
Abstract
Purpose
The effect of caffeine to enhance fat utilisation as fuel for submaximal aerobic exercise is well established. However, it is unknown whether this effect is dose dependent. The aim of this study was to investigate the effect of 3 and 6 mg of caffeine per kg of body mass (mg/kg) on whole-body substrate oxidation during an incremental cycling exercise test.
Methods
In a double-blind, randomised, and counterbalanced experiment, 18 recreationally active males (maximal oxygen uptake [VO2max] = 56.7 ± 8.2 mL/kg/min) performed three experimental trials after ingesting either 3 mg/kg of caffeine, 6 mg/kg of caffeine or a placebo (cellulose). The trials consisted of an incremental exercise test on a cycle ergometer with 3-min stages at workloads from 30 to 80% of VO2max. Energy expenditure, fat oxidation rate, and carbohydrate oxidation rate were continuously measured by indirect calorimetry.
Results
During exercise, there was significant effect of substance (F = 7.969; P = 0.004) on fat oxidation rate. In comparison to the placebo, the rate of fat oxidation was higher with 3 mg/kg of caffeine at 30, 40, 50 and 70% of VO2max [all P < 0.050, effect sizes (ES) from 0.38 to 0.50] and with 6 mg/kg of caffeine at 30, 40, 50, 60 and 70% of VO2max (all P < 0.050, ES from 0.28 to 0.76). Both 3 mg/kg (0.40 ± 0.21 g/min, P = 0.021, ES = 0.57) and 6 mg/kg of caffeine (0.40 ± 0.17 g/min P = 0.001, ES = 0.60) increased the maximal rate of fat oxidation during exercise over the placebo (0.31 ± 0.15 g/min). None of the caffeine doses produced any significant effect on energy expenditure or heart rate during exercise, while both caffeine doses reduced perceived fatigue at 80% of VO2max (all P < 0.050, ES from 0.71 to 1.48).
Conclusion
The effect of caffeine to enhance fat oxidation during submaximal aerobic exercise is of similar magnitude with 3 and 6 mg of caffeine per kg of body mass. Thus, a dose of 3 mg of caffeine per kg of body mass would be sufficient to enhance fat utilisation as fuel during submaximal exercise.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Caffeine (1, 3, 7-trimethylxanthine) is a naturally occurring chemical compound found in plant constituents such as coffee and cocoa beans, tea leaves, guarana berries and the kola nut. The ingestion of caffeine via infusions of these plants/seeds, through manufactured caffeine-containing foodstuffs (e.g. cola drinks, energy drinks) and/or through dietary supplements has become a common practise for a high portion of the world population [1]. The reasons for the high consumption of caffeine are mainly associated with the wide spectrum of benefits associated with acute and chronic caffeine intake [2]. Among others, the enhancement of stamina and the lessening of physical and mental fatigue are the most commonly sought effects of caffeine intake [3]. Although the dose of caffeine ingested depends on age, an average of ~ 2.2 mg/kg of caffeine per day has been found as the caffeine intake in the population of the United States—the 90th percentile is 5.0 mg/kg/day- [4]. These data suggest that most of the benefits of caffeine intake can be obtained with a relatively low dose of caffeine.
The high consumption of caffeine in modern societies is also reflected in sports as caffeine has also become one of the most consumed substances [5] despite having no nutritional value. In the exercise and sports context, caffeine is primarily used to enhance physical performance since there is plenty of evidence confirming the ergogenic value of oral caffeine intake on a variety of individual and team sports [6,7,8,9,10,11,12]. Caffeine is habitually ingested by athletes in amounts larger than the ones found in the general population. Concretely, doses equivalent to 3–6 mg/kg are commonly recommended to enhance exercise and sports performance [13, 14]. Interestingly, literature on the potential dose–response effect of caffeine on exercise performance indicates that oral caffeine intake produces an ergogenic benefit of similar magnitude within the dose range of 3–9 mg/kg [15,16,17,18]. Doses below 3 mg/kg of caffeine habitually do not produce ergogenic benefits [19, 20], although this is now always the case in some exercise contexts [21].
Acute caffeine intake can also be used to enhance fat oxidation during exercise. This is because the acute intake of caffeine can enhance the use of fat as fuel for the working muscle—with a concomitant reduction in the use of carbohydrates-during aerobic exercise [22,23,24]. To obtain a benefit of caffeine on fat oxidation during aerobic exercise, exercise intensity must be submaximal as the ergogenic benefit of caffeine (i.e. increased exercise intensity) nullifies the effect of caffeine on fat oxidation [25]. The effect of caffeine to enhance fat oxidation during exercise has been found in doses ranging from 3 to 7 mg/kg [22, 26, 27]. A recent systematic review has summarised the findings of 19 studies published between 1978 and 2020 that investigated the effect of caffeine on fat oxidation during exercise [28]. In this systematic review, caffeine produced an overall effect on increasing fat oxidation during submaximal exercise, but this effect was dose dependent. Specifically, caffeine was not effective to enhance fat oxidation when the dose was ≤ 3 mg/kg while there was an increasing effect of caffeine on fat oxidation with doses of 3.1–5.9 and ≥ 6 mg/kg of caffeine. However, none of the included studies investigated more than one dose of caffeine within the same experiment. Therefore, the aim of this study was to investigate, by using a crossover design, the effect of 3 and 6 mg of caffeine per kg of body mass (mg/kg) on whole-body substrate oxidation during an incremental cycling exercise test. We hypothesised that both doses of caffeine would increase fat oxidation during exercise of low-to-moderate intensity but the effect of 6 mg/kg to enhance fat oxidation rate would be of higher magnitude than 3 mg/kg when compared to a placebo condition.
