
Abstract
Background
Acrylamide is a chemical compound present in tobacco smoke and food, classified as a probable human carcinogen and a known human neurotoxin. Acrylamide is formed in foods, typically carbohydrate-rich and protein-poor plant foods, during high-temperature cooking or other thermal processing. The objectives of this study were to compare dietary estimates of acrylamide from questionnaires (DQ) and 24-h recalls (R) with levels of acrylamide adduct (AA) in haemoglobin.
Methods
In the European Prospective Investigation into Cancer and Nutrition (EPIC) study, acrylamide exposure was assessed in 510 participants from 9 European countries, randomly selected and stratified by age, sex, with equal numbers of never and current smokers. After adjusting for country, alcohol intake, smoking status, number of cigarettes and energy intake, correlation coefficients between various acrylamide measurements were computed, both at the individual and at the aggregate (centre) level.
Results
Individual level correlation coefficient between DQ and R measurements (r DQ,R) was 0.17, while r DQ,AA and r R,AA were 0.08 and 0.06, respectively. In never smokers, r DQ,R, r DQ,AA and r R,AA were 0.19, 0.09 and 0.02, respectively. The correlation coefficients between means of DQ, R and AA measurements at the centre level were larger (r > 0.4).
Conclusions
These findings suggest that estimates of total acrylamide intake based on self-reported diet correlate weakly with biomarker AA Hb levels. Possible explanations are the lack of AA levels to capture dietary acrylamide due to individual differences in the absorption and metabolism of acrylamide, and/or measurement errors in acrylamide from self-reported dietary assessments, thus limiting the possibility to validate acrylamide DQ measurements.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acrylamide is a chemical compound found in tobacco smoke [1] and food [2] and other sources such as occupational exposure, consumer products and textiles [3]. It is a potential human carcinogen and a known human neurotoxin [4]. Acrylamide is formed in foods, typically carbohydrate-rich and protein-poor plant commodities, during cooking or other thermal processing such as frying, baking or roasting at temperatures of 120 °C or higher. Acrylamide’s presence in foods may pose a public health concern.
Exposure to dietary acrylamide is usually assessed through estimates based on self-reported dietary assessments of known acrylamide-containing foods, typically by means of dietary questionnaires (DQ), weighted records or 24-h dietary recalls (R). Assessing dietary exposure to acrylamide is challenging because exposure levels depend heavily on the nature and extent of heat treatment of specific foods. In addition, preparation methods vary between different populations and are particularly difficult to capture with DQs, as these instruments are generally not conceived to collect information about the processing and the cooking methods of consumed foods. In parallel, haemoglobin (Hb) adducts of acrylamide and its primary metabolite glycidamide have been considered biomarkers of acrylamide exposure. These measurements provide information about the amount of acrylamide exposure accumulated during the last 4 months [5].
Although recent evidence suggests that a dose–response relationship exists between dietary acrylamide exposures and Hb adduct levels [6], a number of correlation studies reported mixed results on the relationship between self-reported DQ acrylamide intake and measured Hb adduct levels in humans, the magnitude of correlation coefficients ranging from moderate [7–9] to trivial values [3, 10].
Results of epidemiological studies on the association between dietary acrylamide exposure and risk of various cancer have been reported, with inconclusive findings, often differential to the type of assessments (dietary vs. biomarkers) and the type of cancer investigated [11, 12]. As it is not clear whether the inconsistency of findings are the result of methodological limitations and/or a lack of variability in the exposure or a true lack of association, further epidemiological studies of dietary acrylamide exposure and cancer risk have been recommended [11].
In a subgroup of the European Prospective Investigation into Cancer and Nutrition (EPIC) study [13], Hb adducts of acrylamide and glycidamide were measured [14]. In the current study, acrylamide and glycidamide Hb measurements were compared to dietary levels of acrylamide assessed in DQ and R measurements. Correlation coefficients between different acrylamide measurements were computed, both at the individual and at the aggregate levels, and the main sources of variation were determined and evaluated.
Methods
EPIC is a multicentre cohort study investigating the relation between diet, nutritional and metabolic characteristics, various lifestyle and environmental factors, and the risk of cancer and other chronic diseases among over 500,000 study subjects [13]. Twenty-three research centres in 10 European countries participate in the study. Collection of data and blood samples started in 1992. A subsample of 37,000 participants also provided dietary information by means of a single standardized 24-h dietary recall for calibration purposes [15].
