
Abstract
A first episode of depression after 65 years of age has long been associated with both severe macrovascular and small microvascular pathology. Among the three more frequent forms of depression in old age, post-stroke depression has been associated with an abrupt damage of cortical circuits involved in monoamine production and mood regulation. Late-onset depression (LOD) in the absence of stroke has been related to lacunes and white matter lesions that invade both the neocortex and subcortical nuclei. Recurrent late-life depression is thought to induce neuronal loss in the hippocampal formation and white matter lesions that affect limbic pathways. Despite an impressive number of magnetic resonance imaging (MRI) studies in this field, the presence of a causal relationship between structural changes in the human brain and LOD is still controversial. The present article provides a critical overview of the contribution of neuropathology in post-stroke, late-onset, and late-life recurrent depression. Recent autopsy findings challenge the role of stroke location in the occurrence of post-stroke depression by pointing to the deleterious effect of subcortical lacunes. Despite the lines of evidences supporting the association between MRI-assessed white matter changes and mood dysregulation, lacunes, periventricular and deep white matter demyelination are all unrelated to the occurrence of LOD. In the same line, neuropathological data show that early-onset depression is not associated with an acceleration of aging-related neurodegenerative changes in the human brain. However, they also provide data in favor of the neurotoxic theory of depression by showing that neuronal loss occurs in the hippocampus of chronically depressed patients. These three paradigms are discussed in the light of the complex relationships between psychosocial determinants and biological vulnerability in affective disorders.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mood disorders in late life are seen as the final byproduct of complex interactions between genetic predispositions, environmental influences, and neurobiological abnormalities [7, 14, 16, 88, 97]. Depressive illness is projected to be the second leading cause of disease burden after ischemic heart disease by year 2020 [145]. With the demographic transition observed in most Western countries, this burden is progressively shifting towards the older age groups. Clinically significant depressive syndromes can be found in 8–16 % of community-dwelling, about 25 % of primary care, and 23 % of hospitalized older adults (i.e., adults aged 60 years or older) [18, 112], and are associated with disability, decline in overall health, increased use of medical services and increased mortality rates through suicide and complications of comorbid diseases [6, 15, 67, 71]. A large number of older adults develop depression for the first time in their lives after age of 60, often in the presence of multiple health problems [85, 86]. Introducing the concept of “arteriosclerotic depressive disease” in his 1905 treatise, Gaupp [51] was the first to consider the impact of cerebrovascular pathology on mood regulation. The relationship between the accumulation of vascular lesions in the human brain and affective disorders remained, however, controversial before the experimental work of Robinson and collaborators [102] who demonstrated the role of middle cerebral artery lesions in the development of behavioral and cellular changes compatible with depression. Progressively, three apparently distinct theoretical models have been developed to describe the complex interactions between vascular burden and emotional disturbances in late life. The first one referred to the traumatic consequences of acute vascular pathology and was initially based on the higher incidence of depression in elderly patients during the 2-year period following stroke as compared to those having a comparable degree of disability caused by other medical conditions [47]. According to the first description of this model, stroke induces an abrupt biological stress not only by affecting cortical circuits involved in the emotional regulation and cognitive appraisal but also by interrupting the projections ascending from midbrain and brainstem, leading to a decreased bioavailability of the biogenic amines. This traumatic status of the human brain may increase the psychological reactions that are usually present in chronic medical conditions characterized by increased functional disabilities (for review see [1, 69, 83]). In contrast to this conceptualization that points to the catastrophic impact of acute brain damage on mood, the second model focused on the progressive accumulation of small macrovascular and microvascular lesions in old age and its possible neurocognitive and affective repercussions. It highlighted the impact of an existing burden of vascular pathology on the development of first episodes of depression in late life. The terms of vascular depression and depression-executive dysfunction syndrome attempted to define the morphological substrates of the atypical clinical expression of depressive illness in the elderly, regrouping psychiatric, neuropsychological and, in certain cases, pure neurological symptoms [12, 121, 122, 128]. Besides the possible causal link between vascular burden and first episode of depression after 65 years of age, the neurotoxic hypothesis of depression provided an attractive theoretical framework to explain the concomitant presence of mood dysregulation and cognitive deficits in elderly patients with long-lasting depression. Unlike the two previous models that mainly concern the first episodes of depression in late life, no distinctive histopathology was incriminated here, the persistence of clinical symptoms over time thought to be the indirect consequence of neuronal and synaptic loss caused by neuroendocrine abnormalities [54, 66, 100, 101, 108, 116]. To examine the pertinence of these models, we provide here a comprehensive review of the morphological correlates of depression in late life combining structural neuroimaging contributions and neuropathological validation studies. To facilitate reading and despite the unavoidable overlap of the neurobiological mechanisms surrounding post-stroke, late-onset and recurrent late-life depression, we opted to describe each model separately before commenting on their pertinence.
Post-stroke depression: the traumatic model of late-life mood disorders
Post-stroke depression affects one-third of stroke survivors [57] and is associated with poor functional recovery, decreased quality of life, and increased mortality [109]. Besides the core signs of depression, the main clinical symptoms include catastrophic reactions, hyperemotionality, and diurnal mood changes [50]. Early-onset forms (<6 months post-stroke) are characterized by frequent anxiety, loss of libido, and feelings of guilt, whereas late-onset cases display social isolation and diurnal mood changes [98]. However, these descriptions are by far not widely accepted. A recent study from Cumming et al. [38] explored further the claims for a phenomenologic distinction between post-stroke depression (PSD) and depression without brain injury and reported a broadly similar symptomatic profile with the exception of “inability to feel” and “disturbed sleep” levels that were significantly higher in non-PSD depressed patients.
The relevance of stroke location in PSD: MRI findings
Stroke location has been long considered as the main determinant of PSD. The initial concept was that abrupt ischemia interrupts the projections ascending from midbrain and brainstem, leading to a decreased bioavailability of the biogenic amines—serotonin (5HT), dopamine (DA) and norepinephrine (NE) and possibly acetylcholine (for review see [83]). Subsequently, cases with a massive damage of frontal lobe association and limbic areas may be more prone to mood disorders compared to those with posterior parietal or occipital lobe macroinfarcts. To explore the validity of this hypothesis, several magnetic resonance imaging (MRI) studies were conducted in patients with PSD by the end of 1990s. Robinson et al. [104] reported first a 2-year longitudinal study and found that patients with left-sided frontal cerebral lesions were more at risk to develop PSD when compared to patients with right hemisphere or left hemisphere posterior lesions. This pioneer work was followed by more than 50 MRI studies in hospital dwelling samples that led to conflicting data. In their extensive review, Vataja et al. [141] supported the positive association between PSD and left prefrontal-subcortical location and volume size. However, two systematic reviews challenged this viewpoint and pointed to the main methodological problems of previous studies including PSD definition, small sample sizes, and lesion characterization [17, 30]. In a timely review based on the analysis of 38 neuroimaging studies, Bhogal et al. reported that the source of sampling could be a major determinant of the relationship between stroke location and occurrence of depression. In this work, left hemisphere lesion location was significantly associated with PSD in hospital-based population studies, whereas the inverse was true in community-based studies. Carson et al. [30] found no association between PSD and lesion location in a pooled analysis of 34 primary studies. A cortico-subcortical involvement of the temporal lobe and internal capsule, increased numbers of cerebral microbleeds and deep white matter hyperintensities were all associated with the occurrence and severity of PSD [125, 126, 149, 150].
