
Abstract
Introduction
Trans-fatty acids (TFAs) can be produced either from bio-hydrogenation in the rumen of ruminants or by industrial hydrogenation. While most of TFAs’ effects from ruminants are poorly established, there is increasing evidence that high content of industrial TFAs may cause deleterious effects on human health and life span.
Material and methods
Indeed, several epidemiological and experimental studies strongly suggest that high content of most TFA isomers could represent a higher risk of developing cardiovascular diseases by a mechanism that lowers the “good HDL cholesterol” and raises the “bad LDL cholesterol.”
Results
With respect to the general precautionary principle and considering the existence of an international policy consensus regarding the need for public health action, some industrialized countries, such as France, are still not sufficiently involved in preventive strategies that aim to efficiently reduce TFAs content and TFAs consumption and produce alternative healthier fat sources.
Conclusion
In this manuscript, we provide an overview about TFAs origins, their use and consumption among French population. We also discuss their potential human health implications as well as the preventive and regulatory measures undertaken in France.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Unlike other dietary fats, trans-fatty acids (commonly shortened to trans fats or TFAs) are neither essential nor salubrious and, in fact, their consumption can lead to higher risk of some pathologies, such as cardiovascular diseases [1].
TFAs arise through partial hydrogenation or isomerization (i.e. reduction in unsaturation) of cis unsaturated fatty acids (UFAs) [1]. TFAs can be produced by two major sources: (1) the bio-hydrogenation, which is naturally occurring in ruminants (e.g. cows, sheep) and involves bacterial enzymes (e.g. desaturases) as catalysts and (2) the partial catalytic hydrogenation of vegetables or fish oils, which is an industrial process that requires hydrogen gas and a metal catalyst in order to modify the physical–chemical properties of UFAs (e.g. decrease in their oxidation sensitivity, solidification of vegetable fat products) [1].
In terms of quantitative distribution, the total content of TFAs and isomers, in either natural (i.e. pasture) or industrial (i.e. conventional) food products, can largely vary between products, while the qualitative nature of TFAs is usually quite similar [2]. As a result, the fat in milk, butter, cheese and beef approximately contains 2-9 % TFAs, whereas industrial products such as margarines and “shortenings” (e.g. containing partially hardened vegetable oils such as baking or frying fats) can reach over 50 % of total FAs [2–4].
Furthermore, TFAs qualitatively differ according to the feeding source. Indeed, feeding of pasture (i.e. natural fat foods) results in high amounts of vaccenic acid (i.e. oleic acid isomer trans-11 aka 18:1 Δ11 trans), which can be converted in mammals into small amounts of the conjugated linoleic acid (CLA) 18:2 cis-9, trans-11 [2, 5], whereas conventional feeding (i.e. industrial/hydrogenated fat foods) mainly results in high amounts of elaidic acid (i.e. oleic acid isomer trans-9 aka 18:1, Δ9 trans) [2, 6]. In some cases, such as during partial hydrogenation of fish oils, trans-isomers of the omega-3 eicosapentaenoic acid (EPA aka 20:5) and docosahexaenoic acid (DHA aka 22:6) are predominant [7]. Besides, gamma-linoleic trans-isomers (18:2) and of alpha-linolenic acid (18:3) may arise from deep fat frying [8].
Nowadays, ruminant fats are considered as the major source of TFAs in most European countries because of the step reduction in the production and intake of industrial TFAs [9]. It was predicted that it will likely become so in the USA [10]. Nevertheless, the specific effects of ruminant TFAs on health are unclear as they can hardly be discriminated from the industrial ones. Indeed, the current epidemiological and experimental studies remain limited and controversial to correctly associate TFAs intake, whatever their origins, with the risk of causing deleterious human health effects (e.g. “non-communicable diseases” such as cardiovascular diseases, obesity, diabetes or cancers) [11–22]. For instance, a debatable positive association between industrial TFAs consumption and the risk of developing coronary heart disease has been shown and further explained by a TFAs-mediated increase in the plasmatic LDL level (low-density lipoprotein or “bad cholesterol”) and decrease in the plasmatic HDL level (high-density lipoprotein or “good cholesterol”) [1, 11, 12, 14, 15, 18–22]. In this context, one can notably argue about the presence of TFAs in a number of products such as marketed capsules promoted for weight loss for which no strong evidence of their safety in humans has been demonstrated [23, 24].
Eventually, the 2004 World Health Organization (WHO) Global Strategy on Diet, Physical Activity and Health endorsed the recommendation that TFAs intake should not exceed 1 % of the total energy intake (TEI) [25]. In 2007, the PAHO/WHO Task Force on “Trans Fat Free Americas” recommended that industrial TFAs should be eliminated from the food supply across the American continent [26]. Ultimately, in addition to other proposals (e.g. food labeling, health claims regulation disclosing fat content of foods supplied in restaurants and food programs), this same organization suggested that TFAs content should not reach more than 2 % of total fat in vegetable oils and margarines, and no more than 5 % in other foods [26]. Despite these international recommendations, only few governments have implemented a TFA policy. For instance, in France, strategies to reduce TFAs consumption are still required and shall range from public health approaches such as the use of dietary guidelines and health promotion programs, mandatory labeling of TFAs content in food and voluntary agreements with the food industry to reduce TFAs content and produce alternative healthier fat sources.
Our present work aims to review the TFAs origins, use, consumption and regulation in France comparatively to some reference countries (e.g. Denmark), as well as their implications on human health.
Definition, nomenclature and properties of fatty acids: an overview
Definition and nomenclature of cis-fatty acids
The term fatty acid (FA) designates any one of the aliphatic monocarboxylic acids that can be liberated by hydrolysis from naturally occurring fats and oils [27, 28]. FAs play multiple and essential cellular roles (e.g. energy production, membrane structures, immune cell regulation, cell signaling, gene expression and regulation) [29–33].
Depending on the absence or presence of a double bond, the FA is called “saturated” (SFA) (e.g. palmitic acid 16:0, arachidic acid 20:0) or unsaturated (UFA), respectively [7, 33]. When the chain presents one or several double bonds, the FA is called monounsaturated (MUFA) or polyunsaturated (PUFA), respectively [7, 33]. Thereby, MUFAs occur naturally in various animal and vegetable fats and can be obtained by biotransformation of SFAs [34]. MUFA group is represented by the oleic acid (18:1), which belongs to the family omega 9 (ω9 or serial n-9). It is formed by a chain of 18 carbons and one double bond in configuration cis at the position 9 (aka ∆9, which represents the number of carbon atoms from the α-carbon/carboxylic group (–COOH) to the nearest double bond). The PUFA group is divided into two major families: (1) under the appellation omega-3 (ω3 or serial n−3) such as linolenic acid 18:3, EPA 20:5 or DHA 22:6 and (2) under the appellation omega-6 (ω6 or serial n−6) such as linoleic acid 18:2 or arachidonic acid 20:4 [7, 33]. Their classification (i.e. omega-3 or omega-6) is obtained by subtracting the highest double bond—which is, respectively, located three or six carbons away from the “omega” carbon/opposite end of the carboxyl group (e.g. 15 in the case of α-linolenic acid)—from the number of carbons in the FA (e.g. 18 in the case of α-linolenic acid). The PUFAs linolenic and linoleic acids are essential in humans—they cannot be synthesized by the organism and cannot be obtained from biotransformation of SFAs or MUFAs—and so, they must be provided by food (e.g. vegetables), preferentially at the 5/1 ratio [34]. Eventually, by successive elongations and desaturations, PUFAs can be converted into longer unsaturated carbonated FAs chain (e.g. linolenic acid 18:3 can be converted into EPA 20:5 which, in turns, can be converted into DHA 22:6) [34].
Eventually, several ways exist to write an unsaturated FA, depending on the terminology adopted by biochemists, chemists and physiologists [35, 36]. In the chemist’s terminology, the carbon atoms are counted from the carboxyl group (–COOH) which put the emphasis on the double bond closet to this group (∆-notations) [35]. However, in the biochemist’s and physiologist’s terminology, a new numbering system for the unsaturation of FAs called the “omega nomenclature” was proposed by Holman RT in 1964 and consists of counting the carbon atoms from the methyl (–CH3) determining the metabolic family, noted by ωx (e.g. ω3) or better n−x (n for the total number of carbon, x being the position of the distal double bond) [36]. For instance, linoleic acid (aka cis-9, cis-12-octadecadienoic acid) can also be written 18:2 9c, 12c; 18:2 ∆9, 12 or 18:2 (n−6) or 18:2 ω6 [7, 33].
Definition and properties of trans-fatty acids
Naturally occurring FAs usually have the cis-configuration. Nevertheless, under certain conditions (e.g. partial catalytic hydrogenation or enzymatic hydrogenation), a double bond in FAs may change from a cis (Z) to a trans (E) configuration (geometric isomerization) and/or move to other positions in the carbon chain (positional isomerization) [7, 37].