Materials and methods
Participants
Eighteen young, and recreationally active males volunteered to participate in this investigation. Participants were considered active because all of them exercised at least 60 min of exercise per day for at least 4 days per week for the 2 years prior to the investigation, although they practised different sport disciplines (road cycling, mountain biking, endurance running and triathlon). Participants’ age, morphological characteristics, and maximal values at the end of a maximal oxygen uptake (VO2max) test on a cycle ergometer are depicted in Table 1. An a priori sample size calculation indicated that at least 9 participants were required to obtain statistically significant differences between caffeine and placebo on fat oxidation during exercise of increasing intensity. The required sample size was calculated to obtain an effect size of 0.5 Cohen’s d units based on a previous study that reported increases of such magnitude in fat oxidation with 3 mg/kg of caffeine at 30–70% VO2max [23]. The sample size was calculated using the G*Power software (v.3.1.9.7, Germany) with a statistical power of 0.95, a two-tailed α level of 0.05, for an ANOVA of repeated measures, within factors. We recruited 18 participants to increase the likelihood of finding differences between 3 and 6 mg/kg of caffeine. The inclusion criteria for participants were: (a) regularly performing aerobic exercise training 1 h per day, at least 4 days per week, (b) age between 18 and 45 years and (d) low caffeine intake assessed by using a food frequency questionnaire as defined by Filip [29]. Exclusion criteria were: (a) smoking status, (b) using medications or any type of dietary supplementation in the month before testing, (c) allergy to caffeine and (d) cardiopulmonary or musculoskeletal diseases. Before the enrolment, all potential participants were fully informed about the experimental procedures and their potentially associated risks. Once inclusion/exclusion criteria were applied, all participants of the study provided oral and written informed consent. The study was approved by the Francisco de Vitoria University Research Ethics Committee (18-2020) and was conducted under the latest version of the Declaration of Helsinki.
Experimental design
A randomised, double-blind, and placebo-controlled design was used in this experimental investigation. Each participant completed three identical trials separated by at least 3 days to allow complete recovery and caffeine wash-out. In each trial, participants ingested either 3 mg of caffeine per kg of body mass (3 mg/kg), 6 mg of caffeine per kg of body mass (6 mg/kg) or 3 mg/kg of an inert substance as a placebo. The use of 3 and 6 mg/kg of caffeine was based on a previous systematic review which found that the intake of more than 3 mg/kg of caffeine is needed to enhance fat oxidation during exercise [28]. Both caffeine (HSN, Spain) and cellulose (Guinama, Spain) were 100% pure and were administered in an opaque and unidentifiable capsule. Upon arrival at the laboratory, participants ingested the capsule with 150 mL of tap water 60 min before the onset of the experimental trials while a researcher verified the ingestion. Subsequently, participants performed a cycling test of increasing intensity with 3-min stages (i.e. Fatmax test) and the workload at each stage was equivalent to 30–80% of VO2max. An alphanumeric code was assigned to each trial by an individual independent of the study to blind participants and experimenters to the substance being tested in each trial. Ambient temperature and humidity were controlled to avoid the effect of ambient temperature on fat oxidation during exercise [30]. Both, ambient temperature, and humidity were recorded at the beginning and the end of each trial (OH1001, OH Haus, Spain) they were 21.7 ± 0.9 ℃ and 41.5 ± 6.2%, respectively. All experimental trials were performed in the morning to avoid the influence of circadian rhythm on the effect of caffeine on fat oxidation [24].
Pre-experimental trials
One week before the first trial, participants were weighed and morphologically analysed by bioimpedance (InnerScan Dual, Tanita, Japan) to estimate body fat. Then, participants underwent a standardised warm-up that included 10 min at 50 W on a cycle ergometer (Ergoselect 4, Ergoline, Germany) and completed an incremental exercise test (25 W each 1 min) until volitional fatigue to determine VO2max, as previously described [31]. The test was finished when participants were unable to maintain a cadence > 50 rpm or when they abruptly stopped pedalling. During exercise, oxygen uptake (VO2) and carbon dioxide production (VCO2) were measured through a breath-by-breath gas analyser (Ergostik, Geratherm Respiratory, Germany) and the data were averaged each 15 s. VO2max was defined as the highest VO2 value obtained during the test. The VO2max was considered valid when participants rated their perceived exertion higher than 19 on the Borg scale, the VO2 difference between the last two consecutive loads was less than 0.15 L/min, the respiratory exchange ratio was higher than 1.10, and the heart rate was superior to 80% of the age-adjusted estimate of maximal heart rate [33]. To normalise exercise intensity in the experimental trials (workloads that elicited between 30 and 80% of participants’ VO2max), a regression analysis was performed for each subject for the relationship between workload (in W) and VO2 (L/min) obtained in this test. In this pre-experimental testing, participants fixed the saddle and handlebar position of the cycle ergometer and wore the same clothing that would be used in the trials. Within the week prior to the onset of the experiment, a second pre-experimental testing was carried out to familiarise participants with the experimental protocol. In this second pre-experimental trial, participants performed the incremental exercise test as in the experimental trials but without the intake of any substance.