Microvascular lesions predict PSD: post-mortem observations
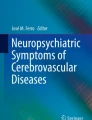
Neuropathological explorations that may shed some light on the anatomic substrates of PSD remain scarce. In a first study assessing the relationship between the presence of diffuse or focal macrovascular pathology and the occurrence of depressive symptoms in the first 2 years following stroke, we did not find a significant impact of these lesions in the development of clinically overt depression [20]. Later on, Brodaty and collaborators [24] postulated that more than stroke location, the progressive accumulation of small macrovascular and microvascular lesions may determine the occurrence of PSD. To address this issue, we assessed lacunes and microvascular lesions in 41 post-mortem brains of stroke patients, 20 having developed PSD and 21 without depression. The presence of lacunes in subcortical regions, namely in the thalamus, basal ganglia, and deep white matter was strongly related to the development of PSD explaining 25 % of the variability of this occurrence (Fig. 1) [106]. In conjunction with our previous work in cognitively impaired elders, this finding suggests that the development of subcortical lacunes may constitute a common denominator of cognitive and mood disorders in late life [53].

Representative example of a patient sufferring from late-onset major depressive disorder. Macroscopic (a) and histological views (low magnification in b, higher magnification in c) of multiple lacunes in basal ganglia. b, c hematoxylin–eosin staining. Scale bar b 6.5 mm; c 1.2 mm
Future perspectives: combining biological and psychological determinants of PSD
The interaction between biological determinism and psychosocial mechanisms in the etiology of PSD remains, however, a highly controversial issue [1, 45, 58, 70, 89, 103, 108]. The relationship between PSD and physical disability is complex and certainly goes beyond the commonly held notion that depression after stroke is a typical consequence of physical impairment [139]. In fact, psychological reactions to loss during stressful life periods are at least partly biologically determined. In the same line, even in the case of the absence of social contacts, shown to be a main psychosocial determinant of PSD [11], the direction of the relationship remains ambiguous as they may be both a cause and a consequence of PSD. In a recent attempt to conciliate the biological and psychosocial dimensions of PSD, Hama et al. [60] proposed a distinction between an affective PSD form with predominant depressed mood and an apathetic form characterized by loss of interest. Using specific symptom scales for each PSD subtype, these authors aimed to correlate these symptoms to lesion location in two sets of 243 and 101 stroke patients, respectively. In both samples, they found that affective PSD was associated with left frontal lobe damage while apathetic depression was more frequent in patients presenting with basal ganglia damage [59]. Apathy has also been associated with subcortical lesions by other authors [120]. A recent SPECT study by Onoda et al. [96] found that the lesions of left basal ganglia were associated with hypoperfusion of bilateral basal ganglia in an apathetic group of 37 patients when compared to 65 non-apathetic patients with major depression. In line to conciliate the biological and the psychological etiologic perspectives on PSD, a recent study reported no relationship between hemispheric location, level of social support, age, gender, or compliance to antidepressive treatment and the development of PSD, but a strong association between a good response to psychosocial treatments and serotonin transporter polymorphisms [73].
Neurocognitive changes and vascular burden in late-life depression
Neuroimaging data
Several studies supported the idea that depression in older people might have a different etiology from depression in younger adults. For instance, individuals with early-onset major depression are likely to have a positive family history for this disorder, whereas later age at onset of depression has been associated with subcortical vascular pathology [3, 23, 26, 72].
In the last decades, two main sets of experimental data supported the presence of significant vascular pathology in the brain of elderly individuals with depressive illness. The first concerns diffusion tensor imaging (DTI)-based investigation of white matter tracts that documented a great variety of deficits affecting both neocortical association areas and subcortical nuclei. The second refers to the frequent coexistence of cognitive deficits primarily affecting executive functions, white matter hyperintensities and late-life depression [76, 127].
DTI is an MRI technique based on the analysis of the diffusion of water in tissues that provides indirect evidence about the microstructure of white matter. Fractional anisotropy (FA) and mean diffusivity (MD) are the most commonly assessed parameters thought to reflect white matter integrity [148]. Several teams used DTI to investigate the presence of subtle changes in white matter tracts occurring in late-life depression [34, 39, 115, 123]. Colloby [34] recently used the tract-based spatial statistics (TBSS) analysis, an automated whole brain analysis method (for its description see [142]), to detect white matter brain abnormalities in an elderly population of 30 controls and 38 subjects with late-onset depression (LOD). They found a lower FA in these regions, suggesting white matter fiber lesions of numerous tracts, such as the corpus callosum, the uncinate fasciculus, the inferior fronto-occipital fasciculus, the inferior longitudinal fasciculus, and the corticospinal and corticopontine tracts. Further research in the field attempts to identify connectivity deficits in late-life depression. Dalby et al. [39] showed a positive correlation between the severity of depression and loss of integrity of white matter fiber tracts (including the left superior longitudinal fasciculus and the right uncinate fasciculus) in LOD. A study using DTI excluding white matter hyperintensities from the analysis of an elderly depressed population, found an increased MD in the prefrontal regions in the depressed compared to healthy controls [115]. A new interesting approach is the combination of structural and functional markers to elucidate possible underlying connectivity deficits. Steffens et al. used DTI and the resting-state BOLD to test whether impaired structural integrity of the uncinate fasciculus is coupled with decreased activation of target regions. They found positive correlations between left uncinate fasciculus FA values and resting state functional connectivity in left ventrolateral prefrontal cortex and amygdala, as well as left ventrolateral prefrontal cortex and hippocampus [123]. DTI has been lately combined with neuropsychological assessment to identify MRI correlates of neuropsychological impairment in elderly depressed patients. Sexton et al. [113] found a positive correlation between reduced FA of anterior thalamic radiation, the corpus callosum, the uncinate fasciculus and impaired executive function and episodic memory.
Overall, it remains quite hard to draw definite conclusions from voxel-based morphometry (VBM) and DTI findings, in spite of a large number of studies. Even though several groups have replicated some MRI patterns, others reported negative data. Methodological differences related to small sample sizes, as well as the chronicity of depressive episodes and effects of treatment, not always taken into account in the analysis and interpretation of results, may partly explain discrepancies. Moreover, the existence of some of these deficits in younger depressed patients challenged their real relevance in the context of late-life depression [37, 65, 80].
The strongest argument in favor of the neurocognitive origin of late-life depression comes, however, from the study of white matter hyperintensities coupled with executive deficits in old depressed patients within the theoretical framework of the “vascular depression” hypothesis [124]. Executive dysfunction and episodic memory impairment constitute the most prominent symptoms in patients with LOD after remission [93], and patients with LOD present with a more frequent and rapid cognitive decline compared to early-onset depression (EOD) cases and controls in neuropsychological studies [63, 74]. The first neuroimaging studies in this field pointed to the role of white matter hyperintensities as a possible trigger or at least correlate of LOD. According to the “vascular depression hypothesis” [5], the presence of increased white matter hyperintensities in some elders reflects a predisposition for the development of depression, through the fiber tract disruption of frontostriatal circuits. In their systematic review, Herrmann et al. [64] found a fourfold higher prevalence of deep and periventricular WMH in LOD when compared to EOD. Similar conclusions were reached by Tham [130] and colleagues in their recent review on late-life depression. The European multi-centre study (LADIS) investigated the relationship between WMH, cognitive impairment and depression. After controlling for cognitive impairment, these data indicate a stronger association between deep white matter lesions and depressive symptoms compared to periventricular ones [76]. Recent functional MRI studies added credit to the vascular depression concept. For instance, there was a positive correlation between WMH burden and BOLD fMRI activity in subgenual cingulate cortex during a facial expression affective reactivity task supporting the idea that high WMH burden in late-life depression disrupts the brain mechanisms of affective regulation leading to hyperactivation of limbic areas involved in mood regulation such as hippocampus and cingulate cortex [2]. In the same line, increased activation of the dorsomedial prefrontal cortex during the performance of a low cognitive load event-related task that correlated with WMH burden was recently reported in late-life depression [147].