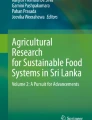
In configuration cis, the two hydrogen atoms are on the same side of the carbon chain with respect to the double bond, a situation that produces a bend in the FAs, whereas in the configuration trans, the two atoms of hydrogen are diagonally opposed to each other, straightening the carbon chain (Fig. 1). For instance, oleic acid (18:1) can be found either as a geometric trans-isomer called elaidic acid (18:1 9t) or as a positional trans-isomer called vaccenic acid (18:1 11t) (Fig. 1). The case of PUFAs is more complex since their double bonds can be found in configuration trans or cis/trans. Indeed, linoleic acid (18:2 9c, 12c) can be found in three possible geometric isomers: 18:2 9c, 12t; 18:2 9t, 12c and/or 18:2 9t, 12t as well as in two positional isomers 18:2 9c, 13t and/or 18:2 9c, 11t (Fig. 2). In natural conjugated linoleic acid (CLA), the collective name for a range of conjugated octadecadienoic geometrical and positional isomers, 18:2 9c, 11t, is always the major isomer formed during microbial biohydrogenation of LA. In industrial preparations, the 9c, 11t and 10t, 12c isomers are the major components. CLA can occur naturally at low levels in a range of products, but is highest (about 0.5 % of total fat) in ruminants, both in meat and in dairy products. It is also produced on an industrial scale by alkaline isomerization of LA (e.g. from sunflower or safflower oil) and is often referred to as commercial CLA [38]. Interestingly, CLA is a fatty acid that is currently receiving considerable attention because of a range of properties that may make a positive contribution to health at moderate doses [38].

Isomers of the oleic acid (aka cis-Δ9-Octadecenoic acid, C18H34O2 or 18:1-9c). a Represents this MUFA in its configuration cis (Z). In this configuration, hydrogen atoms are on the same side of the carbon chain with respect to the double bond, a situation that produces a bend in the FAs. Cis-oleic acid can be transformed into configuration trans (E). In this case, the two atoms of hydrogen are diagonally opposed to each other, straightening the carbon chain. Thereby, trans-isomers of (a) can be either b geometric, represented by the elaidic acid (18:1 9t), which is mostly encountered in partially hydrogenated products (i.e. industrial fat foods such as margarines) or c positional represented by the vaccenic acid (18:1 11t), frequently observed in biohydrogenated dairy products (i.e. natural fat foods such as milk). The structures were assessed using online available lipid maps tools [156, 157]

Isomers of the linoleic acid (aka cis-Δ9, cis-Δ12-Octadecenoic acid, C18H32O2 or 18:2-9c, 12c). a Represents this PUFA in its configuration cis, which can be transformed into: b three possible geometric isomers: 18:2 9c, 12t; 18:2 9t, 12t and 18:2 9t, 12c of linoleic acid (LA) or: c two possible positional isomers: 18:2 9c, 11t and 18:2 9c, 13t of LA. The structures were assessed using online available lipid maps tools [156, 157]
Eventually, the physical–chemical properties of FAs have further implications in health and industrial applications (e.g. preparation of shortenings). Thereby, in addition to be characterized by a higher rigid carbon (acyl-) chain, TFAs differ from cis-FAs by their polarity and by a much higher melting point than FAs [39]. For instance, oleic acid 18:1 9c melts at 4 °C, whereas its trans-isomers, the elaidic acid 18:1 9t and vaccenic acid 18:1 11t, melt between 42 and 44 °C and 44 and 45 °C, respectively [39].
Origins of trans-fatty acids
In human diets, TFAs may arise from three sources: a natural one (i.e. biohydrogenation), an industrial one (i.e. catalytic hydrogenation) and a technological/domestic one (i.e. extreme thermal treatments) that is often forgotten, probably because it is considered as a minor source.
Biohydrogenation
The biohydrogenation mainly results from the enzymatic transformation of cis-FAs into TFAs by the bacterial flora (aka microbiome) present in the rumen of animals (e.g. cows, cheeps, goats) [2]. They also can be produced by mammalian breasts through the action of the Δ9-desaturase [40–42]. Natural TFAs are found in different quantities (up to 10 % of total FAs) predominantly in milk, derived milk products (e.g. butter, cheese) and meats [2, 43–45]. The corresponding TFA isomers are mainly represented by the vaccenic acid (18:1 11t) at a quantity ranging from 30 to more than 50 % of the 18:1 [2, 43, 46]. This quantitative variation can depend on the race, stage of lactation, age and seasonal alimentation of mammalians (e.g. ruminants) [47–49].
Partial catalytic hydrogenation
The chemistry of hydrogenation, initially developed in the late nineteenth century by the Nobel laureate Paul Sabatier and the German chemist Wilhelm Normann, is an industrial process that leads to a reduction in FAs unsaturation in order to solidify vegetable fats, decrease their oxidation sensitivity and enhance their taste [50, 51]. Thereby, vegetable oils are often processed in agro-industries [52–54], notably to produce margarines as well as “shortenings” which are anhydrous fat products used for cooking and confecting other products (e.g. chocolates, cakes, pizzas) [55, 56]. The amount of TFAs in margarines varied from 1 to 2 % (e.g. high-quality margarine) to 60 % (e.g. low-quality margarine) of total FAs [54, 55]. Industrial TFAs are principally composed of the oleic acid isomers 18:1 9t (elaidic acid) and 18:1 10t, which represent up to 85–95 % of the 18:1 [52–56].
The use of some industrial processes such as the trans-esterification to produce shortenings largely contributes to decrease the TFAs level in those products and their derived products [55, 57, 58]. However, in some partially hydrogenated vegetable oils (PHVO), TFAs levels are still too high [6].
Extreme thermal treatments
Thermal treatments involving technology (e.g. deodorization during oil refining) and domestic processes (e.g. dry pan frying, barbecue or long-time baking at high temperatures) can generate TFA isomers [59, 60]. Indeed, oils exposed at very high temperatures induced high amounts of gamma-linoleic acid (18:2 9c, 12c) and alpha-linolenic acid (18:3 9c, 12c, 15c) trans-isomers, while small amounts of oleic acid (18:1 9c) trans-isomers were observed [60, 61]. Globally, the nature and the quantity of TFA isomers generated after thermal treatment depend on the degree of temperature, the duration of treatment and the product itself (e.g. milk, meat, oils). For instance, the trans-isomer of gamma-linoleic acid (18:2 9t 12t) was abundantly (~15–30 % of TFAs) found in vegetable oils (e.g. peanut, sunflower, rape) but was rare in milk when those products were heated at very high temperatures (>200 °C during ~15 min) or used several times [60]. Those generated isomers were stable at very low temperatures (4 or −20 °C) for several weeks (up to 24), but gamma-linoleic acid was much lesser sensitive to isomerization (i.e. about 12–14-folds) than alpha-linolenic acid [62]. Eventually, it was estimated that TFAs originated from thermal treatments would represent 1.3 % of total FAs after heating at 220 °C but represented only 0.2 % at 180 °C, a most commonly used temperature [63].
Analytical methods for TFAs characterization
Several techniques (e.g. GC, TLC, HPLC and FTIR) have been proposed to quantitatively and qualitatively determine TFAs in sample matrices. At every stage of the fat analysis, precautions are requested to minimize the risk of auto-oxidation of unsaturated FAs (i.e. procedures shall be followed under subdued light in an inert atmosphere of nitrogen) and/or enzymatic lipolysis (i.e. analysis or freezing of all tissues shall be followed immediately after removal from the living organism) [7]. Among the major techniques to characterize TFAs, gas chromatography (GC) and Fourier transform infrared spectroscopy (FTIR) represent the two current methods routinely used.
In opposite to FTIR and when suitable standards are available, GC allows the identification of individual FAs [7]. However, in complex mixtures of isomeric FAs such as those present in some foods containing partially hydrogenated vegetable or fish oil, all FAs isomers are rarely resolved by GC, resulting in an overlap of cis- and trans-isomers as well as in biased data [7]. Nevertheless, these overlapping isomers could be quantified using auxiliary fractionation techniques, such as silver nitrate thin-layer chromatography (TLC) or silver ion high-pressure liquid chromatography (Ag+-HPLC) [7, 64]. The problems of cis–trans isomers identification can also be overcome by gas chromatography coupled to mass spectrometry (GC–MS) [7]. In this case, the double bond position can easily be identified by analyzing FA samples as nitrogen compounds such as picolinyl, pyrrolidide or 4,4-dimethyloxazoline derivatives [7, 64, 65]. GC coupled to FTIR (FTIR–GC) can also differentiate cis- and trans-isomers, including those present in PUFAs [7, 66]. Interestingly, an efficient GC method to analyze FAs profile, from biological or food samples, has been described [7]. This method involved three steps: (1) extraction of lipids; (2) conversion of the extracted lipids to a volatile derivative, often to fatty acid methyl esters (FAMEs); and (3) analysis of the FAMEs by GC. Optimal FAs profile analysis was obtained using a flame ionization detector, a carrier gas (e.g. hydrogen or helium) and polar fused silica capillary (PFSC) columns [7]. Furthermore, the use of high elution pressure allowed analysis of complex FA mixtures in shorter times than conventional GC [7]. Eventually, the best separation of FAs from partially hydrogenated vegetable oils with minimum overlaps of cis–trans isomers was achieved when the column temperature was isothermally operated at 180 °C, using hydrogen as the carrier gas with a flow rate of 1.0 ml/min [7, 67]. These GC parameters have been adopted by the American Oil Chemists’ Society (AOCS) in their official method “Ce 1 h-05” to determine the FAs composition by GC in vegetable or non-ruminant animal oils and fats [7, 68]. These GC operating parameters in conjunction with the fat extraction procedure of AOAC Official Method “996.06” [69] are widely used in Canada and the USA for the determination of total fat, SFAs, TFAs, MUFAs and PUFAs as well as for subsequent food labeling [7].