Standardisations and experimental trials
Before and after each experimental trial, participants refrained from strenuous exercise and adopted a similar diet and fluid intake regimen. Participants were also required to avoid alcohol, caffeine, and other stimulants 24 h before each trial. Participants were requested to complete a 24-h dietary record on the day before the first trial and to follow the same dietary pattern during all visits. During experimental trials, participants come to the laboratory between 09.00 and 11:00 am) in a fasted state (at least 8 h after their last meal) and 2 h after ingesting 7 mL/kg of water. Upon arrival, participants voided, and a urine sample was obtained to measure urine specific gravity (MASTER-SUR, Atago, Japan). A threshold of < 1.020 for urine specific gravity was used to certify euhydration before the trials [34]. The capsule with the assigned experimental treatment was provided in an unidentifiable bag and ingested. Then, participants rested supine for 60 min to allow the substance absorption.
Participants were then dressed in a T-shirt, and shorts and a heart rate belt (H10, Polar, Finland) was attached to their chest. Then, participants performed a 10-min standardised warm-up at a workload equivalent to 30% of VO2max on the cycle ergometer and the exercise intensity was increased by 10% of VO2max every 3 min until they completed the workload equivalent to 80% of VO2max. The final load was set at 80% of VO2max because the respiratory exchange ratio was > 1.00 for all individuals beyond this workload. At the end of each workload, the rating of perceived exertion was measured with the 6–20 point Borg scale [35]. During the whole exercise trial, expired gases were collected and measured by the same breath-by-breath analyser used for the pre-experimental trial and representative values of VO2 and VCO2 and heart rate were assessed for each workload by averaging the last 60 s of each stage [36]. The gas analyser used for this investigation has good inter-day reliability for respiratory measurements (CV = 7.7 ± 5.5% for the maximal rate of fat oxidation (MFO), and CV = 6.5 ± 8.0% for Fatmax [32]). The rate of energy expenditure and fat and carbohydrate oxidation were calculated from stoichiometric equations assuming that urinary nitrogen excretion was negligible [37, 38]. Energy expenditure (kcal/min) during exercise was calculated as (3.869 × VO2) + (1.195 × VCO2), where VO2 and VCO2 are in L/min. Fat oxidation rate (g/min) was calculated as (1.67 × VO2) − (1.67 × VCO2) and carbohydrate oxidation rate (g/min) was calculated as (4.55 × VCO2) − (3.21 × VO2). In each trial, MFO was individually calculated for each participant as the highest value of fat oxidation rate obtained during the incremental exercise intensity test. The exercise intensity at which MFO was obtained for each individual was categorised as Fatmax. In addition, the total amount of fat oxidised during each trial was calculated using data from all the expired gases during the whole exercise testing, excluding the warm-up.
Certified calibration gases (16.0% O2; 5.0% CO2, Sanro, Spain) and a 3-L syringe were used to calibrate the gas analyser and the flowmeter before each trial. The same test with the identical workloads and times was used for the three experimental trials being the only difference among them the content of the capsule ingested before exercise. The position of the saddle and handlebar in the cycle ergometer, clothing used, and cycling cadence were meticulously replicated in both trials. After the exercise testing, participants continued with their daily activities but were encouraged to avoid any dietary source of caffeine and alcohol or to perform any extra exercise. Participants completed an ad hoc questionnaire regarding common side effects after acute caffeine intake. This questionnaire included a 1–10-point scale to assess the magnitude of each side effect. Participants were previously informed that one point meant a minimal magnitude of the side effect (equivalent to a normal day) and 10 points meant the highest magnitude of the side effect. Participants were provided with an online version of this questionnaire via WhatsApp, and the questionnaire contained two phases. In the first phase, participants had to rate their feelings of nervousness, vigour, irritability, gastrointestinal problems, muscular pain, headache, and diuresis and they completed this questionnaire 12 h after the end of the exercise protocol. In the second phase of the questionnaire, participants rated their level of insomnia during the night after the experimental trial. This survey was completed on the following morning of the experiment once participants had completed their night’s sleep. This two-phase survey has been effectively used to assess side effects resulting from acute caffeine ingestion in individuals performing several exercise situations [39, 40].
Statistical analysis
Data were collected as previously indicated and the results of each test were blindly introduced into the statistical package SPSS v21.0 (IBM, USA) and subsequently analysed. The normality of each variable was initially tested with the Shapiro–Wilk test which confirmed normal distribution for all variables. A one-way analysis of variance (ANOVA) was used to compare MFO and Fatmax, the total amount of fat oxidised, and the magnitude of side effects among trials. A two-way ANOVA (substance × workload; 3 × 6) was used to compare energy expenditure, fat and carbohydrate oxidation rates, heart rate and perceived exertion during exercise. Sphericity assumption was checked with Mauchly’s test. In the case of a main effect of substance, workload, or interaction between these two factors, pairwise comparisons between caffeine and placebo trials (i.e. 3 mg/kg vs 6 mg/kg vs placebo) were performed at each workload and differences were identified with LSD post hoc tests. The Cohen’s effect size (d) was calculated in pairwise comparisons between each caffeine dose and the placebo [41]. In all statistical tests, a significance level of P < 0.050 was set to consider the difference as significant. The data are presented as mean ± standard deviation.