In our recent cross-sectional and longitudinal studies, Delaloye et al. [41, 144] confirmed these observations in a prospective analysis of euthymic, EOD and LOD patients and control subjects combining MRI investigation and neuropsychological assessment. They found a higher degree of white matter hyperintensities in LOD patients, as well as decreased performances in episodic memory tasks, while euthymic EOD patients manifested a preserved episodic memory capacity, replicating previous findings in younger age groups [22, 74]. In the same line, a longitudinal study of a large sample size showed that the severity of white matter changes predicts the development of depressive symptoms at 1 year from the baseline [129]. Together with the clinical criteria of a more frequent presence of cardiovascular risk factors such as hypertension, dyslipidemia and a history of cerebrovascular disease, a higher burden of WMH was proposed to be a diagnostic criterion for vascular depression [5]. The same authors also introduced the concepts of “depression-executive dysfunction syndrome of late life” [4] and “subcortical ischemic depression” [75] and proposed that the disruption of frontostriatal circuits by vascular lesions constituted the main pathophysiological mechanism underlying depressive symptoms in old age.
Despite a decade’s worth extensive literature on the association between LOD and cardiovascular risk factors, the underpinnings of the “vascular depression” construct are still difficult to disentangle (for review see [27, 133, 137]), and datasets from different fields seem to ascribe it dissimilar significance. One of the points that remain controversial is the etiologic role of WMH in late-life depression, given their frequent association with cardiovascular risk factors as well as with advanced age [39, 99, 142]. Moreover, results on the validity of the symptom profile attributed to “vascular depression” phenotype are conflicting. Together with the Longitudinal Aging Study Amsterdam (LASA) community-based results from Naarding et al. [92], McDougall’s [90] recent systematic review of the literature failed to support a clinically recognized subtype of vascular depression [119, 137].
Besides sampling differences, several methodological reasons may explain the observed discrepancies in neuroimaging studies including the pathological heterogeneity of WMH, the frequent failure to take into account site and lateralisation of lesions and inter-rater variability in respect to the radiological criteria for white matter lesions (WML) [64]. In a recent review based on neuroimaging and neuropathological data, Casanova et al. [31] did not identify a reliable association between WMHs and depression in different types of dementia. WML heterogeneity and its correlation with age was also recently reviewed by Schmidt et al. According to authors periventricular WMH seem to have a non-vascular origin, whereas the majority of deep, subcortical WMH correspond to incomplete ischemic destruction [111]. Most neuroimaging–histopathological correlations have established that WMH can correspond to a wide variety of histologic processes such as arteriosclerosis, perivascular demyelination, dilated perivascular spaces, vascular ectasia, ischemia, incomplete infarction, partial loss of myelin and axons, gliosis, infarction with necrosis, and congenital diverticula [21, 33, 46, 135].
The contribution of neuropathology
Post-mortem studies including rigorous neuropathological investigation in clinically well-documented autopsy cases, although difficult to perform, are crucial to elucidate the role of cerebrovascular lesions in late-life affective disorders [118]. Thomas and colleagues have performed pioneer work in the neuropathological exploration of “vascular depression hypothesis” with conflicting results. Although deep white matter hyperintensities (DWMH) were more frequently associated with ischemia in depressed patients, mainly when located in the dorsolateral prefrontal cortex [134, 136] and patients with depression presented an increased frequency of cerebrovascular atheromatous lesions, depression was not associated with small vascular or with microvascular disease (Figs. 1, 2) [132, 134]. To investigate this question further, we have performed a clinico-neuropathological exploration in the post-mortem brains of 38 patients with LOD and 29 control subjects [107]. Our results complemented those obtained by Thomas et al. [131] by confirming, in a more extensive analysis that included both more cortical regions and a separate analysis of each type of small microvascular and microvascular lesions, the same absence of association between cerebrovascular pathology and LOD, even in the subgroup of patients fulfilling the criteria for vascular depression. Moreover, in this same study, neither deep white matter nor periventricular demyelination were associated with LOD. These results seem to contradict the vascular depression hypothesis by indicating that the chronic burden of small vascular and microvascular lesions is not a major determinant of LOD. A few months ago, Tsopelas and collaborators reported the largest autopsy series of elderly individuals with late-life depression from the Medical Research Council Cognitive Function and Ageing Study [140]. A total of 153 community-based participants (36 with late-life depression) were autopsied. Here also, no relationship was found between cerebrovascular pathology such as hemorrhages, infarcts larger than 10 mm, lacunes and small vessel disease, and depression [108]. A possible interpretation for this discrepancy is that the burden of subcortical lacunes may constitute a neuroanatomical substrate for both cognitive decline and affective dysregulation in old age but that their contribution to the development of depression may be relevant solely in the presence of a “second hit” such as an episode of acute brain compromise (as in PSD) or the accumulation of age-related neurodegenerative changes (as in mixed cases). Alternatively, the absence of a clear structural marker for LOD may reflect the predominant role of psychosocial determinants. In fact, several recent studies have highlighted the role of clinical and psychological determinants of LOD, namely the impact of the burden of medical comorbidities [35, 36, 86, 105], the presence and type of treatment for depression [19], the degree of social support [61, 84, 117, 138], the existence of functional disability [48, 81], and the psychological profile and psychiatric status of the patient [9, 29, 35, 84]. Interestingly, a recent review by Weber et al. [143] concludes that while more biologically determined risk factors for depression, such as gender or family history, seem to predict mainly short-term changes in mood regulation, personality characteristics are more closely related to the long-term evolution and treatment of depressive episodes.

Representative examples of microvascular lesions in brain aging. Slightly asymmetric deep white matter demyelination (a arrows), multiple cortical microinfacts (b), focal cortical gliosis (c) and subcortical gliosis (d). a Luxol-van Gieson staining; b–d Globus silver-impregnation. Scale bar b 800 mm, c 200 mm, d 400 mm
The neurotoxic hypothesis of late-life depression
Structural neuroimaging
The main piece of evidence supporting this scenario is related to the volumetric loss in hippocampus observed in late-life depression. Whether or not, this finding is related to the recurrence of early-onset depressive illness or the development of LOD remains, however, highly controversial. In fact, a loss of hippocampal volume bilaterally has been reported in VBM analyses of LOD cases unlike EOD and healthy elderly controls [68, 82]. This was further confirmed by another study that found greater hippocampal volume reductions in the subiculum and the lateral-posterior aspects of the CA1 in LOD compared to controls and EOD [13]. The origin of this finding is unclear. Does small hippocampal size render a person more vulnerable to develop depression or is it a result of the disease? The duration of illness [32, 91] as well as poor treatment outcome and increased risk of relapse [49, 87] are all associated with hippocampal volume reductions and may thus partly explain the association between this MRI variable and late-life depression. However, a recently published 10-year prospective study of an elderly population failed to establish the relationship between smaller hippocampal size at baseline and subsequent development of LOD [42]. Other VBM analyses of elderly patients with depression revealed volume reductions in the right frontal, orbitofrontal and anterior cingulate cortices left temporal lobe and caudate nucleus compared to both control subjects and EOD patients [8, 10, 25, 43, 44, 55].
Early MRI contributions have also reported decreased hippocampal volumes in middle-aged and elderly patients suffering from EOD [114]. Reduced hippocampal volume, mainly in the left side, was also reported later on in unmedicated remitted patients with major depression [94], drug-naïve depressed outpatients [110], young patients who relapse in a 2-year follow-up [77], as well as in male patients with a first episode of major depression [78]. Despite the impressive variability of the experimental data, a recent meta-analysis of 32 MRI studies concluded that hippocampal volume loss is mainly present in patients with a duration of illness longer than 2 years and more than one disease episode [91]. Previous comparisons between early-onset and late-onset elderly cases led to discrepant data. Unlike the data reported by Janssen and collaborators [68], we found no evidence supporting hippocampal volume loss in early-onset cases In a recent region of interest and VBM longitudinal study [41, 144]. In the community based SMART Medea study, early-onset was associated with smaller hippocampal volume, whereas late-onset cases had small entorhinal cortex volume [52].