Alternatively, FTIR coupled to attenuated total reflection (ATR) infrared cell technique (FITR–ATR) can determine the total trans content in a very short time (i.e. about 5 min) in pure fats and oil samples without converting them into FAMEs or other derivatives [7, 66].
Consumption levels of TFAs and current recommendations in France
In France, the dietary guidelines are given by committees of experts organized by the Centre National d’Etudes et de Recommendations sur la Nutrition et l’Alimentation (CNERNA) along with the national food council (Conseil National de l’Alimentation; CAN) [70]. The national food consumption database is handled by the Observatoire des Consommations Alimentaires (OCA) [71, 72]. This database includes national individual dietary surveys and continuous national food purchase panels [71]. In spite of several French cohort studies (e.g. TRANSFAIR study [9], E3N-EPIC cohort [73], AQUITAINE survey [74]), information on the French population’s nutritional intake and representative individual consumption level of TFAs in the French population have been mostly provided by AFSSA (Agence Française de Sécurité Sanitaire des Aliments), recently renamed as ANSES (Agence Nationale de Sécurité Sanitaire), through two large dietary surveys: INCA 1 (1998–1999) and INCA 2 (2005–2007) (enquêtes Individuelles Nationales de Consommation Alimentaire) [75, 76], which were combined to the national food composition database CIQUAL (Centre Informatique sur la QUalité des ALiments) available at the time of the investigation [72, 77].
The INCA 1 (1998–1999) represents the second largest national survey on adult and child dietary consumption in France after the ASPCC one (Association Sucre-Produits Sucrés, Consommation, Communication) piloted by CREDOC (Centre de Recherche pour l’ÉtuDe et l’Observation des Conditions de vie) during the period 1993–1994 [70, 78]. The INCA 1 survey described the dietary consumption of 3.003 individual people of 3 years old and above, who were representative of the French population. This survey, which took place after several years, troubled by many food crises (e.g. bovine spongiform encephalopathy (BSE), dioxins or listeria), and the intense debate about genetically modified organisms (GMOs) revealed both a decline in traditional dietary models through the development of fast food products (e.g. pizzas, fizzy drinks or fruit juices) and a strong demand from consumers for information, control by the public authorities and scientific research in the fields of food safety and nutrition [76]. According to this survey, the average consumption of TFAs in adults (2.8 g/day in women and 3.4 g/day in men) was independent of the gender and not significantly different from the one observed in children (2.7 g/day in girls and 3.0 g/day in boys) [75]. Importantly, this consumption level was higher than the one observed from the TRANSFAIR study (2.1 g/day in women and 2.7 g/day in men) [9]. Furthermore, the INCA 1 survey revealed that the consumption of TFAs was increased from the age-group 15–24 (3.55 %) to the group older than 65 years (4.01 %) [75]. Spearman correlation studies, after adjustment with age, showed that daily intake of TFAs was strongly associated with SFA amounts independently of the gender [75]. After adjustment with calorie diet, this association was still significant in adults but reduced in children [75]. The “strong” consumers were usually young participants, and the TFAs overall consumption was superior to 4.89 g/day in girls and 5.79 g/day in boys [75]. Nevertheless, a high distortion may exist if interindividual analysis of TFA consumption is done. Besides, it was shown that 303 and 311 food products in girls and women, respectively, versus 299 and 331 in boys and men, respectively, contribute to the total TFAs intake [75]. Among the most consumed TFAs-containing food groups in adults versus in children, the butter (29.15 % vs. 24.04 %), the cheeses (17.75 % vs. 10.05 %), the meats (9.18 % vs. 8.97 %) and the pastries (6.63 % vs. 10.38 %) contributed together to approximately 62.71 % of total TFAs in adults and about 53.44 % in children [75]. Eventually, in the analyzed population, the average consumption of TFAs corresponded to 1.3 % TEI. In adults, 5 % of the population reached the threshold of 2 % TEI, while boys of 12–14 years represented the most consuming group with nearly 8 g/day of TFAs, largely exceeding this threshold.
The INCA 2 (2005–2007), the third largest national individual survey on food consumption, reported food consumption data gathered over 7 days for over 4,000 participants, adults and children, living in mainland France [76]. The weight and height of the participants as well as information related to their physical activity level, food supplement consumption or food storage practice were also collected. From the analysis of this study in 2008, AFSSA considered that the total TFAs intake level in the French population was lower than the levels observed during INCA 1 [77]. Indeed, the TEI (as a mean of total TFAs intake level) was similar between adults and children and close to 1 %. Furthermore, among the strongest consumers, this level remained below the threshold of 2 % TEI set earlier, regardless of the age and gender [77]. However, it was observed that natural TFAs were predominant in adults, whereas both natural and industrial TFAs were found in children [77]. In spite of lower-level TFAs intake in the general population, AFSSA still recommends a reduced consumption (about 30 %) of TFAs-enriched food products (e.g. cookies, fat meats) [76, 77]. Interestingly, in the French population, approximately 63 % of TFAs consumed originates from animals and 37 % from vegetables [79]. In European countries (including France), average TFAs consumption varies from 1.98 g/day in women to 2.40 g/day in men [75]. France was listed in front of most investigated North European countries such as Island (4.1–6.7 g/day women–men) or Norway (3.2–4.8 g/day women–men), but under South European countries such as Italy (1.6 g/day) or Greece (1.2–1.7 g/day women–men) [9, 75]. Interestingly, the average TFAs consumption in Denmark was much lower than in France (1.1 g/day) [75], certainly because of its efficient governmental legislation. Worldwide TFAs consumption analysis showed that North American countries (USA and Canada) were on the top list of TFAs-consuming countries [75]. Indeed, the TFAs intake in US Americans varied between 4.6 and 8.3 g/day on average [75], which was quite similar to the one in Canadians which varied between 3.8 and 8.4 g/day on average [75].
Nevertheless, comparison and interpretation of TFA levels between populations at a given time period are globally difficult since the cohort study protocols were not strictly standardized (e.g. lack of adjustment parameters). The minimization of daily intake of deleterious TFAs and SFAs as well as the sufficient consumption of cis-UFAs (i.e. omega-3 known to present health benefits such as lowering LDL cholesterol) shall be anyway encouraged worldwide, and particularly in France (Fig. 3).

Schematic representation of the interrelations between TFAs and health status. Briefly, TFAs can originate from three known sources (natural, industrial and technological/domestic). Once overproduced or overconsumed (arrow symbols as marking activation), most TFAs may cause deleterious effects on health such as potentially increasing the risk of cardiovascular diseases (CVDs) by concomitantly reducing the HDL levels and stimulating the LDL production in the blood, which can be targeted by cholesterol-lowering drugs such as statins, albeit the role of cholesterol in the cardiovascular physiopathology remains controversial. Eventually, efficient prevention (e.g. information on TFAs, personalized nutritional chart, quick blood test, longitudinal follow-up of patients, etc.) and novel therapy strategies (hammer symbols marking inhibition or blockade) against TFAs might be then required
Potential effects of TFAs on health
Most TFAs—with the exception of some CLAs which, at moderate doses, would present some therapeutic benefits [38]—can negatively affect the human health and so be involved in several chronic pathologies and biological processes.
TFAs and cardiovascular diseases
Cardiovascular diseases (CVDs) are known to be the first cause of human death worldwide [80]. Importantly, arterial hypertension is considered as one of the major risk factors for both CVD (about 50 %) and death [80]. Several epidemiologic and experimental studies underlines the preponderant role of high levels of cholesterol low-density lipoproteins (C-LDL or “bad cholesterol”) and low levels of cholesterol high-density lipoproteins (C-HDL or “good cholesterol”) on atherogenesis and its consequences [81–84].
However, there is increasing consensus that dietary fats can also affect the CVDs risk via factors other than C-LDL and C-HDL [85, 86]. Thereby, in vivo modulating factors such as TFAs [87], triglycerides [88], homocysteine [89], lipoprotein(a) [90] and plasminogen activator inhibitor-1 (PAI-1) [91] and clotting factors such as FVII [92] when relatively increased, as well as a natural anticoagulants when significantly decreased, appear to be important to better explain the etiology of CVDs and their complications.