Results
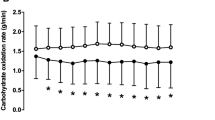
Figure 1 depicts the effect of 3 and 6 mg/kg of caffeine ingestion on fat oxidation, carbohydrate oxidation and energy expenditure during exercise with increasing intensity. There were significant effects of substance (F = 7.969; P = 0.004), exercise intensity (F = 42.535; P < 0.001), and substance × exercise intensity interaction (F = 5.893; P = 0.010) on fat oxidation rate during exercise. The post hoc analysis revealed that the rate of fat oxidation was higher with 3 mg/kg of caffeine than with the placebo at 30, 40, 50 and 70% of VO2max (all P < 0.050, ES from 0.38 to 0.50; Fig. 1). Moreover, the rate of fat oxidation was higher with 6 mg/kg of caffeine than with the placebo at 30, 40, 50 60 and 70% of VO2max (all P < 0.050, ES from 0.28 to 0.76) with no differences between 3 and 6 mg/kg at any exercise intensity. There were main effects of substance (F = 23.580; P < 0.001) and exercise intensity (F = 110.797; P < 0.001), and a substance × exercise intensity interaction (F = 5.993; P = 0.013) on carbohydrate oxidation rate during exercise. The post hoc analysis revealed that the rate of carbohydrate oxidation was lower with 3 mg/kg of caffeine than with the placebo at 70% of VO2max (P = 0.050, ES = 0.41). Similarly, the rate of carbohydrate oxidation was lower with 6 mg/kg of caffeine compared to the placebo at 40, 50 and 70% of VO2max (all P < 0.050, ES from 0.23 to 0.34), with no differences between 3 and 6 mg/kg at any exercise intensity. There was a significant effect of exercise intensity (F = 166.911; P < 0.001) on energy expenditure rate, with no effect of substance or substance × exercise intensity interaction.

Rates of fat oxidation, carbohydrate oxidation and energy expenditure during exercise of increasing intensity after the ingestion of 3 and 6 mg/kg of caffeine or a placebo. Data are mean ± SD for 18 participants. (*) Differences between placebo and 3 mg/kg (P < 0.05). (†) Differences between placebo and 6 mg/kg (P < 0.05)
Figure 2 depicts the effect 3 and 6 mg/kg of caffeine ingestion on heart rate and perceived exertion during exercise of increasing intensity. There was a significant effect of exercise intensity (F = 110.496; P < 0.001) on heart rate, with no effect of substance or substance × exercise intensity interaction. There was a significant effect of exercise intensity (F = 251.436; P < 0.001), and a substance × exercise intensity interaction (F = 5.629; P = 0.016) on the rating of perceived exertion. The post hoc analysis revealed that the rating of perceived exertion was lower with 3 mg/kg of caffeine than with the placebo at 70 and 80% of VO2max (all P < 0.050, ES from 0.51 to 0.71) and with 6 mg/kg of caffeine lower than with the placebo at 80% of VO2max (P < 0.001, ES = 1.48). No differences in the rating of perceived exertion were noted between 3 and 6 mg/kg at any exercise intensity.

Heart rate and perceived exertion during exercise of increasing intensity after the ingestion of 3 and 6 mg/kg of caffeine or a placebo. Data are mean ± SD for 18 participants. (*) Differences between placebo and 3 mg/kg (P < 0.05). (†) Differences between placebo and 6 mg/kg (P < 0.05)
Figure 3 depicts the effect of caffeine on MFO and Fatmax. There was an effect of substance on MFO (F = 7.085; P = 0.003). The post hoc analysis showed that both 3 mg/kg of caffeine (P = 0.021, ES = 0.57) and 6 mg/kg of caffeine (P = 0.001, ES = 0.60) increased MFO over the placebo. However, the intake of caffeine did not modify Fatmax compared to the placebo (F = 0.079; P = 0.924). There was an effect of substance on the total amount of fat oxidised in the trial (F = 8.055; P = 0.001). During the placebo trial, 19.2 ± 8.2 g of fat were oxidised while this value increased to 23.5 ± 10.6 g (P = 0.038, ES = 0.52) with 3 mg/kg of caffeine and to 23.9 ± 9.0 g (P < 0.001, ES = 0.57) with 6 mg/kg of caffeine.

Maximal fat oxidation (MFO) and exercise intensity at maximal fat oxidation (Fatmax) during exercise of increasing intensity after the ingestion of 3 and 6 mg/kg of caffeine or a placebo. Data are mean ± SD for 18 participants. (*) Differences between placebo and 3 mg/kg (P < 0.05). (†) Differences between placebo and 6 mg/kg (P < 0.05)
In the 24 h following the ingestion of substances, both 3 and 6 mg/kg of caffeine increased participants’ feelings of nervousness and vigour (Table 2). However, caffeine did not modify the rating of any other side effect.
