
Abstract
Introduction
Compression of the median nerve at the wrist by a persistent median artery is one of the uncommon reasons for carpal tunnel syndrome. Most of the studies in the literature deal with thrombosed persistent median artery.
Materials and method
In this study, we present surgical treatment of four carpal tunnel syndromes, which had persistent median arteries. The mean age of the patients was 51 years. All four median arteries were patent and only transverse carpal ligament releases were performed using a standard anterior open approach for decompression of the carpal tunnel. Neither ligation nor transposition of the arteries was done.
Results
All patients became symptom free after a few weeks. Only one patient had a slight recurrence 13 months postoperatively. Splint use and modification of her activities reduced her disturbance, and no further treatment was applied.
Conclusion
If the patient has no additional anomaly, our clinical experiences lead us not to advise resection or transposition because simple release of the transverse carpal ligament can relieve symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Compression of the median nerve at the wrist is the commonest nerve entrapment syndrome. The syndrome classically presents with paresthesia in the distribution of the median nerve associated with wasting and weakness of thenar muscles [1].
The most common cause is tenosynovitis of the flexor tendons, but a variety of etiologies has been described in the literature [8]. One of the rare etiologies of the carpal tunnel syndrome (CTS) is the persistent median artery (PMA), increasing pressure of the median nerve by an enlarged median artery.
The majority of the studies in the literature pertained to thrombosed PMA. Barfred at al. reported the largest series with nine patients: three with thrombosed and six with patent PMA. In this current study, we present four cases, making it the second largest series in the English literature, to share our experience and clinical approach to patent PMA that may cause carpal tunnel syndrome.
Materials and methods
A total of 524 carpal tunnel releases were performed between October 1995 and May 2002 in our department, 313 of which were performed using a standard anterior open and one-incision mini-open approach and the remaining 211 cases by dual portal endoscopic technique (modified Chow’s technique). There were 273 women and 40 men in the open approach group. There were four patients with PMA in this group, all of whom were woman with a mean age of 51 years. We evaluated these patients based on their subjective symptoms such as pain, paresthesia, numbness in the radial three digits, awakening at night with pain and additional clinical findings such as Phalen’s test, Tinel’s sign, and two-point discrimination. Only transverse carpal ligament releases were performed for these four patients with an average follow-up of 42 months. In this study, we review the patients and summarize the details of the clinical follow-up.
Results
There were 4 patients (1.2%) with PMA among 313. The onset of symptoms was gradual in all cases. All involved extremities were dominant and unilateral except one. Only one patient had bilateral symptoms, but her complaint in the dominant hand was evident. Nocturnal symptoms were present in all patients, but using the hand easily increased paresthesia and pain. Phalen’s test and Tinel’s sign were positive for all. Sensibility and two-point discrimination were slightly disturbed in all cases. Conservative treatment [splint and administration of nonsteroidal anti-inflammatory drug (NSAID) for 6 weeks] failed in all.
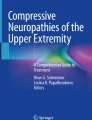
Intravenous regional anesthesia (IVRA) was used after exsanguinating the limb with an Esmarch bandage for CTS release routinely. The procedures were performed using a standard anterior open incision. All of the PMA were diagnosed during the operation and all seemed to be normal; none of the arteries were thrombosed or aneurysmatic. Not being sure about the configuration of the superficial palmar arch, neither ligation nor transposition of the arteries was done. Two of the median arteries were big (≥2 mm), the others were medium size (<2 mm), and none of them were filiform epineural arteries (Fig. 1). None of the patients had other possible causes of CTS such as excessive tenosynovitis. The simple release of the transverse carpal ligament release was performed alone.

Medium-sized patent median artery was found lying anterior to the median nerve. The limb was exsanguinated with an Esmarch bandage under intravenous regional anesthesia
The symptoms of all of the patients started to abate after 1 week and they all became symptom free after 4 weeks. The patients returned to activities of daily living after approximately 6 weeks. We have detected no recurrence of symptoms up to date in all patients except one. Only subjective symptoms of that patient began to appear at 13 months postoperatively. Her pain and paresthesia became evident during work and nocturnal symptoms were present, but she has no positive Phalen’s test or Tinel’s sign. Splint use and modification of her activities reduced her disturbance, and no further treatment was applied.
Discussion
The metacarpal bones and transverse carpal ligament cover the carpal tunnel through which the median nerve and extrinsic flexor tendons pass [1]. Any condition that reduces the volume of the tunnel will increase the pressure of the median nerve. The median artery is a transistory vessel that develops from the axillary artery in early embryonic life and does not normally survive until postfetal life. In a small percentage of individuals, it persists into adulthood and is generally asymptomatic [3, 7, 8]. A persistent median artery can be blamed as the cause of carpal tunnel syndrome rarely, increasing the pressure of the median nerve by an enlarged median artery.