Study population
In this work, the study population, described in detail elsewhere [14], was a random sample of 510 persons from 9 European countries, that is, Denmark (Aarhus and Copenhagen), France, Germany (Heidelberg and Potsdam), Greece, Italy (Northern and Southern centres), the Netherlands, Spain, Sweden (Malmö and Umeå), United Kingdom (Cambridge and Oxford health conscious), as shown in Online Resource 1. The sample was evenly represented by men and women, with the exception of France where women only were selected. Within the groups of men and women, an equal number of smokers and never smokers, based on self-reported questionnaire data, were sampled. Study subjects’ age ranges were 41–60 years in men and 43–60 years in women. The IARC and CDC ethics committees approved the study, and the study was conducted according to the guidelines of the Helsinki declaration. Hb acrylamide and glycidamide were measured in 300 μL of hemolysed erythrocytes and analysed by HPLC/tandem mass spectrometry (HPLC/MS/MS) as described previously [14, 16]. In brief, the N-terminal valines of haemoglobin with acrylamide and glycidamide attached were cleaved from the protein chain using modified Edman reaction with pentafluorophenyl isothiocyanate as Edman reagent [17]. The resulting Edman products (Acrylamide-Val-PFPTH and Glycidamide-Val-PFPTH) were extracted using liquid–liquid extraction and analysed by HPLC/MS/MS. Calibrators, reagent blanks, and quality-control materials were processed the same way as the samples. Two independent measurements per sample were performed. Haemoglobin adduct concentrations were reported relative to the amount of haemoglobin used in the analysis. The detection limits for this method were 3 and 4 pmol/g of Hb for acrylamide and glycidamide, respectively. Blood samples were analysed in a randomized manner to minimize systematic analytical differences between country groups.
Dietary data
Information on habitual dietary intakes was assessed at baseline with different dietary questionnaires (France, the Netherlands, Germany, Greece, and Italy, except Naples), a diet history questionnaire (Spain), a modified diet history methodology combining a quantified dietary frequency questionnaire, a 7-day menu book and a 1-h interview (Malmö, Sweden), or a semi-quantitative food frequency questionnaire (United Kingdom and Naples) developed and validated in each participating country [13]. In addition, a single 24-h dietary recall measurement per subject was collected in EPIC as a reference measurement from a subsample (~ 8 %) of each cohort [15]. In contrast to baseline questionnaires, 24-h dietary recall interviews were standardized across countries using the same structure and interview procedure and a common computer program (EPIC-Soft®, IARC, Lyon, France). More details on the concept of standardization and the structure of EPIC-Soft are described in detail elsewhere [18].
In order to compile a harmonized acrylamide database, values from the EU monitoring database of acrylamide levels in food maintained by the Institute for Reference Materials and Measurements (IRMM) (http://irmm.jrc.ec.europa.eu/activities/acrylamide/Pages/index.aspx) were used. The data included in the IRMM database cover a broad range of food commodities. The data are mainly from official and private food laboratories, including food industry, of Germany, the Netherlands, Ireland, Greece, Italy, Spain and United Kingdom. Acrylamide values for foods not available in this database were completed with analysed data from the US FDA database (e.g. peanut butter) (US Food and Drug Administration 2004) and country-specific databases (Swedish, Dutch, Norwegian, French and German national databases). Details of national contact persons for acrylamide content in food items are available upon request to the Authors. An inventory of all food items occurring in the IRMM database and the additional sources for the 10 countries included in the present study was made and classified according to the EPIC-Soft classification [18]. The DQ items and, when available, its specific description (e.g. ‘potatoes baked’) were matched with the respective foods in the AA database. In general, DQ consumption factors on the proportion of type of cooking methods of a given food (e.g. potatoes) were extrapolated from the distribution of specific food items (e.g. boiled, fried, or roasted potatoes) using nationally available food consumption data. If an exact match was not possible, the item was matched to a mean of all foods of the food group in the AA database. Relevant information on food preparation was available for potatoes (except in Italy), bread, and breaded meat, fish and processed meat. For all countries, the same mean value of acrylamide content was assigned to the corresponding food.