Interestingly, most retrospective case–control and prospective cohort studies reported positive associations, even after adjustments of confusion factors (e.g. smoking, age, obesity and high blood pressure), between a relatively high consumption of TFAs (>3 g/day) and the risk to develop CVDs [11, 13, 93–103]. In fact, TFAs consumption corresponding to 2 % TEI can increase the cardiovascular risk of 25 % [15], suggesting that the threshold of 2 % TEI should not be considered as an acceptable reference by competent authorities. That is certainly one of the reasons why the 2004 WHO Global Strategy on Diet, Physical Activity and Health has subsequently recommended an intake of TFAs lower than 1 % TEI [25]. The respect of 1 % TEI is applied in many countries, ruminant fats being a more important source than industrially partially hydrogenated fats.
Mechanistically, TFAs could represent a strong risk factor in the development of CVDs by molecular mechanisms involving (1) increase in plasmatic cholesteryl ester transfer protein (CETP) activity [104, 105]; (2) increase in C-LDL level [106–109]; (3) decrease in C-HDL levels [106–109]; (4) stimulation of pro-inflammatory molecules [e.g. tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), C-reactive protein (C-RP)] [110, 111]; and (5) endothelial dysfunction [110, 111].
Interestingly, TFAs [e.g. vaccenic acid (18:1 11t)] would be, consequently, more atherogenic than SFAs (e.g. palmitic acid, 16:0) which increased both C-LDL and C-HDL [107].
Eventually, although the importance of C-LDL and C-LDL/C-HDL ratio is relatively debated to explain the etiology of CVDs, the implication of TFAs in the development of CVDs appears prominent and thus TFAs should be considered as preventive and therapeutic targets (Fig. 3).
TFAs and other possible health effects
TFAs and metabolic disorders
Most TFAs can be considered as modifiable dietary risk factors for metabolic syndrome, diabetes mellitus (aka type 2 diabetes or T2D) and obesity.
Indeed, relatively high TFAs intake can cause metabolic dysfunction in humans: It can adversely affect circulating lipid levels, trigger systemic inflammation, induce endothelial dysfunction and increase visceral adiposity, body weight as well as insulin resistance (i.e. low insulin sensitivity) [112–115]. The mechanisms behind such effects are unclear, but could involve several possible components such as altered physiochemical membrane properties, fuel partitioning (via altered fat oxidation and carbohydrate oxidation) or altered gene expression [116].
However, rodent studies suggested that supplementation of a CLA mixture (18:2 9c, 11t and 18:2 10t, 12c) could be beneficial for the management of insulin resistance, reduce the corporal fat mass and improve the lipid metabolism, whereas 18:2 10t, 12c alone was associated with greater insulin resistance [117]. In humans, the CLA isomers, 18:2 9c, 11t and 18:2 10t, 12c, have opposite effects with regard to the total cholesterol/c-HDL ratio. Thereby, 18:2 9c, 11t would have a beneficial effect, while 18:2 10t, 12c would have a deleterious effect translated by an increase in insulin resistance in obese individuals presenting a metabolic syndrome [118].
Nevertheless, relatively high consumption of CLAs does not prevent obesity. Indeed, it has been shown that daily consumption of a drinkable dairy product containing up to 3 g of CLA isomers for 18 weeks had no statistically significant effect on body composition in overweight, middle-aged men and women [119].
Eventually, the lack of longitudinal and dose-effects studies does not allow us to clearly conclude about the importance of TFAs and CLAs.
TFAs and cancers
High content of TFAs was associated with an increased risk of cancers, mainly human breast and colorectal cancers [120–122]. However, other studies reported no increase in the rate of those cancers when greater intake of dietary fat and fat subtypes, including TFAs, was consumed, at least among older and postmenopaused women [123, 124]. Interestingly, experimental studies suggest promising effects of some CLAs (e.g. 18:2 9c, 11t) on cancer risk in animal models and in breast cancer cells [125–127]. However, these effects have, until now, not been confirmed in humans.
Taken together, TFAs may be associated with the risk of some cancers. Nevertheless, further studies are still definitively required to solidify this hypothesis. Indeed, method limitations as well as lack of some experimental considerations could explain bias and contradictory results. In the benefice of doubts, the precautionary principle to limit TFAs consumption should be applied.
TFAs and teratogeny: from mother to early infant development and lactation
TFAs ingestion by pregnant women could affect the fetal development due to the presence of TFAs in the maternal milk and their transplacental passage [128, 129].
Indeed, while some 18:2 CLA trans-isomers (e.g. 18:2 9t,12c) are overrepresented in umbilical plasma, 18:1 trans-isomers (e.g. 18:1 9t) were predominantly found in maternal plasma [130]. Since the TFAs composition in human milk fat was mainly represented by oleic acid 18:1 isomers (range: ∆9–12t) and an inverse relation between the weight at birth and the elaidic acid (18:1 9t) level was observed in premature babies, the occurrence of a transplacental passage of elaidic acid was strongly suggested [131]. Furthermore, it has been shown that newborns with low venous umbilical DHA levels and high levels of umbilical TFAs had poor neurologic conditions at 18 months [132]. Overall, it is now admitted that poor maternal DHA status can affect infant’s brain and retinal development [133].
Mechanistically, TFAs transported across the placenta and secreted in human milk in amounts that depend on the maternal dietary intake may have adverse effects on infant growth and development through interfering with essential FA metabolism, direct effects on membrane structures or metabolism or secondary to reduce the intakes of the cis essential FAs in either mother or child [134].
Overall, those limited data point out the risk for pregnant and breast-feeding mothers to consume industrial TFA-containing products, while consumption of essential FAs such as the omega-3 DHA would be largely beneficial.
Policies about TFAs content in France
Regulation
In 2005, the French AFSSA’s report suggested that in a given product (e.g. table oils, shortenings), TFAs should not exceed 1 g/100 g (0.4 % TEI) [75]. Furthermore, AFSSA advised the consumers to reduce their consumption of 30 % in TFA-enriched foods (e.g. pastries, industrial bread products, chocolate bars) because of their low nutritional value [75–77]. To be consistent with the decline in consumption of these products, the agency encouraged manufacturers of margarine and fats for the food sector to reduce TFAs content of their products [75–77].
Nevertheless, in spite of the awareness of the problem, the AFSSA’s suggestions and recommendations are not fully transparent to the consumers and cannot be correctly applied unless legal, firm and concrete procedures (e.g. limitation of TFAs content in manufactured/industrial products, banning of TFAs use in restaurants and in packaged foods and mediatization of the TFAs-related health risks). Yet, international policies could be used as a reference to efficiently reduce TFAs in foods, inform and prevent the French population against potential deleterious TFAs-associated health effects [135].
Thereby and comparatively, Denmark and Switzerland were the first European countries in 2003 and 2008, respectively, to promptly introduce a legal regulation to limit the TFAs content in foods, based on a publication reporting the risk of coronary heart disease and TFAs consumption [136] as well as on the Danish Nutritional Council (DNC) scientific reports [137, 138]. Thereby, along with The Danish Ministry of Food and Agriculture, the Danish Order on TFA imposed a maximum of 2 g TFA/100 g (0.8 % TEI) of oils or fats destined for human consumption [138]. Later, the undertaken regulation also limited products claimed to be “free from TFAs” to <1 g TFA/100 g (0.4 % TEI) in the oil or fat used for production [139]. In USA, some cities and states, such as New York and California, decided to regulate TFAs independently of the national action. By 2008, New York’s Board of Health successfully removed and prevent fats containing TFAs in restaurants [140–142].
Mandatory labeling
In 2005, the AFSSA’s report recommended labeling only when thresholds are exceeded from the standards of the current food supply [75]. Consequently, manufacturers were likely encouraged to improve the composition of their products at some points, but the lack of information on TFAs content and mandatory accessible labeling on any food product—that does or not exceed the regulated threshold—was and is still far from helping customers to reduce their TFAs consumption.
Comparatively, Canada was the first country to regulate mandatory food labeling in 2002, which ordered in 2005 that food labels separately list the amount of TFAs and SFAs for most pre-packaged foods, including products with <0.2 g TFAs per serving which could be labeled as “TFAs free” [143]. This labeling regulation, together with the Task Force Action and the published “Transfat monitoring program,” has been successful in stimulating food manufacturers to reduce or eliminate TFAs [143]. In the USA, along with the important help of the Center for Science in the Public Interest (CSPINET) [144], the FDA final ruling of 2003 required mandatory food labeling mentioning the amount of TFAs [145], although it did not specify maximum allowable limits or approve claims such as “TFAs free” due to concerns of trace amounts adding up with increasing servings. Thereby, food manufacturers were prompted to make product changes [146]. Interestingly, Brazil and Argentina are examples of middle-income countries that have seen changes in TFAs content of food, in part due to the agricultural trade agreement MERCOSUR (the South American Common Market integrated by Argentina, Brazil, Paraguay and Uruguay) in 2003 to mandate labeling which specified amount of TFAs on pre-packaged foods [147]. This initiative induced some food industries to switch from partially hydrogenated oils (aka PVHO) to non-hydrogenated unsaturated oils at no additional costs to consumers because being “trans free” was seen as a competitive advantage [148].