Discussion
The aim of this investigation was to test the effect of oral intake of 3 and 6 mg/kg of caffeine on whole-body substrate oxidation during an incremental cycling exercise test. While the study of the potential effect of caffeine to enhance fat oxidation during aerobic exercise has been the topic of previous research [22,23,24, 26, 27] and one meta-analysis [28], the current experiment is the first to analyse whether a dose–response effect of caffeine on fat oxidation during exercise is present or not. The main findings of this research indicate that, in comparison to the placebo trial, oral ingestion of caffeine with a dose of either 3 and 6 mg/kg of caffeine enhanced the rate of fat oxidation at several workloads between 30 and 70% VO2max. The effect of caffeine on fat oxidation rate was of similar magnitude with both doses and there was no difference in fat oxidation rate between 3 and 6 mg/kg of caffeine at any workload. As a result, both doses of caffeine increased MFO from 0.31 g/min to 0.40 g/min in the placebo-caffeine comparison, respectively. In the case that the participants would have maintained exercise at Fatmax for 1 h, the intake of caffeine would have produced a change from 18.8 ± 8.9 g/h to 23.8 ± 8.9 g/h with 3 mg/kg and 24.4 ± 10.9 g/h with 6 mg/kg of caffeine. These changes represent an increase of 31.9–34.2% in the amount of fat oxidised for 1 h with the intake of caffeine. Interestingly, these effects were obtained without any change in energy expenditure or heart rate during the whole exercise protocol while both caffeine doses reduced perceived fatigue at the higher workloads. Collectively, all these outcomes suggest that oral acute ingestion of caffeine between 3 and 6 mg per kg of body mass enhances the utilisation of fat as a fuel at intensities between 30 and 70% of VO2max.
The potential effect of caffeine to enhance fat oxidation during aerobic exercise, at the expenses of lower use of carbohydrates, was established at the end of the 1970s [27, 42, 43]. However, the existence of this effect was disputed for several decades as there were contradictory results regarding the effect of caffeine on the rate of fat utilisation during aerobic exercise [44,45,46]. The conflicting results can be explained by the type of exercise protocol used to assess the effect of caffeine on fat oxidation (free-chosen vs fixed exercise intensity). In those protocols designed to measure the ergogenic effect of caffeine with free-chosen intensity protocols, caffeine habitually increased performance but failed to produce any effect on the shifting of substrate oxidation. This point may be easily explained because in trials with free-chosen intensity caffeine enhances exercise intensity (e.g. ergogenic effect) which counteracts the effect of caffeine on fat oxidation rate [25]. On the other hand, acute caffeine intake has the capacity to enhance the rate of fat oxidation in those investigations that compared caffeine to placebo using a protocols of fixed exercise intensity, either in incremental [23] or in steady-state tests [22]. The current investigation provides further evidence of the caffeine-induced effect on fat oxidation rate during submaximal aerobic exercise in a protocol with normalised exercise intensity. Moreover, the present study is innovative because it supplies the first evidence to recommend the use of either a dose of 3 or 6 mg of caffeine per kg of body mass to improve fat oxidation during exercise.
In 1995, Graham and Spriet [15] carried out an elegant study to determine metabolic, catecholamine and exercise performance responses to 3, 6 and 9 mg/kg of caffeine. In their investigation, these authors found that a dose-related response in the concentration of epinephrine and free-fatty acids (FFA) at rest. However, the ergogenic benefit of caffeine, measured as the time to exhaustion during running at 85% of VO2max, was of similar magnitude with 3, 6 and 9 mg/kg of caffeine. This investigation established the starting point of the lack of dose–response, in terms of ergogenic effect, of oral caffeine intake and contributed to the current knowledge that considers caffeine as a substance that produces comparable benefits in the dose range of 3–9 mg/kg, at least for individuals with low habituation to caffeine [15, 17, 18]. Graham and Spriet’s investigation [15] also contributed to understand the mechanism associated to caffeine’s ergogenicity as the metabolic responses seemed to uncouple from the performance benefits of the substance. The blockade of adenosine receptors was then confirmed as the most plausible mechanism explaining the ergogenic effect of caffeine [47], while the metabolic effect may an accessory mechanism for endurance events in which glycogen spring may entail some benefit on performance. Although less related to exercise performance, ascertaining whether the dose-related effect of caffeine on epinephrine- and free-fatty acid release [15] produces a dose–response effect on fat oxidation is also scientifically relevant. This is because enhanced fat oxidation during aerobic exercise is an objective of athletes/sportspeople seeking body fat reduction. The current investigation sheds light on this topic as the effect of caffeine on fat oxidation during exercise was similar with 3 and 6 mg/kg of caffeine. Moreover, the effect was present with both doses at intensities between 30 and 70%VO2max and none of the doses produced any effect on energy expenditure or heart rate during exercise. As presented in Fig. 1, the curve of fat oxidation rate-exercise intensity was almost identical with 3 and 6 mg/kg of caffeine. In fact, both doses of caffeine produced an increase of 0.09 g/min in MFO over the placebo trial (Fig. 3). The effect of caffeine on fat oxidation found in this investigation was similar to the one found during a ramp exercise test with 3 mg/kg of caffeine (+0.09–0.14 g/min [23, 24]) or the mean effect found during 1 h of exercise at Fatmax (+0.08 g/min [22]). Collectively, this information supports that doubling the dose of caffeine from 3 to 6 mg/kg does not produce a further benefit at increasing fat oxidation rates during aerobic exercise.