Statistical analyses
Geometric means and inter-decile range (10–90th percentiles) of DQ and R measurements, of Hb acrylamide and glycidamide adduct levels, as well as their ratio (GA/AA), were computed. In an exploratory phase, multivariable regression analyses were used to assess the contribution of a list of factors to the variability of dietary measurements, and of Hb adduct levels (acrylamide, glycidamide and their ratio). Each type of acrylamide measurement was modelled as a function of smoking status (never/current), number of cigarettes, country, age at recruitment, sex, physical activity, weight, level of schooling (None/Primary school/Technical school/Secondary school/Longer education/Not specified), alcohol (g/day), and energy intake (Kcal/day), overall and separately in smokers and never smokers. Models for Hb adducts included the effect of batch. The partial R 2 (R 2partial ) was used to assess, conditional on other independent variables in the model, the relative amount of variability (expressed as a percentage) that each independent variable contributed to explain [19] in acrylamide measurements of, in turn, DQ, R and Hb adduct levels. In addition, R 2total was also determined, as a measure of total variability explained by the ensemble of independent factors on the variability of each acrylamide measurement.
Correlation coefficients between dietary and Hb adduct levels of acrylamide were computed. Crude coefficients were primarily computed, and then adjustment was performed by country, alcohol intake, smoking status, number of cigarettes and energy intake. Adjustment was performed using the residual method, that is, by regressing each type of acrylamide measurement on the specific list of adjustment factors and computing residuals. Correlation coefficients were computed for the whole sample, by smoking status and by sex. Country-specific correlation coefficients were also computed. In addition, means of Hb adduct levels were compared with DQ and R measurements at the aggregate level by computing correlation coefficients using arithmetic centre-specific means. Aggregate-level correlation coefficients were adjusted by the mean of centre-specific energy intake, alcohol intake and number of cigarettes, and weighed by centre-specific sample size.
Consistently in this work, Pearson’s correlation coefficients were computed. The 95 % confidence intervals (CIs) were computed by applying Fisher’s z transformation [20]. In all statistical analyses, acrylamide measurements were log-transformed (natural logarithm). Regression and correlation analyses were conducted using the MIXED and CORR procedures, respectively, of the SAS software, version 9.3 [21].
Results
The design of the EPIC acrylamide measurements validation study is presented in Online Resource 1 by sex and participating country; a total of 510 subjects (50 % never smokers, 50 % smokers) were selected. While self-reported DQ and R means were invariant with respect to smoking status, Hb adduct levels were between two- to threefold higher in smokers, with geometric means equal to 116.5 and 86.7 pmol/g in AA and GA, respectively, compared to never smoker subjects, with means equal to 44.4 and 39.0 pmol/g (Table 1). These large differences are also reflected in the total variation observed in Hb adduct levels, where 10 and 90th percentile values were ranging between 28.1 and 75.4 pmol/g in never smokers, and between 53.8 and 243.8 in smokers. Conversely, the GA/AA ratio showed a similar pattern in never and current smokers.
The analysis of the determinants of self-reported dietary intake and Hb adduct levels of acrylamide (Table 2) indicated that country and energy intake were the most important determinants of dietary acrylamide, in both DQ and R measurements, overall and by smoking status. Statistical models suggested that the ensemble of predictors explained some 66 % of total variability in acrylamide DQ measurements and 28 % in R values. On the other hand, smoking status, and the number of cigarettes smoked in smokers, explained a large proportion of AA and GA–Hb adduct variability, conditional on all other variables in the model. Country was still an important determinant of Hb adduct level. Alcohol intake displayed a value of R 2partial equal to 6.9 and 23.5 % in never smokers and smokers, respectively, for the ratio GA/AA. Large R 2partial values related to alcohol intake were also observed for GA measurements. The total amount of variability explained by the set of independent variables (total R 2) ranged between 29 and 47 % for Hb adduct levels, in smokers or never smokers.
Table 3 shows correlation coefficients between different pair-wise combinations of acrylamide measurements, crude and adjusted. Consistently in almost all comparisons, as expected, adjusted correlation coefficients displayed lower values compared to crude ones. Adjustment for energy intake had an overall small impact on correlation values. The coefficients between DQ and R (r DQ,R) were equal to 0.35 (95 %CI: 0.27, 0.42) and to 0.17 (0.08, 0.25), for crude and adjusted estimates, respectively. Lower correlations were observed between dietary measurements and Hb adduct levels, with values equal to 0.08 (−0.01, 0.17) for r DQ,AA, to 0.06 (−0.03, 0.15) for r R,AA and 0.09 (0.01, 0.18) for r DQ,GA. Overall, correlations displayed similar values according to smoking status, with the exception of r DQ,GA, which was equal to 0.03 (−0.09, 0.15) and 0.14 (0.02, 0.26) in never smokers and smokers, respectively. Values of r DQ,GA/AA displayed rather poor agreement, with values close to zero if not negative. Overall, correlation coefficients were slightly higher in women compared with men. Correlations by country are available as Online Resource 2, overall and by smoking status. Values for r DQ,R and r DQ,AA ranged from −0.02 to 0.28, and from −0.16 to 0.26, respectively. In never smokers, r DQ,R and r DQ,AA ranged from −0.07 to 0.49, and from −0.16 to 0.40, respectively, with a sample size of 30 study subjects in each country.