Voluntary industrial initiatives
From the second half of the 1990s which marked the discovery and confirmation of adverse effects of TFAs, TFA intake went down significantly. This was mainly due to voluntary changes in oil processing by the food industry. Indeed, many international food manufacturers and retailers (e.g. Unilever) have voluntarily removed TFAs from their products (e.g. margarines and spreads) [149], triggered by media coverage that TFAs were unhealthier than SFAs [150].
Contrarily to France, where alternatives to reduce the use of industrial TFAs have only been suggested [75–77], some European countries, such as the Netherlands, have successfully relied on voluntary agreements with the food industry [151]. In the UK, the British Retail Consortium announced that major retailers (e.g. some supermarket chains) were committed to remove TFAs from all branded products, and by December 2007, the Food Standards Agency (FSA) claimed that voluntary measures to reduce TFAs had already resulted in safe levels of consumer intake [152]. In the USA, a task force with representation of various stakeholders played an important role in pressuring the food industry to effectively remove TFAs from the food supply without government regulations or involvement [153]. Eventually, in South Korea and Argentina, novel public–private business partnerships between academics and industrials have led to the production of healthier and cost-effective fats or oils, stimulating the food industry to replace TFAs in food manufacturing [135]. Furthermore, in Costa Rica, the industry voluntarily decreased TFAs content in their oils (e.g. soybean oil) which consequently reduced the risk of myocardial infarction in his population, in spite of lack of food labeling and TFAs content regulation [154, 155].
Conclusion
There is abundant evidence that TFAs—with perhaps the exception of some CLAs—have deleterious effects on health. The question whether ruminant TFAs have the same effect, also in the long term, on human diseases risk as industrial TFA has not definitively been settled. The most convincing studies have shown that TFAs represent an independent risk factor for CVDs, a group of non-communicating diseases which lead to the highest rates of mortality worldwide. One of the major explanations of such risk on health is that TFAs consumption concomitantly raises LDL cholesterol levels and reduces HDL cholesterol levels, the later representing an additional negative effect comparatively to SFA. Overall, TFAs intake should be largely prevented by different sanitary and legal dispositions (e.g. media coverage; regulations on food content, labeling and marketing; replacement of poor nutritional oils by healthy fats; fiscal measures; and quick blood test). In France, policy makers—along with the public health sector and other competent authorities—shall be enough stimulated to improve dietary intake behavior (notably to lower TFAs) and health outcomes of individuals, without compromising meanwhile the quality and the price of a given product.
Abbreviations
- AFSSA:
-
Agence Française Sanitaire et Sociale des Aliments
- Ag-TLC:
-
Silver nitrate thin-layer chromatography
- CLA:
-
Conjugated linoleic acid
- DHA:
-
Docosahexaenoic acid
- EPA:
-
Eicosapentaenoic acid
- FA:
-
Fatty acid
- FDA:
-
Food and Drug Administration
- FTIR–ATR:
-
Fourier transform infrared spectroscopy–attenuated total reflection
- GC:
-
Gas chromatography
- g/d:
-
Gram per day
- LDL:
-
Low-density lipoprotein
- HDL:
-
High-density lipoprotein
- HPLC:
-
High-pressure liquid chromatography
- MUFA:
-
Mono-unsaturated fatty acid
- PHVO:
-
Partially hydrogenated vegetable oils
- PUFA:
-
Poly-unsaturated fatty acid
- SFA:
-
Saturated fatty acid
- TFA:
-
Trans-fatty acid
References
Brouwer IA, Wanders AJ, Katan MB (2010) Effect of animal and industrial trans fatty acids on HDL and LDL cholesterol levels in humans—a quantitative review. PLoS ONE 5:e9434
Sommerfeld M (1983) Trans unsaturated fatty acids in natural products and processed foods. Prog Lipid Res 22:221–233
Ledoux M, Rouzeau A, Sauvant D, Bas P (2002) Occurrence of trans-C18:1 fatty acid isomers in goat milk: effect of two dietary regimens. J Dairy Sci 85:190–197
Aro A, Antoine JM, Pizzoferrato L, Reykdal O, Van Poppel G (1998) Trans fatty acids in dairy and meat products from 14 European countries: the TRANSFAIR Study. J Food Compos Anal 11:150–160
Turpeinen AM, Mutanen M, Aro A, Salminen I, Basu S, Palmquist DL, Griinari JM (2002) Bioconversion of vaccenic acid to conjugated linoleic acid in humans. Am J Clin Nutr 76:504–510
Wolff RL, Combe NA, Destaillats F, Boué C, Precht D, Molkentin J, Entressangles B (2000) Follow-up of the D4 to D16 trans-18:1 isomer profile and content in French Processed foods containing partially hydrogenated vegetable oils during the period 1995–1999. Analytical and nutritional implications. Lipids 35:815–825
Ratnayake WM, Galli C (2009) Fat and fatty acid terminology, methods of analysis and fat digestion and metabolism: a background review paper. Ann Nutr Metab 55:8–43
Saguy IS, Dana D (2003) Integrated approach to deep fat frying: engineering, nutrition, health and consumer aspects I. J Food Eng 56:3143–3152
Hulshof KF, van Erp-Baart MA, Anttolainen M, Becker W, Church SM, Couet C, Hermann-Kunz E, Kesteloot H, Leth T, Martins I, Moreiras O, Moschandreas J, Pizzoferrato L, Rimestad AH, Thorgeirsdottir H, van Amelsvoort JM, Aro A, Kafatos AG, Lanzmann-Petithory D, van Poppel G (1999) Intake of fatty acids in western Europe with emphasis on trans fatty acids: the TRANSFAIR Study. Eur J Clin Nutr 53:143–157
American Heart Association Nutrition Committee, Lichtenstein AH, Appel LJ, Brands M, Carnethon M, Daniels S, Franch HA, Franklin B, Kris-Etherton P, Harris WS, Howard B, Karanja N, Lefevre M, Rudel L, Sacks F, Van Horn L, Winston M, Wylie-Rosett J (2006) Diet and lifestyle recommendations revision 2006: a scientific statement from the American Heart Association Nutrition Committee. Circulation 114:82–96
Ascherio A, Hennekens CH, Buring JE, Master C, Stampfer MJ, Willett WC (1994) Trans-fatty acids intake and risk of myocardial infarction. Circulation 89:94–101
Pietinen P, Ascherio A, Korhonen P, Hartman AM, Willett WC, Albanes D, Virtamo J (1997) Intake of fatty acids and risk of coronary heart disease in a cohort of Finnish men. The Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Am J Epidemiol 145:876–887
Jakobsen MU, Overvad K, Dyerberg J, Heitmann BL (2008) Intake of ruminant trans fatty acids and risk of coronary heart disease. Int J Epidemiol 37:173–182
Willett WC, Stampfer MJ, Manson JE, Colditz GA, Speizer FE, Rosner BA, Sampson LA, Hennekens CH (1993) Intake of trans fatty acids and risk of coronary heart disease among women. Lancet 341:581–585
Oomen CM, Ocké MC, Feskens EJ, van Erp-Baart MA, Kok FJ, Kromhout D (2001) Association between trans fatty acid intake and 10-year risk of coronary heart disease in the Zutphen Elderly Study: a prospective population-based study. Lancet 357:746–751
Thompson AK, Minihane AM, Williams CM (2011) Trans fatty acids and weight gain. Int J Obes (Lond) 35:315–324
Smith BK, Robinson LE, Nam R, Ma DW (2009) Trans-fatty acids and cancer: a mini-review. Br J Nutr 102:1254–1266
Mozaffarian D, Katan MB, Ascherio A, Stampfer MJ, Willett WC (2006) Trans fatty acids and cardiovascular disease. N Engl J Med 354:1601–1613
Almendingen K, Jordal O, Kierulf P, Sandstad B, Pedersen JI (1995) Effects of partially hydrogenated fish oil, partially hydrogenated soybean oil, and butter on serum lipoproteins and Lp[a] in men. J Lipid Res 36:1370–1384
Müller H, Jordal O, Seljeflot I, Kierulf P, Kirkhus B, Ledsaak O, Pedersen JI (1998) Effect on plasma lipids and lipoproteins of replacing partially hydrogenated fish oil with vegetable fat in margarine. Br J Nutr 80:243–251
Vermunt SH, Beaufrère B, Riemersma RA, Sébédio JL, Chardigny JM, Mensink RP, TransLinE Study (2001) Dietary trans alpha-linolenic acid from deodorised rapeseed oil and plasma lipids and lipoproteins in healthy men: the TransLinE Study. Br J Nutr 85:387–392