Taking into account both the molecular and cellular effects of chronic stress and the possible neuroprotective impact of antidepressant treatment on hippocampus, a recent review postulates that chronic depression may critically affect hippocampus and even be a risk factor for Alzheimer disease [87]. Similarly, de Leeuw and collaborators [40] have reported an association between increased subcortical WMLs shown to be increased in patients with EOD as compared to control subjects [56, 64, 79] and decreased hippocampal volume in patients with probable Alzheimer’s disease. The authors hypothesized that WMLs affecting cortico-subcortical tracts linking prefrontal and limbic areas might disrupt hippocampal function and structure and may be associated with depressive symptoms. Interestingly, the results of a recent correlation of MRI-assessed hippocampal volume and cognitive performance in a large series of patients with CADASIL (a hereditary disorder that models pure small vessel disease [95]), confirmed the links between vascular burden, hippocampal atrophy and cognitive impairment in the absence of neurodegenerative process.
Lessons from neuropathology
Only rare studies attempted to explore the association between Alzheimer’s disease pathology as well as hippocampal neuronal loss and late-life depression. It seems to be a general consensus against an association between previously ascertained depression and Alzheimer’s disease pathology in old age. For instance, in a sample of 139 priests and nuns followed up to 4 years, depressive symptoms were not associated with plaque and tangle burden [146]. Similar observations were made by Hendricksen and coworkers [62] and Thomas and coworkers [131]. These observations were recently confirmed by Tsopelas et al. [140] in the largest autopsy series of non-demented elders with long-lasting depression. However, these authors still found neuronal loss in hippocampus supporting the idea of a direct effect of depression on hippocampal volumes. Surprisingly, they also reported an association between Lewy body densities in the brainstem nuclei and late-life depression in some rare cases with probable raphe pathology.
Conclusion and future perspectives
Starting from the viewpoint of three conceptually distinct models of depressive illness in the elderly, this review reveals the marked difficulty to analyze the interaction between psychosocial determinants and biological vulnerability over time. Although still too rare, the autopsy studies in this complex field sometimes confirm and in other challenge the relevance of MRI findings. In respect to post-stroke depression, the classical paradigm of acute mood disorder consecutive to well identified brain damage, both MRI and autopsy studies do not support the idea of a simple association between stroke location and mood disorder. Going beyond structural imaging, the neuropathological analysis in PSD cases stresses, however, the deleterious impact of small macrovascular burden on affective regulation. From this point of view, a purely traumatic model based on the abrupt change of brain status in PSD is not pertinent and should be revised. In contrast to PSD, LOD was not a priori defined as the consequence of a biological event. Attempting to establish a neurobiological origin, the introduction of the clinico-radiological concept of vascular depression was based on the frequently repeated, but not yet demonstrated assumption that the disruption of subcortico-frontal circuits is a key etiologic factor for the development of late-life mood disorders. However, neuropathological data challenged first the relationship between cerebrovascular pathology and LOD. These observations parallel the claims of some groups that questioned the clinical validity of the vascular depression hypothesis by highlighting the important role of psychosocial and personality factors in this type of depression. For example, a recent study by Canuto et al. [28] pointed to the role of neurocognitive and personality dimensions in euthymic patients with mood disorders in late life. Last but not least, despite the MRI evidence in favor of a possibly causal link between recurrent depression and neurodegeneration in old age, recent neuropathological data show that EOD is not a risk factor for AD pathology. However, they also provide experimental evidence in favor of the neurotoxic theory of depression by showing that AD pathology-unrelated neuronal loss occurs in the hippocampus of chronically depressed patients. These three paradigms illustrate the complementarity of neuroradiological and neuropathological observations in this field.
Although useful to structure the exploration of such complex field, theoretical models are necessarily simplistic. When interpreting these data, one should keep in mind that the mechanisms underlying depression after stroke are by far more complex than the dichotomy between biological vulnerability and psychosocial factors. In fact, genomic signatures, neurotransmitter and neurotrophin signaling, hippocampal neurogenesis, cellular plasticity in the ischemic lesion, secondary degenerative changes, activation of the hypothalamo–pituitary–adrenal (HPA) axis and neuroinflammation are all involved in the pathogenetic cascade that precede the occurrence of depressive symptoms in this context. Future studies assessing the role of these additional players are clearly warranted to assess the relative weight of biological determinants of late-life depression.
References
Aben I, Verhey F (2006) Depression after a cerebrovascular accident. The importance of the integration of neurobiological and psychosocial pathogenic models. Panminerva Med 48:49–57
Aizenstein HJ, Andreescu C, Edelman KL, Cochran JL, Price J, Butters MA, Karp J, Patel M, Reynolds CF 3rd (2011) fMRI correlates of white matter hyperintensities in late-life depression. Am J Psychiatry 168:1075–1082
Alexopoulos GS, Kelly RE Jr (2009) Research advances in geriatric depression. World Psychiatry 8:140–149
Alexopoulos GS, Kiosses DN, Klimstra S, Kalayam B, Bruce ML (2002) Clinical presentation of the “depression-executive dysfunction syndrome” of late life. Am J Geriatr Psychiatry 10:98–106
Alexopoulos GS, Meyers BS, Young RC, Campbell S, Silbersweig D, Charlson M (1997) ‘Vascular depression’ hypothesis. Arch Gen Psychiatry 54:915–922
Alexopoulos GS, Vrontou C, Kakuma T, Meyers BS, Young RC, Klausner E, Clarkin J (1996) Disability in geriatric depression. Am J Psychiatry 153:877–885
Almeida M, Lee R, Coccaro EF (2010) Cortisol responses to ipsapirone challenge correlate with aggression, while basal cortisol levels correlate with impulsivity, in personality disorder and healthy volunteer subjects. J Psychiatr Res 44:874–880
Almeida OP, Burton EJ, Ferrier N, McKeith IG, O’Brien JT (2003) Depression with late onset is associated with right frontal lobe atrophy. Psychol Med 33:675–681
