial branch of the radial nerve can be avoided by careful preparation at the site of Lister’s tubercle. Paying attention to these demands, no nerve damage was seen in our series.
Conclusions
According to our own experience so far, the interlocking nail introduced here is considered a favourable alternative to standard plate osteosynthesis. Advantages are high rates of bony consolidation along with minimized surgical approaches and little risk of refracture after removal of the implant. Especially complex fracture pattern (C-type injuries) are stabilized in an elegant manner without additional damage to soft tissues. Disadvantages are a fiddling surgical technique along with prolonged times during which fluoroscopy is needed.
References
Bauer G, Arand M, Mutschler W (1991) Post-traumatic radioulnar synostosis after forearm fracture osteosynthesis. Arch Orthop Trauma Surg 110:142–145
Bednar DA, Grandwilewski W (1991) Complications of forearm-plate removal. Can J Surg 35:428–431
Chapman MW, Gordon JE, Zissimos AG (1989) Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg (Am) 71:159–169
Deluca PA, Lindsey RW, Ruwe PA (1988) Refracture of bones of the forearm after the removal of compression plates. J Bone Joint Surg (Am) 70:1372–1376
DePedro JA, Garcia-Navarrete F, Garcia De Lucas F, Otero R, Oteo A, Lopez-Duran-Stern L (1990) Internal fixation of ulnar fractures by locking nail. Clin Orthop 283:81–85
Gustilo RB, Gruniger RP, Davis T (1987) Classification of type III (severe) open fractures relative to treatment and results. Orthopaedics 10:1781–1788
Hertel R, Pisan M, Lambert S, Ballmer FT (1996) Plate osteosynthesis of diaphyseal fractures of the radius and ulna. Injury 27:545–548
Hidaka S, Gustilo RB (1984) Refracture of bones of the forearm after plate removal. J Bone Joint Surg (Am) 66:1241–1243
Hudak PL, Amadio PC, Bombardier C, The Upper Extremity Collaborative group (UECG) (1996) Development of an upper extremity outcome measure: the DASH (Disabilities of the Arm, Shoulder, and Hand). Am J Ind Med 29:602–608
Jones DJ, Henley MB, Schemitsch EH, Tencer AF (1995) A biomechanical comparison of two methods of fixation of fractures of the forearm. J Orthop Trauma 9:198–206
Krettek C, Schandelmaier P, Tscherne H (1997) Neue Entwicklungen bei der Stabilisierung dia- und metaphysärer Frakturen der langen Röhrenknochen. Orthopäde 26:408–421
Labosky DA, Cermak MB, Waggy CA (1990) Forearm fracture plates: to remove or not to remove. J Hand Surg 15:294–301
Matthews LS, Kaufer H, Garver DF, Sonstegard DA (1982) The effect on supination-pronation of angular malalignment of fractures of both bones of the forearm. J Bone Joint Surg (Am) 64:14–17
McAuliffe JA (1997) Forearm fixation. Hand Clin 13:689–701
Mih AD, Coone WP, Idler RS, Lewallen DG (1994) Long-term follow-up of forearm bone diaphyseal plating. Clin Orthop 299:256–258
Müller ME, Allgöwer M, Schneider R, Willenegger H (1991) Manual of internal fixation. Springer, Berlin Heidelberg New York
Oestern HJ, Tscherne H (1983) Ergebnisse der AO-Sammelstudie über Unterarmschaftfrakturen. Unfallchirurg 86:136–146
Rosson JW, Shearer JR (1991) Refracture after the removal of plates from the forearm. An avoidable complication. J Bone Joint Surg (Br) 73:415–417
Rumball K, Finnegan M (1990) Refractures after forearm plate removal. J Orthop Trauma 4:124–129
Schemitsch EH, Jones D, Henley MB, Tencer AF (1995) A comparison of malreduction after plate and intramedullary nail fixation of forearm fractures. J Orthop Trauma 9:8–16
Schöne G (1913) Zur Behandlung von Vorderarmfrakturen mit Bolzung. Münch Med Wochenschr 60:2327–2328
Street DM (1986) Intramedullary forearm nailing. Clin Orthop 212:219–230
Tabor OB, Bosse MJ, Sims SH, Kellam JF (1995) Iatrogenic posterior interosseous nerve injury: is transosseous static locked nailing of the radius feasible? J Orthop Trauma 9:427–429
Winckler S, Brug E, Baranowski D (1991) Bündelnagelung bei Unterarmfrakturen. Indikation und Ergebnisse. Unfallchirurg 94:335–341
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Weckbach, A., Blattert, T.R. & Weißer, C. Interlocking nailing of forearm fractures. Arch Orthop Trauma Surg 126, 309–315 (2006). https://doi.org/10.1007/s00402-006-0122-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-006-0122-9