The study of McCormak et al. indicated that a PMA was found to be present in 2.1% of 750 arms [2]. Other incidence studies reported the existence of a median artery in 3% (Edwards) and 10% of 60 arms (Pecked et al.) [2]. On the other hand, Olave et al. reported the incidence of a median artery at 23%, which is higher than the incidence of carpal tunnel syndrome itself [6]. We encountered only 4 cases (1.2%) among 313 cases treated by an open approach.
In this current study, the onset of symptoms in all cases was gradual and the arteries were all patent as mentioned by Barfred et al. [2]. Therefore, the symptoms in CTS that may be caused by PMA without any complication take place gradually. Nocturnal symptoms were present in all of our cases. Exacerbation of symptoms by using the hands was obvious in all cases, both in Barfred et al.’s and our series.
Many authors offer to perform excision when the artery is thrombosed, or transposition as far as possible when the artery is still patent, but their studies indicate that excision may cause circulatory problems in the digits [1, 2, 3, 5]. According to Chalmers, if the vessel is still open there is no evidence that it is necessary to resect it [2]. Resection however involves the potential for vascular compromise to the fingers and should not be performed without thorough evaluation of radial and ulnar arteries and the aberrant arteries’ relative contribution to the hand’s circulation [8]. A PMA makes a remarkable contribution to the circulation of the hand in 4–5% of cases [8].
Barfred et al. reported a series of six patients who had CTS caused by a patent PMA. Four had no primary resection of PMA and two of these showed no improvement and were reoperated on with resection of the vascular bundle, resulting in total relief of their symptoms. The other two were symptom free. Barfred et al. reported 50% persistence of symptoms if the artery was left undisturbed [2]. If the vascular bundle thromboses, it should undoubtedly be excised.
Kato et al. showed that even an endoscopic release procedure is effective for increasing the cross-sectional area and volume of the carpal canal [4]. Being inspired by that idea and because of using IVRA and not having a chance to test the contribution of a PMA to the circulation, we performed anterior open release of the carpal tunnel in our patients. None of our patients experienced persistence of any symptoms. Only one patient with a big median artery (>2 mm) experienced a slight recurrence 13 months postoperatively.
In the study of Olave et al. in which cadaver dissection and latex injection were performed, they found the median artery in 23 of 102 cases (23%), and its calibers ranged from 0.7 to 2.7 mm, mean (SD) 1.6 (0.5) mm. That incidence is much higher than the carpal tunnel syndrome itself [6]. This high rate of incidence and correlation raises the question: “Can a persistent median artery cause carpal tunnel syndrome?” Probably, a median artery can be persistent as an anatomic variation in most CTS cases, but a persistent median artery can be blamed in young adults and those without excessive tenosynovitis.
If a persistent median artery is the cause of CTS by increasing the carpal canal volume, the amount of decompression will determine the final outcome. Our clinical experiences have led us not to advise resection or transposition if the patient has no additional anomaly because simple release of the transverse carpal ligament can relieve symptoms. This approach would save the surgeon from a dilemma if one were not sure about the configuration of the superficial palmar arch when confronted with a median artery during the release procedure.
References
Balakrishnan C, Smith MF, Puri P (1999) Acute carpal tunnel syndrome from thrombosed persistent median artery. J Emerg Med 17:437–439
Barfred T, Hojlund AP, Bertheussen K (1985) Median artery in carpal tunnel syndrome. J Hand Surg [Am] 10:864–867
Jones NF, Ming NL (1988) Persistent median artery as a cause of pronator syndrome. J Hand Surg [Am] 13:728–732
Kato T, Kuroshima N, Okutsu I, Ninomiya S (1994) Effects of endoscopic release of the transverse carpal ligament on carpal canal volume. J Hand Surg [Am] 19:416–419
Khashaba A (2002) Carpal tunnel syndrome from thrombosed persistent median artery. J Emerg Med 22:55–57
Olave E, Prates JC, Gabrielli C, Pardi P (1997) Median artery and superficial palmar branch of the radial artery in the carpal tunnel. Scand J Plast Reconstr Surg Hand Surg 31:13–16
Rose RE (1995) Acute carpal tunnel syndrome secondary to thrombosis of a persistent median artery. West Indian Med J 44:32–33
Zeiss J, Guilliam Haidet L (1993) MR demonstration of a persistent median artery in carpal tunnel syndrome. J Comput Assist Tomogr 17:482–484
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bilgin, S.S., Olcay, S.E., Derincek, A. et al. Can simple release relieve symptoms of carpal tunnel syndrome caused by a persistent median artery?. Arch Orthop Trauma Surg 124, 154–156 (2004). https://doi.org/10.1007/s00402-004-0637-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-004-0637-x