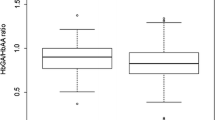
Figure 1 shows geometric means of AA Hb adduct levels according to deciles of DQ acrylamide intake after adjustment for country, energy intake, alcohol intake, number of cigarettes, separately by smoking status. Both groups did not show linear positive relationships.

Geometric meansa (95 % CI)b of acrylamide Hb adducts by decile of DQ acrylamide intake, separately in smokers and never smokers. a Using smoking status–specific residual models, data were adjusted by country, energy intake, alcohol intake and number of cigarettes (in smokers only); b Confidence intervals determined as exp[mean[log(x)] ± 1.96 SE[mean]], where x expresses individual Hb values and exp[mean[log(x)]] is the geometric mean
Estimates of the coefficients obtained at the aggregate level, reported in Table 4, were in general higher than values at the individual level, particularly for values involving R measurements. DQ measurements displayed correlations with R, AA and GA equal to 0.65 (0.18, 0.88), 0.42 (−0.14, 0.78) and 0.32 (−0.25, 0.73), respectively. Aggregate correlations between acrylamide levels based on self-reported assessments, and Hb adducts were rather similar according to smoking status and sex, with the exception of r R,GA, with values larger in smokers than never smokers. Conversely, higher values of r DQ,R were observed in never smokers (0.78: 0.43, 0.93) than smokers (0.48: -0.07, 0.81), and in women (0.88: 0.66, 0.96) compared to men (0.21: −0.36, 0.67).
Discussion
In this study, estimates of acrylamide based on self-reported dietary measurements (i.e. DQ and R) were compared to Hb adduct levels of acrylamide using data collected from 510 participants from 9 countries in the EPIC study. After controlling for a list of covariables, individual level correlation coefficients between DQ and R measurements and Hb adduct levels of acrylamide, and glycidamide, were overall low, both in smokers and never smokers, with correlation values consistently lower than 0.20. Unlike previous observations [9], correlations were of similar magnitude between DQ and the sum of acrylamide and glycidamide Hb levels (data not shown).
Consistent with previous evidence on Hb adducts in the EPIC study [14], dietary measurements of acrylamide varied considerably by country, particularly in DQ. This variation was less apparent in R measurements, possibly because a common standardized methodology using EPIC-Soft across the participating countries was used to collect 24-h dietary recall measurements [18]. Energy intake appeared to be a relevant factor in explaining the observed variability in acrylamide intake, thus suggesting that dietary patterns with acrylamide-rich foods tend to be characterized by large caloric contributions. An evaluation of the major food sources of dietary acrylamide intake in the EPIC study is ongoing [33].
As previously noted, smoking status and alcohol intake are the factors more strongly associated with Hb adducts variability, particularly in glycidamide [14]. While smoking is an important source of overall acrylamide exposure, lower GA–Hb adducts and GA/AA ratios were observed with increasing alcohol intake, which competitively inhibits CYP2E1-mediated metabolism of AA to GA [22]. Glycidamide is an important exposure because, unlike acrylamide, it possessess mutagenic properties [12]. In particular, in evaluating the potential health effects of acrylamide, the exposure balance between acrylamide and glycidamide in the body is of relevance.
One important limitation of haemoglobin adducts of acrylamide as a biomarker of dietary acrylamide exposure is that it reflects a fairly recent period of exposure (up to 3–4 months) and were shown to display large intra-individual variability [23], likely to reflect variations in intake of acrylamide-rich foods, whereas DQ measurements typically assess study participants’ diet over the past year. Given that long-term dietary exposure is more relevant with respect to development of cancer, a single measurement of blood adduct levels may not be sufficient. Furthermore, adducts capture more than one source of acrylamide exposure, not just the dietary component, and they also reflect individual differences in absorption and metabolism. Among others, the extent of passive smoking may well affect the concentration of adduct levels. In general, non-dietary sources of acrylamide Hb adducts seem to be more relevant than previously thought. In this study, correlations were consistently adjusted by smoking status, number of cigarettes smoked and alcohol intake, while no information was available on other potentially relevant factors, including the extent of individuals’ exposure to passive smoking.