Andreescu C, Butters M, Lenze EJ, Venkatraman VK, Nable M, Reynolds CF 3rd, Aizenstein HJ (2009) fMRI activation in late-life anxious depression: a potential biomarker. Int J Geriatr Psychiatry 24:820–828
Andreescu C, Butters MA, Begley A, Rajji T, Wu M, Meltzer CC, Reynolds CF 3rd, Aizenstein H (2008) Gray matter changes in late life depression—a structural MRI analysis. Neuropsychopharmacology 33:2566–2572
Astrom M, Adolfsson R, Asplund K (1993) Major depression in stroke patients. A 3-year longitudinal study. Stroke 24:976–982
Baldwin RC, Tomenson B (1995) Depression in later life. A comparison of symptoms and risk factors in early and late onset cases. Br J Psychiatry 167:649–652
Ballmaier M, Narr KL, Toga AW, Elderkin-Thompson V, Thompson PM, Hamilton L, Haroon E, Pham D, Heinz A, Kumar A (2008) Hippocampal morphology and distinguishing late-onset from early-onset elderly depression. Am J Psychiatry 165:229–237
Bearden CE, Hoffman KM, Cannon TD (2001) The neuropsychology and neuroanatomy of bipolar affective disorder: a critical review. Bipolar Disord 3:106–150 discussion 151–103
Beekman AT, Deeg DJ, Braam AW, Smit JH, Van Tilburg W (1997) Consequences of major and minor depression in later life: a study of disability, well-being and service utilization. Psychol Med 27:1397–1409
Benazzi F (2003) Unipolar depression with bipolar family history: links with the bipolar spectrum. Psychiatry Clin Neurosci 57:497–503
Bhogal SK, Teasell R, Foley N, Speechley M (2004) Lesion location and poststroke depression: systematic review of the methodological limitations in the literature. Stroke 35:794–802
Blazer DG (2003) Depression in late life: review and commentary. J Gerontol A Biol Sci Med Sci 58:249–265
Bogner HR, Cary MS, Bruce ML, Reynolds CF 3rd, Mulsant B, Ten Have T, Alexopoulos GS (2005) The role of medical comorbidity in outcome of major depression in primary care: the PROSPECT study. Am J Geriatr Psychiatry 13:861–868
Bozikas VP, Gold G, Kovari E, Herrmann F, Karavatos A, Giannakopoulos P, Bouras C (2005) Pathological correlates of poststroke depression in elderly patients. Am J Geriatr Psychiatry 13:166–169
Braffman BH, Zimmerman RA, Trojanowski JQ, Gonatas NK, Hickey WF, Schlaepfer WW (1988) Brain MR: pathologic correlation with gross and histopathology. 2. Hyperintense white-matter foci in the elderly. AJR Am J Roentgenol 151:559–566
Brodaty H, Luscombe G, Anstey KJ, Cramsie J, Andrews G, Peisah C (2003) Neuropsychological performance and dementia in depressed patients after 25-year follow-up: a controlled study. Psychol Med 33:1263–1275
Brodaty H, Luscombe G, Parker G, Wilhelm K, Hickie I, Austin MP, Mitchell P (2001) Early and late onset depression in old age: different aetiologies, same phenomenology. J Affect Disord 66:225–236
Brodaty H, Withall A, Altendorf A, Sachdev PS (2007) Rates of depression at 3 and 15 months poststroke and their relationship with cognitive decline: the Sydney Stroke Study. Am J Geriatr Psychiatry 15:477–486
Butters MA, Aizenstein HJ, Hayashi KM, Meltzer CC, Seaman J, Reynolds CF 3rd, Toga AW, Thompson PM, Becker JT (2009) Three-dimensional surface mapping of the caudate nucleus in late-life depression. Am J Geriatr Psychiatry 17:4–12
Camus V, de Mendonca Lima CA, Gaillard M, Simeone I, Wertheimer J (1997) Are personality disorders more frequent in early onset geriatric depression? J Affect Disord 46:297–302
Camus V, Kraehenbuhl H, Preisig M, Bula CJ, Waeber G (2004) Geriatric depression and vascular diseases: what are the links? J Affect Disord 81:1–16
Canuto A, Giannakopoulos P, Moy G, Rubio MM, Ebbing K, Meiler-Mititelu C, Herrmann FR, Gold G, Delaloye C, Weber K (2010) Neurocognitive deficits and personality traits among euthymic patients with mood disorders in late life. J Neurol Sci 299:24–29
Carney J, Corna L, Veldhuizen S (2009) Co-morbid depression and anxiety in later life: patterns of association, subjective well-being and impairment. Am J Geriatr Psychiatry 16:201–208
Carson AJ, MacHale S, Allen K, Lawrie SM, Dennis M, House A, Sharpe M (2000) Depression after stroke and lesion location: a systematic review. Lancet 356:122–126
Casanova MF, Starkstein SE, Jellinger KA (2011) Clinicopathological correlates of behavioral and psychological symptoms of dementia. Acta Neuropathol 122:117–135
Cheng YQ, Xu J, Chai P, Li HJ, Luo CR, Yang T, Li L, Shan BC, Xu XF, Xu L (2010) Brain volume alteration and the correlations with the clinical characteristics in drug-naive first-episode MDD patients: a voxel-based morphometry study. Neurosci Lett 480:30–34
Chimowitz MI, Estes ML, Furlan AJ, Awad IA (1992) Further observations on the pathology of subcortical lesions identified on magnetic resonance imaging. Arch Neurol 49:747–752
Colloby SJ, Firbank MJ, Thomas AJ, Vasudev A, Parry SW, O’Brien JT (2011) White matter changes in late-life depression: a diffusion tensor imaging study. J Affect Disord 135:216–220
Cui X, Lyness JM, Tang W, Tu X, Conwell Y (2008) Outcomes and predictors of late-life depression trajectories in older primary care patients. Am J Geriatr Psychiatry 16:406–415
Cui X, Lyness JM, Tu X, King DA, Caine ED (2007) Does depression precede or follow executive dysfunction? Outcomes in older primary care patients. Am J Psychiatry 164:1221–1228
Cullen KR, Klimes-Dougan B, Muetzel R, Mueller BA, Camchong J, Houri A, Kurma S, Lim KO (2010) Altered white matter microstructure in adolescents with major depression: a preliminary study. J Am Acad Child Adolesc Psychiatry 49(173–183):e171
Cumming TB, Churilov L, Skoog I, Blomstrand C, Linden T (2010) Little evidence for different phenomenology in poststroke depression. Acta Psychiatr Scand 121:424–430
Dalby RB, Chakravarty MM, Ahdidan J, Sorensen L, Frandsen J, Jonsdottir KY, Tehrani E, Rosenberg R, Ostergaard L, Videbech P (2010) Localization of white-matter lesions and effect of vascular risk factors in late-onset major depression. Psychol Med 40:1389–1399
de Leeuw FE, Barkhof F, Scheltens P (2004) White matter lesions and hippocampal atrophy in Alzheimer’s disease. Neurology 62:310–312
Delaloye C, Moy G, de Bilbao F, Baudois S, Weber K, Hofer F, Ragno Paquier C, Donati A, Canuto A, Giardini U, von Gunten A, Stancu RI, Lazeyras F, Millet P, Scheltens P, Giannakopoulos P, Gold G (2010) Neuroanatomical and neuropsychological features of elderly euthymic depressed patients with early- and late-onset. J Neurol Sci 299:19–23
den Heijer T, Tiemeier H, Luijendijk HJ, van der Lijn F, Koudstaal PJ, Hofman A, Breteler MM (2011) A study of the bidirectional association between hippocampal volume on magnetic resonance imaging and depression in the elderly. Biol Psychiatry 70:191–197
Dotson VM, Resnick SM, Zonderman AB (2008) Differential association of concurrent, baseline, and average depressive symptoms with cognitive decline in older adults. Am J Geriatr Psychiatry 16:318–330