Bhattacharya A, Banu J, Rahman M, Causey J, Fernandes G (2006) Biological effects of conjugated linoleic acids in health and disease. J Nutr Biochem 17:789–810
Whigham LD, Watras AC, Schoeller DA (2007) Efficacy of conjugated linoleic acid for reducing fat mass: a meta-analysis in humans. Am J Clin Nutr 85:1203–1211
World Health Organization (2004) Global strategy on diet, physical activity and health. WHO, Geneva
Nishida C, Uauy R, Kumanyika S, Shetty P (2004) The Joint WHO/FAO Expert Consultation on diet, nutrition and the prevention of chronic diseases: process, product and policy implications. Public Health Nutr 7:245–250
PAHO/WHO Task Force (2007) Trans fats free Americas. Conclusions and Recommendations. Pan American Health Organization, Washington, DC
[No authors listed] (1978) The nomenclature of lipids (Recommendations 1976) IUPAC-IUB Commission on Biochemical nomenclature. Biochem J 171(1):21–35
Fahy E, Subramaniam S, Murphy RC, Nishijima M, Raetz CR, Shimizu T, Spener F, van Meer G, Wakelam MJ, Dennis EA (2009) Update of the LIPID MAPS comprehensive classification system for lipids. J Lipid Res 50:S9–S14
Graber R, Sumida C, Nunez EA (1994) Fatty acids and cell signal transduction. J Lipid Mediat Cell Signal 9:91–116
Woollett LA, Spady DK, Dietschy JM (1992) Saturated and unsaturated fatty acids independently regulate low density lipoprotein receptor activity and production rate. J Lipid Res 33:77–88
Yaqoob P (2003) Fatty acids as gatekeepers of immune cell regulation. Trends Immunol 24:639–645
Neitzel JJ (2010) Fatty acid molecules: fundamentals and role in signaling. Nat Educ 3:57
Davidson BC, Cantrill RC (1985) Fatty acid nomenclature. A short review. S Afr Med J 67:633–634
Lobb K, Chow CK (2007) Fatty acid classification and nomenclature. In: Chow CK (ed) Fatty acids in foods and their health implications, 3rd edn. CRC Press, New York, pp 1–15
Holman RT (1998) The slow discovery of the importance of omega 3 essential fatty acids in human health. J Nutr 128:427S–433S
Holman RT (1964) Nutritional and metabolic interrelationships between fatty acids. Fed Proc 23:1062–1067
Sébédio JL (2007) Acides gras trans: nature, origine et impact sur la santé. Cah Nutr Diet 42:239–245
Dobson G (2002) Analysis of fatty acids in functional foods with emphasis on ω3 fatty acids and conjugated linoleic acid. In: Hurst WJ (ed) Methods of analysis for functional foods and nutraceuticals. CRC Press, New York
Handbook of Chemistry and Physics (2007) Section 7: Biochemistry. In: Taylor and Francis Group, LLC, 88th edn
Mosley EE, Wright AL, McGuire MK, McGuire MA (2005) Trans fatty acids in milk produced by women in the United States. Am J Clin Nutr 82:1292–1297
Kraft J, Hanske L, Möckel P, Zimmermann S, Härtl A, Kramer JK, Jahreis G (2006) The conversion efficiency of trans-11 and trans-12 18:1 by Delta9-desaturation differs in rats. J Nutr 136:1209–1214
Griinari JM, Corl BA, Lacy SH, Chouinard PY, Nurmela KVV, Bauman DE (2000) Conjugated linoleic acid is synthesized endogenously in lactating dairy cows by D9-desaturase. J Nutr 130:2285–2291
Chilliard Y, Ferlay A, Doreau M (2001) Contrôle de la qualité nutritionnelle des matières grasses du lait par l’alimentation des vaches laitières: acides gras trans polyinsaturés, acide linoléique conjugué. INRA Prod Anim 14:323–335
Griinari JM, Bauman DE (1999) Biosynthesis of conjugated linoleic acid and its incorporation into meat and milk in ruminants. In: Yurawecz MP, Mossoba MM, Kramer JKG, Pariza MW, Nelson GJ (eds) Advances in conjugated linoleic acid research. AOCS Press, Champaign, pp 180–200
Precht D (1995) Variation of trans fatty acids in milk fats. Z Ernährungswiss 34:27–29
Ledoux M, Laloux L, Sauvant D (2000) Les isomères trans des acides gras: origine et présence dans l’alimentation. Sci Alim 20:393–411
Chilliard Y, Ferlay A, Rouel J, Lamberet G (2003) A review of nutritional and physiological factors affecting goat milk lipid synthesis and lipolysis. J Dairy Sci 86:1751–1770
Lucas A, Agabriel C, Martin B, Ferlay A, Verdier-Metz I, Coulon JB, Rock E (2006) Relationships between the conditions of cow’s milk production and the contents of components of nutritional interest in raw milk farmhouse cheese. Lait 86:177–202
de Heredia FP, Larque E, Del Puy Portillo M, Canteras M, Zamora S, Garaulet M (2008) Age-related changes in fatty acids from different adipose depots in rat and their association with adiposity and insulin. Nutrition 24:1013–1022
Sabatier P (1966) The Nobel Prize in Chemistry 1912. Nobel Lectures, Chemistry, 1901–1921. Elsevier. Nobel Foundation http://www.nobelprize.org/nobel_prizes/chemistry/laureates/1912/
Normann W (1903) Process for converting unsaturated fatty acids or their glycerides into saturated compounds. DE patent 141029 and GB patent 190301515
Perkins AG, Smick C (1987) Octadecatrienoic fatty acid isomers of partially hydrogenated soybean oil. J Am Oil Chem Soc 64:1150–1155
Brühl L (1995) Determination of trans fatty acids in cold pressed oils. Eur J Med Res 1:89–93
San Juan PMF (1996) Study of isomeric trans fatty acids content in the commercial Spanish food. Int J Food Sci Nutr 47:399–403
Precht D, Molkentin J (2000) Recent trends in the fatty acid composition of German sunflower margarines, shortenings and cooking fats with emphasis on individual C16:1, C18:1, C18:2, C18:3 and C20:1 trans isomers. Nahrung 44:222–228
Henninger M, Ulberth F (1996) Trans fatty acids in margarines and shortenings marketed in Austria. Z Lebensm Unters Forsch 203:210–215
Ackman RG, Mag TK (1998) Trans fatty acids and the potential for less in technical products. In: Sebedio JL, Christie WW (eds) Trans fatty acids in human nutrition. The Oily Press, Dundee, pp 35–58
Ratnayake WMN, Pelletier G, Hollywood R, Bacler S, Leyle D (1998) Trans fatty acids in Canadian margarines: recent trends. J Am Oil Chem Soc 75:1587–1594
Ackman RG, Hooper SN, Hooper DL (1974) Linolenic acid artefacts from the deodorization of oils. J Am Oil Chem Soc 51:42–49
Sébédio JL, Grandgirard A, Prevost J (1988) Linoleic acid isomers in heat treated sunflower oils. J Am Oil Chem Soc 65:362–366
Devinat G, Scamaroni L, Naudet M (1980) Isomerisation de l’acide linolenique durant la desodorisaton des huiles de colza et de soja. Rev Franç Corps Gras 27:283–287
Shantha NC, Ram LN, O’Leary J, Hicks CL, Decker EA (1995) Conjugated linoleic acid concentrations in dairy products as affected by processing and storage. J Food Sci 60:695–697
Rodríguez-Alcalá LM, García-Martínez MC, Cachón F, Marmesat S, Alonso L, Márquez-Ruiz G, Fontecha J (2007) Changes in the lipid composition of powdered infant formulas during long-term storage. J Agric Food Chem 55:6533–6538
Ratnayake WMN (2004) Overview of methods for the determination of trans fatty acids by gas chromatography, silver-ion thin-layer chromatography, silver-ion liquid chromatography, and gas chromatography/mass spectrometry. J AOAC Int 87:523–529
Ackman RG (2008) Application of gas-liquid chromatography to lipid separation and analysis: Qualitative and quantitative analysis. In: Chow CK (ed) Fatty acids in foods and their health implications. CRC Press, London, pp 47–65
Mossoba MM, Yurawecz MP, Delmonte P, Kramer KG (2004) Overview of infrared methodologies for trans fat determination. J AOAC Int 87:540–544
Ratnayake WMN, Hansen SL, Kennedy MP (2006) Evaluation of the CP-Sil 88 and SP-2560 GC columns used in the recently approved AOCS Official Method Ce 1 h–05: determination of cis-, trans-, saturated, monounsaturated and polyunsaturated fatty acids in vegetable or non-ruminant animal oils and fats by capillary GLC method. J Am Oil Chem Soc 83:475–488
AOCS official method Ce 1 h-05 (2005) Determination of cis-, trans-, saturated, monounsaturated and polyunsaturated fatty acids in vegetable or non-ruminant animal oils and fats by capillary GLC method. In: Official Methods and Recommended Practices of the AOCS, 5th edn. Urbana, American Oil Chemists’ Society