Recently published results from an intervention study in humans confirmed that a dose–response relationship exists between dietary acrylamide exposures and Hb adduct levels [6]. It is worthwhile mentioning that acrylamide intake in this intervention study was much higher than intakes observed in usual diets (~5 to 50-fold higher). Furthermore, the acrylamide content of duplicates of foods consumed by participants in the intervention groups were precisely analysed [6], thus the evaluation was carried out in controlled settings. A number of correlation studies reported mixed results on the relationship between dietary acrylamide intake based on self-reported measurements and measured Hb adduct levels in humans. In a small study of 50 Norwegian adults, no correlation between FFQ acrylamide intake and Hb adduct level was observed [10]. In the Malmo Diet and Cancer study, correlation coefficients between dietary acrylamide assessed with a modified diet history and adduct levels from all food sources were 0.43 in non-smokers and 0.36 in smokers [7], although correlations were probably overestimated because participants were enrolled on the basis of high and low intake of acrylamide-containing foods. Weaker correlations of the order of 0.18 and 0.17 in women and men, respectively, were reported in a sample of non-smokers [8], using FFQ and 24-h dietary recall measurements. Slightly larger correlation between FFQ acrylamide intake and Hb adducts were observed in the Nurses’ Health Study II [9], with correlations equal to 0.29 and 0.35 for AA and GA–Hb levels, respectively. In a representative study of the United States with over 3,700 non-smoking subjects (three years of age and older), a low correlation between dietary acrylamide intake estimates and AA and GA–Hb adducts was found (r = 0.10) [3].
Among the possible explanations for the low correlation observed between dietary acrylamide and Hb in this and other published studies, it could be worth to mention the following, in addition to the already mentioned limitations of Hb measurements. Dietary assessment instruments group multiple foods with varying acrylamide content into single items, whereas acrylamide content could vary substantially even within single foods, with respect to cooking method, cooking time, brand and others aspects of food preparation practices, for whom information is seldom available. Moreover, important information on the extent of cooking or heat treatment of both at home and commercially prepared foods was lacking in our study as in many other observational studies. Further, the acrylamide database was compiled assembling data from European sources as well as from the US FDA database, thus reducing the specificity of country-specific acrylamide estimates. Among other limitations, it is noteworthy to stress that, with few exceptions, DQs are not designed to capture information of food processing, such as cooking methods, extent of cooking and/or brands. Last but not least, it is well accepted that dietary self-reported measurements suffer from bias due to measurement errors, and thus do not provide accurate measures of intake in general.
One additional limitation in our study was the availability of only one replicate of 24-h dietary recall measurement. The sporadic nature of consumption of some acrylamide-rich food items (crisps, fried potatoes, etc.) resulted in large amounts of day-to-day variability in R measurements, likely to be one of the main reasons for the absence of correlation with acrylamide Hb adduct levels, with coefficients equal to 0.09 and 0.02 in smokers and never smokers, respectively.
In most recent dietary measurement validation studies, fairly basic comparisons of questionnaire measurements with short-term assessments (food diaries or 24-HDRs) moved to more complex comparisons of self-reported assessments with objective measurements, such as dietary biomarkers [24–26]. Based on the assumption that Hb adducts could be used as objective measurements to integrate dietary estimates of acrylamide exposure, the use of measurement error model was originally planned in this study to appropriately account for the error structure of the different types of measurement involved. However, based on the limited amount of information available at the individual level in our data, even among never smoker participants, estimates were very unstable and the exercise was not implemented further, thus limiting the possibility to carry out a proper validation study.
In our study, crude and adjusted correlation coefficients were computed. Among other relevant factors, adjustment for country was undertaken to account for systematic differences across centres in questionnaire design, biological sample treatment and other unmeasured group effects. Adjustment for country attenuated the magnitude of correlation coefficients, while the impact of adjusting for energy intake was overall limited. Larger correlation coefficients were observed at the aggregate levels focusing on centre-specific means. All pair-wise comparisons displayed larger correlations than coefficients computed using the individual level component. Unlike aggregate measures, individual level measurements are affected by within-person variation, which is likely the result of random measurement errors and day-to-day variation in dietary exposure [27, 28]. This observation is in line with previous evidence produced in the EPIC study, where the agreement between self-reported and objective measurements was larger at the aggregate level [29, 30]. Given the multicentre nature of the EPIC study, these comparisons are a natural way to evaluate any level of evidence contained in the data, although in most epidemiological investigations, it is mostly the individual level component that is exploited [31]. In the EPIC study, the definition of statistical models that entail individual and aggregate level components into the same statistical model was used in the past [32], and it is currently the object of ongoing research.