Egger K, Schocke M, Weiss E, Auffinger S, Esterhammer R, Goebel G, Walch T, Mechtcheriakov S, Marksteiner J (2008) Pattern of brain atrophy in elderly patients with depression revealed by voxel-based morphometry. Psychiatry Res 164:237–244
Fang J, Cheng Q (2009) Etiological mechanisms of post-stroke depression: a review. Neurol Res 31:904–909
Fazekas F, Kleinert R, Offenbacher H, Schmidt R, Kleinert G, Payer F, Radner H, Lechner H (1993) Pathologic correlates of incidental MRI white matter signal hyperintensities. Neurology 43:1683–1689
Folstein MF, Maiberger R, McHugh PR (1977) Mood disorder as a specific complication of stroke. J Neurol Neurosurg Psychiatry 40:1018–1020
Friedman B, Lyness JM, Delavan RL, Chunyu L, Barker WH (2008) Major depression and disability in older primary care patients with heart failure. J Geriatr Psychiatry Neurol 21:111–122
Frodl T, Jager M, Smajstrlova I, Born C, Bottlender R, Palladino T, Reiser M, Moller HJ, Meisenzahl EM (2008) Effect of hippocampal and amygdala volumes on clinical outcomes in major depression: a 3-year prospective magnetic resonance imaging study. J Psychiatry Neurosci 33:423–430
Gainotti G, Azzoni A, Marra C (1999) Frequency, phenomenology and anatomical-clinical correlates of major post-stroke depression. Br J Psychiatry 175:163–167
Gaupp RE (1905) Depressive states in older age (in German). Medizinische Wochenschrift 52:1531–1537
Gerritsen L, Tendolkar I, Franke B, Vasquez AA, Kooijman S, Buitelaar J, Fernandez G, Rijpkema M (2012) BDNF Val66Met genotype modulates the effect of childhood adversity on subgenual anterior cingulate cortex volume in healthy subjects. Mol Psychiatry 17:597–603
Gold G, Kövari E, Herrmann FR, Canuto A, Hof PR, Michel JP, Bouras C, Giannakopoulos P (2005) Cognitive consequences of thalamic, basal ganglia, and deep white matter lacunes in brain aging and dementia. Stroke 36:1184–1188
Gotlib IH, Joormann J, Minor KL, Hallmayer J (2008) HPA axis reactivity: a mechanism underlying the associations among 5-HTTLPR, stress, and depression. Biol Psychiatry 63:847–851
Greenwald BS, Kramer-Ginsberg E, Krishnan KR, Ashtari M, Auerbach C, Patel M (1998) Neuroanatomic localization of magnetic resonance imaging signal hyperintensities in geriatric depression. Stroke J Cerebral Circ 29:613–617
Greenwald BS, Kramer-Ginsberg E, Krishnan RR, Ashtari M, Aupperle PM, Patel M (1996) MRI signal hyperintensities in geriatric depression. Am J Psychiatry 153:1212–1215
Hackett ML, Anderson CS (2005) Predictors of depression after stroke: a systematic review of observational studies. Stroke 36:2296–2301
Hackett ML, Yapa C, Parag V, Anderson CS (2005) Frequency of depression after stroke: a systematic review of observational studies. Stroke 36:1330–1340
Hama S, Yamashita H, Shigenobu M, Watanabe A, Kurisu K, Yamawaki S, Kitaoka T (2007) Post-stroke affective or apathetic depression and lesion location: left frontal lobe and bilateral basal ganglia. Eur Arch Psychiatry Clin Neurosci 257:149–152
Hama S, Yamashita H, Yamawaki S, Kurisu K (2011) Post-stroke depression and apathy: interactions between functional recovery, lesion location, and emotional response. Psychogeriatrics 11:68–76
Harris T, Cook DG, Victor C, DeWilde S, Beighton C (2006) Onset and persistence of depression in older people—results from a 2-year community follow-up study. Age Ageing 35:25–32
Hendricksen M, Thomas AJ, Ferrier IN, Ince P, O’Brien JT (2004) Neuropathological study of the dorsal raphe nuclei in late-life depression and Alzheimer’s disease with and without depression. Am J Psychiatry 161:1096–1102
Herrmann LL, Goodwin GM, Ebmeier KP (2007) The cognitive neuropsychology of depression in the elderly. Psychol Med 37:1693–1702
Herrmann LL, Le Masurier M, Ebmeier KP (2008) White matter hyperintensities in late life depression: a systematic review. J Neurol Neurosurg Psychiatry 79:619–624
Huang H, Fan X, Williamson DE, Rao U (2011) White matter changes in healthy adolescents at familial risk for unipolar depression: a diffusion tensor imaging study. Neuropsychopharmacology 36:684–691
Jabbi M, Korf J, Kema IP, Hartman C, van der Pompe G, Minderaa RB, Ormel J, den Boer JA (2007) Convergent genetic modulation of the endocrine stress response involves polymorphic variations of 5-HTT, COMT and MAOA. Mol Psychiatry 12:483–490
Jacoby RJ, Levy R, Bird JM (1981) Computed tomography and the outcome of affective disorder: a follow-up study of elderly patients. Br J Psychiatry 139:288–292
Janssen J, Hulshoff Pol HE, De Leeuw FE, Schnack HG, Lampe IK, Kok RM, Kahn RS, Heeren TJ (2007) Hippocampal volume and subcortical white matter lesions in late life depression: comparison of early and late onset depression. J Neurol Neurosurg Psychiatry 78:638–640
Johnson JL, Minarik PA, Nystrom KV, Bautista C, Gorman MJ (2006) Poststroke depression incidence and risk factors: an integrative literature review. J Neurosci Nurs 38:316–327
Johnson L, Andersson-Lundman G, Aberg-Wistedt A, Mathe AA (2000) Age of onset in affective disorder: its correlation with hereditary and psychosocial factors. J Affect Disord 59:139–148
Katon WJ, Lin E, Russo J, Unutzer J (2003) Increased medical costs of a population-based sample of depressed elderly patients. Arch Gen Psychiatry 60:897–903
Kendler KS, Fiske A, Gardner CO, Gatz M (2009) Delineation of two genetic pathways to major depression. Biol Psychiatry 65:808–811
Kohen R, Cain KC, Buzaitis A, Johnson V, Becker KJ, Teri L, Tirschwell DL, Veith RC, Mitchell PH (2011) Response to psychosocial treatment in poststroke depression is associated with serotonin transporter polymorphisms. Stroke 42:2068–2070
Kohler S, Thomas AJ, Barnett NA, O’Brien JT (2010) The pattern and course of cognitive impairment in late-life depression. Psychol Med 40:591–602
Krishnan KR, Taylor WD, McQuoid DR, MacFall JR, Payne ME, Provenzale JM, Steffens DC (2004) Clinical characteristics of magnetic resonance imaging-defined subcortical ischemic depression. Biol Psychiatry 55:390–397
Krishnan MS, O’Brien JT, Firbank MJ, Pantoni L, Carlucci G, Erkinjuntti T, Wallin A, Wahlund LO, Scheltens P, van Straaten EC, Inzitari D (2006) Relationship between periventricular and deep white matter lesions and depressive symptoms in older people. The LADIS Study. Int J Geriatr Psychiatry 21:983–989
Kronmuller KT, Pantel J, Kohler S, Victor D, Giesel F, Magnotta VA, Mundt C, Essig M, Schroder J (2008) Hippocampal volume and 2-year outcome in depression. Br J Psychiatry 192:472–473
Kronmuller KT, Schroder J, Kohler S, Gotz B, Victor D, Unger J, Giesel F, Magnotta V, Mundt C, Essig M, Pantel J (2009) Hippocampal volume in first episode and recurrent depression. Psychiatry Res 174:62–66
Kumar A, Bilker W, Jin Z, Udupa J, Gottlieb G (1999) Age of onset of depression and quantitative neuroanatomic measures: absence of specific correlates. Psychiatry Res 91:101–110
Li L, Ma N, Li Z, Tan L, Liu J, Gong G, Shu N, He Z, Jiang T, Xu L (2007) Prefrontal white matter abnormalities in young adult with major depressive disorder: a diffusion tensor imaging study. Brain Res 1168:124–128