This study presents some limitations that should be discussed to understand the true scope of the study outcomes: (i) the participants of this experiment were individuals that practised recreational exercise at least 4 days per week. Their values of MFO and Fatmax with the placebo were in the 20th percentile for recreationally active, lean males [48]. In fact, most of the recent investigation on the effect of caffeine on fat oxidation during exercise has been carried out with samples of recreationally active individuals [22,23,24]. Therefore, it is safe to conclude that caffeine enhances fat oxidation during exercise in recreationally active individuals, but further research is needed in other populations such as endurance-trained athletes and obese/overweight individuals to assure that this effect is present in these populations. (ii) The sample was composed of male participants. Although recent evidence suggests that men and women obtain similar ergogenic benefits from oral caffeine intake [49, 50], it is still necessary to determine whether women also obtain enhanced fat oxidation with oral caffeine intake at different doses. (iii) We included low daily caffeine intake as an inclusion criterion to participate in the study. It is thus needed to investigate if the effect of caffeine on fat oxidation still exists in participants with high levels of daily caffeine intake as tolerance to the ergogenic properties [51] and the cardiovascular effect [52] of caffeine has been found with a chronic intake of the substance. (iv) We obtained only samples of expired air during exercise while blood and tissue samples would have been helpful to determine molecular and physiological pathways that explain such caffeine-derived effects on energy metabolism [53]. (v) We tested two doses of caffeine which are within the most commonly recommended in the context of exercise [13, 14]. However, the effect of caffeine on fat oxidation may be different with higher doses of caffeine as 9 mg/kg was the dose that produced the highest increase in epinephrine and FFA concentrations in the study by Graham and Spriet [15]. In addition, it is necessary to establish the minimal effective doses of caffeine for enhanced fat oxidation by investigating doses below 3 mg/kg. Future investigation should also determine if the effect of caffeine on fat oxidation is still maintained in the fed state, as in the current investigation, participants were in a fasted state to avoid any interference of carbohydrate intake the potential effect of caffeine on substrate oxidation.
In summary, acute oral ingestion of either 3 or 6 mg of caffeine per kg of body mass was effective to increase fat oxidation during exercise at 30–70% VO2max. Both doses produced an effect of similar magnitude on fat oxidation during exercise as 3 m/kg increased MFO by 26.7 ± 43.4% and 6 mg/kg by 28.6 ± 32.6%. The increase in fat oxidation at low-to-moderate intensities was not accompanied by higher energy expenditure rates or higher heart rates. However, both doses of caffeine also reduced carbohydrate oxidation rates at several workloads and perceived fatigue during the most intense workloads. From a practical perspective, it seems more recommendable to use 3 mg/kg instead of 6 mg/kg of caffeine to obtain a potential effect of caffeine on shifting substrate oxidation towards a higher reliance on fat during aerobic exercise. This is because the prevalence and magnitude of several side effects associated with oral caffeine intake increase along with the dose of caffeine, as found here and elsewhere [54].
References
Reyes CM, Cornelis MC (2018) Caffeine in the diet: country-level consumption and guidelines. Nutrients 10:1772
Barrea L, Pugliese G, Frias-Toral E et al (2021) Coffee consumption, health benefits and side effects: a narrative review and update for dietitians and nutritionists. Crit Rev Food Sci Nutr. https://doi.org/10.1080/10408398.2021.1963207
Ágoston C, Urbán R, Király O et al (2018) Why do you drink caffeine? The development of the Motives for Caffeine Consumption Questionnaire (MCCQ) and its relationship with gender, age and the types of caffeinated beverages. Int J Ment Health Addict 16:981. https://doi.org/10.1007/S11469-017-9822-3
Mitchell DC, Knight CA, Hockenberry J et al (2014) Beverage caffeine intakes in the US. Food Chem Toxicol 63:136–142. https://doi.org/10.1016/J.FCT.2013.10.042
Aguilar-Navarro M, Muñoz G, Salinero JJ et al (2019) Urine caffeine concentration in doping control samples from 2004 to 2015. Nutrients 11:286. https://doi.org/10.3390/nu11020286
Lara B, Gonzalez-Millán C, Salinero JJ et al (2014) Caffeine-containing energy drink improves physical performance in female soccer players. Amino Acids 46:1385–1392. https://doi.org/10.1007/s00726-014-1709-z
Del Coso J, Ramírez JA, Muñoz G et al (2013) Caffeine-containing energy drink improves physical performance of elite rugby players during a simulated match. Appl Physiol Nutr Metab 38:368–374. https://doi.org/10.1139/apnm-2012-0339