AOAC Official Method 996.06 (2001). Fat (total, saturated, and unsaturated) in foods, hydrolytic extraction gas chromatographic method. In: Horwitz W (ed) Official Methods of Analysis of AOAC International, 18th edn. Gaithersburg, AOAC
Volatier JL, Verger P (1999) Recent national French food and nutrient intake data. Br J Nutr 81:S57–S59
Bertail P, Boizot C, Combris P (1993) La consommation alimentaire en 1991, distribution des quantités consommées à domicile, INRA ESR Ivry
Favier JC, Ireland-Ripert J, Toque C, Feinberg M (1996) Répertoire général des aliments, table de composition, CNEVA. CIQUAL. Tec & Doc Lavoisier, Paris
Thiebaut AC, Clavel-Chapelon F (2001) Fat consumption and breast cancer: preliminary results from the E3NEpic cohort. Bull Cancer 88:954–958
Combe N, Boue C, Entressangles B (2000) Consumption of trans fatty acids and cardiovascular risks: aquitaine survey (France). Oléagineux Corps gras Lipides 7:30–34
AFSSA (Agence Française de Sécurité Sanitaire des Aliments) (2005) Risques et bénéfices pour la santé des acides gras trans apportés par les aliments. Recommandations (Rapport), p 217
AFSSA (Agence Française de Sécurité Sanitaire des Aliments). http://www.anses.fr/
AFSSA (Agence Française de Sécurité Sanitaire des Aliments) (2009) Avis de l’Agence française de sécurité sanitaire des aliments sur l′estimation des apports em acides grãs trans de la population française. Saisine n° 2007-SA-0220
Rigaud D, Giachetti I, Deheeger M, Borys JM, Volatier JL, Lemoine A, Cassuto DA (1997) Enquête française de consommation alimentaire I. Energie Macro-nutr Cah Nutr Diét 32:379–389
Boué C, Combe N, Billeaud C, Mignerot C, Entressangles B, Thery G, Geoffrion H, Brun JL, Dallay D, Leng JJ (2000) Trans fatty acids in adipose tissue of French women in relation to their dietary sources. Lipids 35:561–566
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL (2006) Global burden of disease and risk factors. The World Bank and Oxford University Press, Oxford, p 469
Steinberg D, Gotto AM Jr (1999) Preventing coronary artery disease by lowering cholesterol levels: fifty years from bench to bedside. JAMA 282:2043–2050
Genest J Jr, Cohn JS (1999) Epidemiological evidence linking plasma lipoprotein disorders to atherosclerosis and other diseases. In: Barter PJ, Rye KA (eds) Plasma Lipids and their role in disease. Taylor and Francis, London, pp 46–48
Hodis NN, Mack WJ (1998) Triglyceride-rich lipoproteins and progression of atherosclerosis. Eur Heart J 19:40–44
Chapman MJ (1999) Atherogenicity of low density lipoprotein: mechanisms. In: Barter PJ, Rye KA (eds) Plasma lipids and their role in disease. Taylor and Francis, London
de Lorgeril M (2008) Cholestérol, mensonges et propagande. Thierry Souccar Editions, p 317
Ravnskov U (2000) The cholesterol myths. New Trends Publishing, Washington, DC
Bassett CM, McCullough RS, Edel AL, Maddaford TG, Dibrov E, Blackwood DP, Austria JA, Pierce GN (2009) Trans-fatty acids in the diet stimulate atherosclerosis. Metabolism 58:1802–1808
McColl MD, Sattar N, Ellison J, Tait RC, Walker ID, Packard CJ, Greer IA (2000) Lipoprotein (a), cholesterol and triglycerides in women with venous thromboembolism. Blood Coagul Fibrinolysis 11:225–229
Hankey GJ, Eikelboom JW (1999) Homocysteine and vascular disease. Lancet 354:407–413
Loscalzo J (1990) Lipoprotein(a). A unique risk factor for atherothrombotic disease. Arteriosclerosis 10:672–679
Kohler HP, Grant PJ (2000) Plasminogen-activator inhibitor type 1 and coronary artery disease. N Engl J Med 342:1792–1801
Junker R, Heinrich J, Schulte H, van de Loo J, Assmann G (1997) Coagulation factor VII and the risk of coronary heart disease in healthy men. Arterioscler Thromb Vasc Biol 17:1539–1544
Mozaffarian D, Aro A, Willett WC (2009) Health effects of trans-fatty acids: experimental and observational evidence. Eur J Clin Nutr 63:S5–S21
Ascherio P, Rimm EB, Giovannucci EL, Spiegleman D, Stampfer M, Willett WC (1996) Dietery fat and risk of coronary heart disease in men: cohort follow up study in the United States. BMJ 313:84–90
Hu FB, Stampfer MJ, Manson JAE, Rimm E, Colditz GA, Rosner BA, Hennekens CH, Willett WC (1997) Dietary Fat Intake and the Risk of Coronary Heart Disease in Women. N Engl J Med 337:1491–1499
Aro A, Kardinaal AF, Salminen I, Kark JD, Riemersma RA, Delgado-Rodriguez M, Gomez-Aracena J, Huttunen JK, Kohlmeier L, Martin BC et al (1995) Adipose tissue isomeric trans fatty acids and risk of myocardial infarction in nine countries: the EURAMIC study. Lancet 345:273–278
Kromhout D, Menotti A, Bloemberg B, Aravanis C, Blackburn H, Buzina R, Dontas AS, Fidanza F, Giampaoli S, Jansen A et al (1995) Dietary saturated and trans fatty acids and cholesterol and 25-year mortality from coronary heart disease: the Seven Countries Study. Prev Med 24:308–315
Chardigny JM, Chardigny JM, Destaillats F, Malpuech-Brugère C, Moulin J, Bauman DE, Lock AL, Barbano DM, Mensink RP, Bezelgues JB, Chaumont P, Combe N, Cristiani I, Joffre F, German JB, Dionisi F, Boirie Y, Sébédio JL (2008) Do trans fatty acids from industrially produced sources and from natural sources have the same effect on cardiovascular disease risk factors in healthy subjects? Results of the trans Fatty Acids Collaboration (TRANSFACT) study. Am J Clin Nutr 87:558–566
Motard-Bélanger A, Charest A, Grenier G, Paquin P, Chouinard Y, Lemieux S, Couture P, Lamarche B (2008) Study of the effect of trans fatty acids from ruminants on blood lipids and other risk factors for cardiovascular disease. Am J Clin Nutr 87:593–599
Roberts TL, Wood DA, Riemersma RA, Gallagher PJ, Lampe FC (1995) Trans isomers of oleic and linoleic acids in adipose tissue and sudden cardiac death. Lancet 345:278–282
Van de Vijver LP, van Poppel G, van Houwelingen A, Kruyssen DA, Hornstra G (1996) Trans unsaturated fatty acids in plasma phospholipids and coronary heart disease: a case–control study. Atherosclerosis 126:155–161
Fritsche J, Steinhart H, Kardalinos V, Klose G (1998) Contents of trans-fatty acids in human substernal adipose tissue and plasma lipids: relation to angiographically documented coronary heart disease. Eur J Med Res 3:401–416
Van de Vijver LP, Kardinaal AF, Couet C, Aro A, Kafatos A, Steingrimsdottir L, Amorim Cruz JA, Moreiras O, Becker W, van Amelsvoort JM, Vidal-Jessel S, Salminen I, Moschandreas J, Sigfússon N, Martins I, Carbajal A, Ytterfors A, Poppel G (2000) Association between trans fatty acid intake and cardiovascular risk factors in Europe: the TRANSFAIR study. Eur J Clin Nutr 54:126–135
Abbey M, Nestel PJ (1994) Plasma cholesteryl ester transfer activity is increased when trans-elaidic acid is substituted for cis-oleic acid in diet. Atherosclerosis 106:99–107
Van Tol A, Zock PL, Van Gent T, Scheek LM, Katan MB (1995) Dietary trans fatty acids increase serum cholesteryl ester transfer protein activity in man. Atherosclerosis 115:129–134
Mensink R, Katan MB (1990) Effect of dietary trans fatty acids on high density and low density lipoprotein cholesterol levels in healthy subjects. N Engl J Med 323:439–445
Zock PL, Katan MB (1992) Hydrogenation alternatives: effects of trans fatty acids and stearic acid versus linoleic acid on serum lipids and lipoproteins in human. J Lipid Res 33:399–410
Judd JT, Clevidence BA, Muesing RA, Wittes J, Sunkin ME, Podczasy JJ (1994) Dietary trans fatty acids: effects on plasma and lipoproteins of healthy men and women. Am J Clin Nutr 59:861–868
Katan MB, Zock PL, Mensink RP (1995) Trans fatty acids and their effects on lipoproteins in humans. Annu Rev Nutr 15:473–493
Harvey KA, Arnold T, Rasool T, Antalis C, Miller SJ, Siddiqui RA (2008) Trans-fatty acids induce pro-inflammatory responses and endothelial cell dysfunction. Br J Nutr 99:723–731
Mozaffarian D (2006) Trans fatty acids—effects on systemic inflammation and endothelial function. Atheroscler Suppl 7:29–32
Risérus U (2006) Trans fatty acids, insulin sensitivity and type 2 diabetes. Scand J Food Nutr 50:161–165