Licht-Strunk E, Bremmer MA, van Marwijk HW, Deeg DJ, Hoogendijk WJ, de Haan M, van Tilburg W, Beekman AT (2004) Depression in older persons with versus without vascular disease in the open population: similar depressive symptom patterns, more disability. J Affect Disord 83:155–160
Lloyd AJ, Ferrier IN, Barber R, Gholkar A, Young AH, O’Brien JT (2004) Hippocampal volume change in depression: late- and early-onset illness compared. Br J Psychiatry 184:488–495
Loubinoux I, Kronenberg G, Endres M, Schumann-Bard P, Freret T, Filipkowski RK, Kaczmarek L, Popa-Wagner A (2012) Poststroke depression: mechanisms, translation and therapy. J Cell Mol Med doi. doi:10.1111/j.1582-4934.2012.01555.x
Lyness JM, Chapman BP, McGriff J, Drayer R, Duberstein PR (2009) One-year outcomes of minor and subsyndromal depression in older primary care patients. Int Psychogeriatr 21:60–68
Lyness JM, Heo M, Datto CJ, Ten Have TR, Katz IR, Drayer R, Reynolds CF 3rd, Alexopoulos GS, Bruce ML (2006) Outcomes of minor and subsyndromal depression among elderly patients in primary care settings. Ann Intern Med 144:496–504
Lyness JM, Niculescu A, Tu X, Reynolds CF 3rd, Caine ED (2006) The relationship of medical comorbidity and depression in older, primary care patients. Psychosomatics 47:435–439
MacQueen G, Frodl T (2011) The hippocampus in major depression: evidence for the convergence of the bench and bedside in psychiatric research? Mol Psychiatry 16:252–264
Marchand WR, Yurgelun-Todd D (2010) Striatal structure and function in mood disorders: a comprehensive review. Bipolar Disord 12:764–785
Mast BT, Vedrody S (2006) Poststroke depression: a biopsychosocial approach. Curr Psychiatry Rep 8:25–33
McDougall F, Brayne C (2007) Systematic review of the depressive symptoms associated with vascular conditions. J Affect Disord 104:25–35
McKinnon MC, Yucel K, Nazarov A, MacQueen GM (2009) A meta-analysis examining clinical predictors of hippocampal volume in patients with major depressive disorder. J Psychiatry Neurosci 34:41–54
Naarding P, Veereschild M, Bremmer M, Deeg D, Beekman AT (2009) The symptom profile of vascular depression. Int J Geriatr Psychiatry 24:965–969
Nebes RD, Pollock BG, Houck PR, Butters MA, Mulsant BH, Zmuda MD, Reynolds CF 3rd (2003) Persistence of cognitive impairment in geriatric patients following antidepressant treatment: a randomized, double-blind clinical trial with nortriptyline and paroxetine. J Psychiatr Res 37:99–108
Neumeister A, Wood S, Bonne O, Nugent AC, Luckenbaugh DA, Young T, Bain EE, Charney DS, Drevets WC (2005) Reduced hippocampal volume in unmedicated, remitted patients with major depression versus control subjects. Biol Psychiatry 57:935–937
O’Sullivan M, Ngo E, Viswanathan A, Jouvent E, Gschwendtner A, Saemann PG, Duering M, Pachai C, Bousser MG, Chabriat H, Dichgans M (2009) Hippocampal volume is an independent predictor of cognitive performance in CADASIL. Neurobiol Aging 30:890–897
Onoda K, Kuroda Y, Yamamoto Y, Abe S, Oguro H, Nagai A, Bokura H, Yamaguchi S (2011) Post-stroke apathy and hypoperfusion in basal ganglia: SPECT study. Cerebrovasc Dis 31:6–11
Ortiz A, Bradler K, Slaney C, Garnham J, Ruzickova M, O’Donovan C, Hajek T, Alda M (2011) An admixture analysis of the age at index episodes in bipolar disorder. Psychiatry Res 188:34–39
Paradiso S, Ohkubo T, Robinson RG (1997) Vegetative and psychological symptoms associated with depressed mood over the first two years after stroke. Int J Psychiatry Med 27:137–157
Paranthaman R, Burns AS, Cruickshank JK, Jackson A, Scott ML, Baldwin RC (2012) Age at onset and vascular pathology in late-life depression. Am J Geriatr Psychiatry 20:524–532
Pav M, Kovaru H, Fiserova A, Havrdova E, Lisa V (2008) Neurobiological aspects of depressive disorder and antidepressant treatment: role of glia. Physiol Res 57:151–164
Raison CL, Capuron L, Miller AH (2006) Cytokines sing the blues: inflammation and the pathogenesis of depression. Trends Immunol 27:24–31
Robinson RG, Shoemaker WJ, Schlumpf M, Valk T, Bloom FE (1975) Effect of experimental cerebral infarction in rat brain on catecholamines and behaviour. Nature 255:332–334
Robinson RG, Spalletta G (2010) Poststroke depression: a review. Can J Psychiatry 55:341–349
Robinson RG, Starr LB, Lipsey JR, Rao K, Price TR (1984) A two-year longitudinal study of post-stroke mood disorders: dynamic changes in associated variables over the first six months of follow-up. Stroke 15:510–517
Sanders ML, Lyness JM, Eberly S, King DA, Caine ED (2006) Cerebrovascular risk factors, executive dysfunction, and depression in older primary care patients. Am J Geriatr Psychiatry 14:145–152
Santos M, Gold G, Kövari E, Herrmann FR, Bozikas VP, Bouras C, Giannakopoulos P (2009) Differential impact of lacunes and microvascular lesions on poststroke depression. Stroke 40:3557–3562
Santos M, Gold G, Kovari E, Herrmann FR, Hof PR, Bouras C, Giannakopoulos P (2010) Neuropathological analysis of lacunes and microvascular lesions in late-onset depression. Neuropathol Appl Neurobiol 36:661–672
Santos M, Kövari E, Gold G, Bozikas VP, Hof PR, Bouras C, Giannakopoulos P (2009) The neuroanatomical model of post-stroke depression: towards a change of focus? J Neurol Sci 283:158–162
Santos M, Kovari E, Hof PR, Gold G, Bouras C, Giannakopoulos P (2009) The impact of vascular burden on late-life depression. Brain Res Rev 62:19–32
Saylam C, Ucerler H, Kitis O, Ozand E, Gonul AS (2006) Reduced hippocampal volume in drug-free depressed patients. Surg Radiol Anat 28:82–87
Schmidt R, Schmidt H, Haybaeck J, Loitfelder M, Weis S, Cavalieri M, Seiler S, Enzinger C, Ropele S, Erkinjuntti T, Pantoni L, Scheltens P, Fazekas F, Jellinger K (2011) Heterogeneity in age-related white matter changes. Acta Neuropathol 122:171–185
Schwenk TL (2002) Diagnosis of late life depression: the view from primary care. Biol Psychiatry 52:157–163
Sexton CE, McDermott L, Kalu UG, Herrmann LL, Bradley KM, Allan CL, Le Masurier M, Mackay CE, Ebmeier KP (2012) Exploring the pattern and neural correlates of neuropsychological impairment in late-life depression. Psychol Med 42:1195–1202
Sheline YI (2003) Neuroimaging studies of mood disorder effects on the brain. Biol Psychiatry 54:338–352
Shimony JS, Sheline YI, D’Angelo G, Epstein AA, Benzinger TL, Mintun MA, McKinstry RC, Snyder AZ (2009) Diffuse microstructural abnormalities of normal-appearing white matter in late life depression: a diffusion tensor imaging study. Biol Psychiatry 66:245–252
Simon NM, Smoller JW, McNamara KL, Maser RS, Zalta AK, Pollack MH, Nierenberg AA, Fava M, Wong KK (2006) Telomere shortening and mood disorders: preliminary support for a chronic stress model of accelerated aging. Biol Psychiatry 60:432–435
Smit F, Ederveen A, Cuijpers P, Deeg D, Beekman A (2006) Opportunities for cost-effective prevention of late-life depression: an epidemiological approach. Arch Gen Psychiatry 63:290–296