Del Coso J, Portillo J, Salinero JJ et al (2016) Caffeinated energy drinks improve high-speed running in elite field hockey players. Int J Sport Nutr Exerc Metab 26:26–32. https://doi.org/10.1123/ijsnem.2015-0128
Puente C, Abián-Vicén J, Salinero JJ et al (2017) Caffeine improves basketball performance in experienced basketball players. Nutrients. https://doi.org/10.3390/nu9091033
Pérez-López A, Salinero JJ, Abian-Vicen J et al (2014) Caffeinated energy drinks improve volleyball performance in elite female players. Med Sci Sports Exerc 47:850–856. https://doi.org/10.1249/MSS.0000000000000455
Abian P, Del Coso J, Salinero JJ et al (2015) The ingestion of a caffeinated energy drink improves jump performance and activity patterns in elite badminton players. J Sports Sci 33:1042–1050. https://doi.org/10.1080/02640414.2014.981849
Diaz-Lara FJ, Del Coso J, Portillo J et al (2016) Enhancement of high-intensity actions and physical performance during a simulated Brazilian jiu-jitsu competition with a moderate dose of caffeine. Int J Sports Physiol Perform 11:861–867. https://doi.org/10.1123/ijspp.2015-0686
Maughan RJ, Burke LM, Dvorak J et al (2018) IOC consensus statement: dietary supplements and the high-performance athlete. Br J Sports Med 52:439–455. https://doi.org/10.1136/bjsports-2018-099027
Guest NS, VanDusseldorp TA, Nelson MT et al (2021) International society of sports nutrition position stand: caffeine and exercise performance. J Int Soc Sports Nutr 18:1
Graham TE, Spriet LL (1995) Metabolic, catecholamine, and exercise performance responses to various doses of caffeine. J Appl Physiol 78:867–874. https://doi.org/10.1152/jappl.1995.78.3.867
Desbrow B, Biddulph C, Devlin B et al (2012) The effects of different doses of caffeine on endurance cycling time trial performance. J Sports Sci 30:115–120. https://doi.org/10.1080/02640414.2011.632431
Pallarés JG, Fernández-Elías VE, Ortega JF et al (2013) Neuromuscular responses to incremental caffeine doses: performance and side effects. Med Sci Sports Exerc 45:2184–2192. https://doi.org/10.1249/MSS.0b013e31829a6672
Bruce CR, Anderson ME, Fraser SF et al (2000) Enhancement of 2000-m rowing performance after caffeine ingestion. Med Sci Sports Exerc 32:1958–1963. https://doi.org/10.1097/00005768-200011000-00021
Del Coso J, Salinero JJ, González-Millán C et al (2012) Dose response effects of a caffeine-containing energy drink on muscle performance: a repeated measures design. J Int Soc Sports Nutr. https://doi.org/10.1186/1550-2783-9-21
Astorino TA, Terzi MN, Roberson DW, Burnett TR (2010) Effect of two doses of caffeine on muscular function during isokinetic exercise. Med Sci Sports Exerc 42:2205–2210. https://doi.org/10.1249/MSS.0B013E3181E3A11D
Spriet LL (2014) Exercise and sport performance with low doses of caffeine. Sports Med 44(Suppl 2):175–184. https://doi.org/10.1007/S40279-014-0257-8
Ruiz-Moreno C, Gutiérrez-Hellín J, Amaro-Gahete FJ et al (2020) Caffeine increases whole-body fat oxidation during 1 h of cycling at Fatmax. Eur J Nutr. https://doi.org/10.1007/s00394-020-02393-z
Gutiérrez-Hellín J, Del Coso J (2018) Effects of p-synephrine and caffeine ingestion on substrate oxidation during exercise. Med Sci Sports Exerc 50:1899–1906. https://doi.org/10.1249/MSS.0000000000001653
Ramírez-Maldonado M, Jurado-Fasoli L, del Coso J et al (2021) Caffeine increases maximal fat oxidation during a graded exercise test: is there a diurnal variation? J Int Soc Sports Nutr. https://doi.org/10.1186/s12970-020-00400-6
Ruiz-Moreno C, Amaro-Gahete FJ, González-García J et al (2022) Caffeine increases exercise intensity and energy expenditure but does not modify substrate oxidation during 1 h of self-paced cycling. Eur J Nutr. https://doi.org/10.1007/s00394-022-02894-z
Bangsbo J, Jacobsen K, Nordberg N et al (1992) Acute and habitual caffeine ingestion and metabolic responses to steady-state exercise. J Appl Physiol 72:1297–1303. https://doi.org/10.1152/JAPPL.1992.72.4.1297
Costill DL, Dalsky GP, Fink WJ (1978) Effects of caffeine ingestion on metabolism and exercise performance. Med Sci Sports 10:155–158
Collado-Mateo D, Lavín-Pérez AM, Merellano-Navarro E, Del Coso J (2020) Effect of acute caffeine intake on the fat oxidation rate during exercise: a systematic review and meta-analysis. Nutrients 12:1–18. https://doi.org/10.3390/nu12123603
Filip A, Wilk M, Krzysztofik M, Del Coso J (2020) Inconsistency in the ergogenic effect of caffeine in athletes who regularly consume caffeine: is it due to the disparity in the criteria that defines habitual caffeine intake? Nutrients 12:1087. https://doi.org/10.3390/nu12041087
Ruíz-Moreno C, Gutiérrez-Hellín J, González-García J et al (2021) Effect of ambient temperature on fat oxidation during an incremental cycling exercise test. Eur J Sport Sci 21:1140–1147. https://doi.org/10.1080/17461391.2020.1809715
Gutiérrez-Hellín J, Del Coso J (2018) Dose-response effects of p-synephrine on fat oxidation rate during exercise of increasing intensity. Phyther Res. https://doi.org/10.1002/ptr.5937
Robles-González L, Gutiérrez-Hellín J, Aguilar-Navarro M et al (2021) Inter-day reliability of resting metabolic rate and maximal fat oxidation during exercise in healthy men using the ergostik gas analyzer. Nutrients. https://doi.org/10.3390/NU13124308