Micha R, Mozaffarian D (2009) Trans fatty acids: effects on metabolic syndrome, heart disease and diabetes. Nat Rev Endocrinol 5:335–344
Dorfman SE, Laurent D, Gounarides JS, Li X, Mullarkey TL, Rocheford EC, Sari-Sarraf F, Hirsch EA, Hughes TE, Commerford SR (2009) Metabolic implications of dietary trans-fatty acids. Obesity (Silver Spring) 17:1200–1207
Riserus U, Arner P, Brismar K, Vessby B (2002) Treatment with dietary trans 10 cis 12 conjugated linoleic acid causes isomer-specific insulin resistance in obese men with the metabolic syndrome. Diabetes Care 25:1516–1522
Saravanan N, Haseeb A, Ehtesham NZ, Ghafoorunissa AS (2005) Differential effects of dietary saturated and trans fatty acids on expression of genes associated with insulin sensitivity in rat adipose tissue. Eur J Endocrinol 153:159–165
Taylor CG, Zahradka P (2004) Dietary conjugated linoleic acid and insulin sensitivity and resistance in rodent models. Am J Clin Nutr 79:1164S–1168S
Gaullier JM, Halse J, Hoye K, Kristiansen K, Fagerteun H, Vik H, Gudmundsen O (2004) Conjugated linoleic acid supplementation for 1 y reduces body fat mass in healthy overweight humans. Am J Clin Nutr 79:1118–1125
Malpuech-Brugère C, Verboeket-van de Venne WP, Mensink RP, Arnal MA, Morio B, Brandolini M, Saebo A, Lassel TS, Chardigny JM, Sébédio JL, Beaufrère B (2004) Effects of two conjugated linoleic acid isomers on body fat mass in overweight humans. Obes Res 12:591–598
Bakker N, Van’t Veer P, Zock PL, The EURAMIC Study Group (1997) Adipose fatty acids and cancers of the breast, prostate and colon: an ecological study. Int J Cancer 72:587–591
Chajès V, Thiébaut AC, Rotival M, Gauthier E, Maillard V, Boutron-Ruault MC, Joulin V, Lenoir GM, Clavel-Chapelon F (2008) Association between serum trans-monounsaturated fatty acids and breast cancer risk in the E3N-EPIC Study. Am J Epidemiol 167:1312–1320
Slattery ML, Benson J, Ma KN, Potter JD (2001) Trans-fatty acids and colon cancer. Nutr Cancer 39:170–175
Limburg PJ, Liu-Mares W, Vierkant RA, Wang AH, Harnack L, Flood AP, Sellers TA, Cerhan JR (2008) Prospective evaluation of trans-fatty acid intake and colorectal cancer risk in the Iowa Women’s Health Study. Int J Cancer 123:2717–2719
Byrne C, Rockett H, Holmes MD (2002) Dietary fat, fat subtypes, and breast cancer risk: lack of an association among postmenopausal women with no history of benign breast disease. Cancer Epidemiol Biomarkers Prev 11:261–265
Tanmahasamut P, Liu J, Hendry LB, Sidell N (2004) Conjugated linoleic acid block estrogen signalling in human breast cancer cells. J Nutr 134:674–680
Corl BA, Barbano DM, Bauman DE, Ip C (2003) cis-9, trans-11 CLA derived endogenously from trans-11 18:1 reduces cancer risk in rats. J Nutr 33:2893–2900
Degen C, Ecker J, Piegholdt S, Liebisch G, Schmitz G, Jahreis G (2011) Metabolic and growth inhibitory effects of conjugated fatty acids in the cell line HT-29 with special regard to the conversion of t11, t13-CLA. Biochim Biophys Acta 1811(12):1070–1080
Koletzko B, Thiel I, Springer S (1992) Lipids in human milk: a model for infant formulae? Eur J Clin Nutr 46:S45–S55
Carlson SE, Clandinin MT, Cook HW, Emken EA, Filer LJ Jr (1997) Trans fatty acids: infant and fetal development. Am J Clin Nutr 66:715S–736S
Combe N, Judde A, Billeaud C, Boue C, Turon F, Entressangles B, Dallay D, Lengh JJ (1998) Distribution of dietary trans isomers of essential fatty acids in blood lipid classes. In: Riemersma RA, Armstrong RA, Kelly RW, Wilson R (eds) Proceedings of the fourth international congress on essential fatty acids and eicosanoids. Champaign, AOCS Press, pp 239–242
Boué C, Combe N, Billeaud C, Entressangles B (2001) Nutritional implications of trans fatty acids during perinatal period, in French pregnant women. Lipids, fats and oils: opportunities and responsibilities in the New Century. OCL 8:68–72
Bouwstra H, Dijck-Brouwer J, Decsi T, Boehm G, Boersma ER, Muskiet FA, Hadders-Algra M (2006) Neurologic condition of healthy term infants at 18 months: positive association with venous umbilical DHA status and negative association with umbilical trans-fatty acids. Pediatr Res 60:334–339
Innis SM (2007) Fatty acids and early human development. Early Hum Dev 83:761–766
Innis SM (2006) Trans fatty intakes during pregnancy, infancy and early childhood. Atheroscler Suppl 7:17–20
Pérez-Ferrer C, Lock K, Riviera JÁ (2010) Learning from international policies on trans fatty acids to reduce cardiovascular disease in low- and middle-income countries, using Mexico as a case study. Health Policy Plan 25:39–49
Stender S, Dyerberg J (2004) Influence of trans fatty acids on health. Ann Nutr Metab 48:61–66
Stender S, Dyerberg J, Hølmer G, Ovesen L, Sandström B (1995) The influence of trans fatty acids on health: a report from the Danish Nutrition Council. Clin Sci (Lond) 88:375–392
Leth T, Jensen HG, Mikkelsen AA, Bysted A (2006) The effect of the regulation on trans-fatty acid content in Danish food. Atherosclerosis S7:53–56
L’Abbé MR, Stender S, Skeaff CM, Ghafoorunissa, Tavella M (2009) Approaches to removing trans fats from the food supply in industrialized and developing countries. Eur J Clin Nutr 63:S50–S67
Okie S (2007) New York to trans fats: you’re out! N Engl J Med 356:2017–2021
Leake LL (2007) Trans fat to go. Food Technol 61:66–68
California State Assembly (2008) Assembly Bill No. 97. Sacramento, CA
Trans Fat Task Force (2006) Ottawa: Health Canada and Heart and Stroke Foundation of Canada; TRANSforming the Food Supply, Report of the Trans Fat Task Force submitted to the Minister of Health of Canada
CSPINET (Center for Science in the Public Interest). http://www.cspinet.org/
Moss J (2006) Labeling of trans fatty acid content in food, regulations and limits-the FDA view. Atheroscler Suppl 7:57–59
Tarrago-Trani MT, Phillips KM, Lemar LE, Holden JM (2006) New and existing oils and fats used in products with reduced trans-fatty acid content. J Am Diet Assoc 106:867–880
Coutinho JG, Recine E (2007) International experiences with health claims in food labeling. Rev Panam Salud Publica 22:432–437
Valenzuela A, Nieto S, Peterson G, Tavella M (2004) Comparative study in fried food about the stability of different vegetable oils. Fat Oils Mag 2:22–28
Korver O, Katan MB (2006) The elimination of trans fats from spreads: how science helped to turn an industry around. Nutr Rev 64:275–279
Willett WC, Ascherio A (1994) Trans fatty acids: are the effects only marginal? Am J Public Health 84:722–724
Katan MB (2006) Regulation of trans fats: the gap, the Polder, and McDonald’s French fries. Atheroscler Suppl 7:63–66
Food Standards Agency (2007) FSA Board to advise the Department of Heath to maintain successful voluntary approach for trans fats in food. Press release, London
Willett WC (2006) The scientific basis for TFA regulations-is it sufficient? Comments from the USA. Atheroscler Suppl 7:69–71
Colo’n Ramos U, Baylin A, Campos H (2006) The relation between trans fatty acid levels and increased risk of myocardial infarction does not hold at lower levels of trans fatty acids in Costa Rican food supply. J Nutr 136:2887–2892
Baylin A, Kabagambe EK, Ascherio A, Spiegelman D, Campos H (2003) High 18:2 trans-fatty acids in adipose tissue are associated with increased risk of nonfatal acute myocardial infarction in Costa Rican adults. J Nutr 133:1186–1191
The LIPID MAPS–Nature Lipidomics Gateway, http://www.lipidmaps.org/
Fahy E, Sud M, Cotter D, Subramaniam S (2007) LIPID MAPS online tools for lipid research. Nucleic Acids Res 35:W606–W612
Conflict of interest
The authors declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding authors
Additional information
F. Menaa and A. Menaa have equally contributed to this work.
Rights and permissions
About this article
Cite this article
Menaa, F., Menaa, A., Menaa, B. et al. Trans-fatty acids, dangerous bonds for health? A background review paper of their use, consumption, health implications and regulation in France. Eur J Nutr 52, 1289–1302 (2013). https://doi.org/10.1007/s00394-012-0484-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-012-0484-4