Smith PJ, Blumenthal JA, Babyak MA, Doraiswamy PM, Hinderliter A, Hoffman BM, Waugh R, Sherwood A (2009) Intima-media thickness and age of first depressive episode. Biol Psychol 80:361–364
Sneed JR, Rindskopf D, Steffens DC, Krishnan KR, Roose SP (2008) The vascular depression subtype: evidence of internal validity. Biol Psychiatry 64:491–497
Starkstein SE, Fedoroff JP, Price TR, Leiguarda R, Robinson RG (1993) Apathy following cerebrovascular lesions. Stroke 24:1625–1630
Steffens DC, Bosworth HB, Provenzale JM, MacFall JR (2002) Subcortical white matter lesions and functional impairment in geriatric depression. Depress Anxiety 15:23–28
Steffens DC, Krishnan KR, Crump C, Burke GL (2002) Cerebrovascular disease and evolution of depressive symptoms in the cardiovascular health study. Stroke 33:1636–1644
Steffens DC, Taylor WD, Denny KL, Bergman SR, Wang L (2011) Structural integrity of the uncinate fasciculus and resting state functional connectivity of the ventral prefrontal cortex in late life depression. PLoS One 6:e22697
Takahashi K, Oshima A, Ida I, Kumano H, Yuuki N, Fukuda M, Amanuma M, Endo K, Mikuni M (2008) Relationship between age at onset and magnetic resonance image-defined hyperintensities in mood disorders. J Psychiatr Res 42:443–450
Tang WK, Chen YK, Lu JY, Chu WC, Mok VC, Ungvari GS, Wong KS (2011) Cerebral microbleeds and symptom severity of post-stroke depression: a magnetic resonance imaging study. J Affect Disord 129:354–358
Tang WK, Lu JY, Chen YK, Chu WC, Mok V, Ungvari GS, Wong KS (2011) Association of frontal subcortical circuits infarcts in poststroke depression: a magnetic resonance imaging study of 591 Chinese patients with ischemic stroke. J Geriatr Psychiatry Neurol 24:44–49
Taylor WD, MacFall JR, Payne ME, McQuoid DR, Steffens DC, Provenzale JM, Krishnan RR (2005) Greater MRI lesion volumes in elderly depressed subjects than in control subjects. Psychiatry Res 139:1–7
Taylor WD, Steffens DC, Krishnan KR (2006) Psychiatric disease in the twenty-first century: the case for subcortical ischemic depression. Biol Psychiatry 60:1299–1303
Teodorczuk A, O’Brien JT, Firbank MJ, Pantoni L, Poggesi A, Erkinjuntti T, Wallin A, Wahlund LO, Gouw A, Waldemar G, Schmidt R, Ferro JM, Chabriat H, Bazner H, Inzitari D (2007) White matter changes and late-life depressive symptoms: longitudinal study. Br J Psychiatry 191:212–217
Tham MW, Woon PS, Sum MY, Lee TS, Sim K (2011) White matter abnormalities in major depression: evidence from post-mortem, neuroimaging and genetic studies. J Affect Disord 132:26–36
Thomas AJ, Ferrier IN, Kalaria RN, Perry RH, Brown A, O’Brien JT (2001) A neuropathological study of vascular factors in late-life depression. J Neurol Neurosurg Psychiatry 70:83–87
Thomas AJ, Ferrier IN, Kalaria RN, Perry RH, Brown A, O’Brien JT (2001) A neuropathological study of vascular factors in late-life depression. J Neurol Neurosurg Psychiatry 70:83–87
Thomas AJ, Kalaria RN, O’Brien JT (2004) Depression and vascular disease: what is the relationship? J Affect Disord 79:81–95
Thomas AJ, O’Brien JT, Davis S, Ballard C, Barber R, Kalaria RN, Perry RH (2002) Ischemic basis for deep white matter hyperintensities in major depression: a neuropathological study. Arch Gen Psychiatry 59:785–792
Thomas AJ, Perry R, Barber R, Kalaria RN, O’Brien JT (2002) Pathologies and pathological mechanisms for white matter hyperintensities in depression. Ann N Y Acad Sci 977:333–339
Thomas AJ, Perry R, Kalaria RN, Oakley A, McMeekin W, O’Brien JT (2003) Neuropathological evidence for ischemia in the white matter of the dorsolateral prefrontal cortex in late-life depression. Int J Geriatr Psychiatry 18:7–13
Thuile J, Even C, Guelfi JD (2007) Validity of vascular depression as a specific diagnostic: a review. Encephale 33:39–48
Travis LA, Lyness JM, Shields CG, King DA, Cox C (2004) Social support, depression, and functional disability in older adult primary-care patients. Am J Geriatr Psychiatry 12:265–271
Trexler LE, Fordyce DJ (2000) Psychological perspectives on rehabiliation: contemporary assessment and intervention strategies. In: Braddom RL (ed) Physical medicine and rehabilitation, 2nd edn. W. B. Saunders, Philadelphia, pp 75–92
Tsopelas C, Stewart R, Savva GM, Brayne C, Ince P, Thomas A, Matthews FE (2011) Neuropathological correlates of late-life depression in older people. The Br J Psychiatry 198:109–114
Vataja R, Leppavuori A, Pohjasvaara T, Mantyla R, Aronen HJ, Salonen O, Kaste M, Erkinjuntti T (2004) Poststroke depression and lesion location revisited. J Neuropsychiatry Clin Neurosci 16:156–162
Videbech P, Ravnkilde B, Gammelgaard L, Egander A, Clemmensen K, Rasmussen NA, Gjedde A, Rosenberg R (2004) The Danish PET/depression project: performance on Stroop’s test linked to white matter lesions in the brain. Psychiatry Res 130:117–130
Weber K, Giannakopoulos P, Bacchetta JP, Quast S, Herrmann FR, Delaloye C, Ghisletta P, De Ribaupierre A, Canuto A (2011) Personality traits are associated with acute major depression across the age spectrum. Aging Ment Health 16:472–480
Weber K, Giannakopoulos P, Delaloye C, de Bilbao F, Moy G, Ebbing K, Moussa A, Herrmann FR, Gold G, Canuto A (2012) Personality traits, cognition and volumetric MRI changes in elderly patients with early-onset depression: a 2-year follow-up study. Psychiatry Res (in press)
WHO (2001) The World Health Report 2001. World Health Organization, Geneva
Wilson RS, Schneider JA, Bienias JL, Arnold SE, Evans DA, Bennett DA (2003) Depressive symptoms, clinical AD, and cortical plaques and tangles in older persons. Neurology 61:1102–1107
Wu JT, Wu HZ, Yan CG, Chen WX, Zhang HY, He Y, Yang HS (2011) Aging-related changes in the default mode network and its anti-correlated networks: a resting-state fMRI study. Neurosci Lett 504:62–67
Xekardaki A, Giannakopoulos P, Haller S (2011) White matter changes in bipolar disorder, Alzheimer disease, and mild cognitive impairment: new insights from DTI. J Aging Res 2011:286564
Xiong YY, Wong A, Mok VC, Tang WK, Lam WW, Kwok TC, Chu WC, Chan AY, Wong LK (2010) Frequency and predictors of proxy-confirmed post-stroke cognitive complaints in lacunar stroke patients without major depression. Int J Geriatr Psychiatry 26:1144–1151
Zhang T, Jing X, Zhao X, Wang C, Liu Z, Zhou Y, Wang Y (2012) A prospective cohort study of lesion location and its relation to post-stroke depression among Chinese patients. J Affect Disord 136:e83–e87
Acknowledgments
This work has been supported by an unrestricted grant of Fondation Vachoux (MS).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Xekardaki, A., Santos, M., Hof, P. et al. Neuropathological substrates and structural changes in late-life depression: the impact of vascular burden. Acta Neuropathol 124, 453–464 (2012). https://doi.org/10.1007/s00401-012-1021-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00401-012-1021-5