Edvardsen E, Hem E, Anderssen SA (2014) End criteria for reaching maximal oxygen uptake must be strict and adjusted to sex and age: a cross-sectional study. PLoS ONE 9:e85276. https://doi.org/10.1371/journal.pone.0085276
Casa DJ, Armstrong LE, Hillman SK et al (2000) National athletic trainers’ association position statement: fluid replacement for athletes. J Athl Train 35:212–224
Borg G (1990) Psychophysical scaling with applications in physical work and the perception of exertion. Scand J Work Environ Health. https://doi.org/10.5271/sjweh.1815
Achten J, Venables MC, Jeukendrup AE (2003) Fat oxidation rates are higher during running compared with cycling over a wide range of intensities. Metabolism. https://doi.org/10.1016/S0026-0495(03)00068-4
Brouwer E (1957) On simple formulae for calculating the heat expenditure and the quantities of carbohydrate and fat oxidized in metabolism of men and animals, from gaseous exchange (oxygen intake and carbonic acid output) and urine-N. Acta Physiol Pharmacol Neerl 6:795–802
Frayn KN (2016) Calculation of substrate oxidation rates in vivo from gaseous exchange. J Appl Physiol. https://doi.org/10.1152/jappl.1983.55.2.628
Salinero JJ, Lara B, Abian-Vicen J et al (2014) The use of energy drinks in sport: perceived ergogenicity and side effects in male and female athletes. Br J Nutr 112:1494–1502. https://doi.org/10.1017/S0007114514002189
Lara B, Ruiz-Vicente D, Areces F et al (2015) Acute consumption of a caffeinated energy drink enhances aspects of performance in sprint swimmers. Br J Nutr 114:908–914. https://doi.org/10.1017/S0007114515002573
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, Mahwah
Ivy JL, Costill DL, Fink WJ, Lower RW (1979) Influence of caffeine and carbohydrate feedings on endurance performance. Med Sci Sports 11:6–11
Essig D, Costill D, Van Handel P (1980) Effects of caffeine ingestion on utilization of muscle glycogen and lipid during leg ergometer cycling. Int J Sports Med 01:86–90. https://doi.org/10.1055/s-2008-1034637
Green J, Olenick A, Eastep C, Winchester L (2016) Caffeine effects on velocity selection and physiological responses during RPE production. Appl Physiol Nutr Metab 41:1077–1082. https://doi.org/10.1139/APNM-2016-0098
Glaister M, Pattison JR, Muniz-Pumares D et al (2015) Effects of dietary nitrate, caffeine, and their combination on 20-km cycling time trial performance. J Strength Cond Res 29:165–174. https://doi.org/10.1519/JSC.0000000000000596
Graham TE, Helge JW, MacLean DA et al (2000) Caffeine ingestion does not alter carbohydrate or fat metabolism in human skeletal muscle during exercise. J Physiol 529:837–847. https://doi.org/10.1111/j.1469-7793.2000.00837.x
Davis JM, Zhao Z, Stock HS et al (2003) Central nervous system effects of caffeine and adenosine on fatigue. Am J Physiol Integr Comp Physiol 284:R399–R404. https://doi.org/10.1152/ajpregu.00386.2002
Maunder E, Plews DJ, Kilding AE (2018) Contextualising maximal fat oxidation during exercise: determinants and normative values. Front Physiol 23:599
Lara B, Salinero JJ, Giráldez-Costas V, Del Coso J (2021) Similar ergogenic effect of caffeine on anaerobic performance in men and women athletes. Eur J Nutr 60:4107–4114. https://doi.org/10.1007/s00394-021-02510-6
Skinner TL, Desbrow B, Arapova J et al (2019) Women experience the same ergogenic response to caffeine as men. Med Sci Sport Exerc. https://doi.org/10.1249/MSS.0000000000001885
Lara B, Ruiz-Moreno C, Salinero JJ, Del Coso J (2019) Time course of tolerance to the performance benefits of caffeine. PLoS ONE 14:e0210275. https://doi.org/10.1371/journal.pone.0210275
Ruiz-Moreno C, Lara B, Salinero JJ et al (2020) Time course of tolerance to adverse effects associated with the ingestion of a moderate dose of caffeine. Eur J Nutr. https://doi.org/10.1007/s00394-019-02167-2
Romijn JA, Coyle EF, Sidossis LS et al (1993) Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am J Physiol-Endocrinol Metab. https://doi.org/10.1152/ajpendo.1993.265.3.E380
de Souza JG, Del Coso J, de Fonseca F, S, et al (2022) Risk or benefit? Side effects of caffeine supplementation in sport: a systematic review. Eur J Nutr. https://doi.org/10.1007/S00394-022-02874-3
Acknowledgements
The authors wish to thank the participants for their invaluable contribution to the study.
Funding
The study was part of the project supported by a Grant from the Universidad Francisco de Vitoria, registered under the code UFV-2020-18.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors declare no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; and no other relationships or activities that could appear to have influenced the submitted work.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gutiérrez-Hellín, J., Aguilar-Navarro, M., Ruiz-Moreno, C. et al. Effect of caffeine intake on fat oxidation rate during exercise: is there a dose–response effect?. Eur J Nutr 62, 311–319 (2023). https://doi.org/10.1007/s00394-022-02988-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-022-02988-8