In summary, in a subsample of the EPIC study, sources of variability of dietary acrylamide from DQ and R measurements, as well as of Hb adducts levels, were investigated. A comparison of correlation coefficients between the different type of measurements revealed that, after adjustment for relevant covariables, the agreement between estimates of acrylamide based on self-reported and objective measurements is rather poor, with larger values of correlation coefficients at the aggregate level. Values of individual level correlations were poor even among never smokers. These results indicate that in the EPIC study, the assessment of validity of dietary acrylamide measurements is limited by a combination of relevant key factors: (1) the presence of measurement errors in dietary estimates of acrylamide, (2) the availability of one single replicate of R measurements per study subject in the present design, (3) the challenge of compiling a comprehensive database of acrylamide content in foods, (4) the lack of (over time replicates of) an objective biomarker measurement, specific enough to capture dietary exposure of acrylamide. In this context, ongoing comparisons of food sources of acrylamide as estimated by DQ and R measurements in the EPIC study might well reveal interesting features of the patterns of acrylamide consumption across EPIC centres.
References
Smith CJ, Perfetti TA, Rumple MA, Rodgman A, Doolittle DJ (2000) “IARC group 2A Carcinogens” reported in cigarette mainstream smoke. Food Chem Toxicol 38:371–383
Tareke E, Rydberg P, Karlsson P, Eriksson S, Tornqvist M (2002) Analysis of acrylamide, a carcinogen formed in heated foodstuffs. J Agric Food Chem 50:4998–5006
Tran NL, Barraj LM, Murphy MM, Bi X (2010) Dietary acrylamide exposure and hemoglobin adducts–National Health and Nutrition Examination Survey (2003–04). Food Chem Toxicol 48:3098–3108
Doerge DR, Young JF, McDaniel LP, Twaddle NC, Churchwell MI (2005) Toxicokinetics of acrylamide and glycidamide in B6C3F1 mice. Toxicol Appl Pharmacol 202:258–267
Tornqvist M, Fred C, Haglund J, Helleberg H, Paulsson B, Rydberg P (2002) Protein adducts: quantitative and qualitative aspects of their formation, analysis and applications. J Chromatogr B Analyt Technol Biomed Life Sci 778:279–308
Vikstrom AC, bramsson-Zetterberg L, Naruszewicz M, Athanassiadis I, Granath FN, Tornqvist MA (2011) In vivo doses of acrylamide and glycidamide in humans after intake of acrylamide-rich food. Toxicol Sci 119:41–49
Wirfalt E, Paulsson B, Tornqvist M, Axmon A, Hagmar L (2008) Associations between estimated acrylamide intakes, and hemoglobin AA adducts in a sample from the Malmo Diet and Cancer cohort. Eur J Clin Nutr 62:314–323
Kutting B, Uter W, Drexler H (2008) The association between self-reported acrylamide intake and hemoglobin adducts as biomarkers of exposure. Cancer Causes Control 19:273–281
Wilson KM, Vesper HW, Tocco P, Sampson L, Rosen J, Hellenas KE, Tornqvist M, Willett WC (2009) Validation of a food frequency questionnaire measurement of dietary acrylamide intake using hemoglobin adducts of acrylamide and glycidamide. Cancer Causes Control 20:269–278
Bjellaas T, Olesen PT, Frandsen H, Haugen M, Stolen LH, Paulsen JE, Alexander J, Lundanes E, Becher G (2007) Comparison of estimated dietary intake of acrylamide with hemoglobin adducts of acrylamide and glycidamide. Toxicol Sci 98:110–117
Pelucchi C, Galeone C, Levi F, Negri E, Franceschi S, Talamini R, Bosetti C, Giacosa A, La VC (2006) Dietary acrylamide and human cancer. Int J Cancer 118:467–471
Hogervorst JG, Baars BJ, Schouten LJ, Konings EJ, Goldbohm RA, van den Brandt PA (2010) The carcinogenicity of dietary acrylamide intake: a comparative discussion of epidemiological and experimental animal research. Crit Rev Toxicol 40:485–512
Riboli E, Hunt KJ, Slimani N, Ferrari P, Norat T, Fahey M, Charrondiere UR, Hemon B, Casagrande C, Vignat J, Overvad K, Tjonneland A, Clavel-Chapelon F, Thiebaut A, Wahrendorf J, Boeing H, Trichopoulos D, Trichopoulou A, Vineis P, Palli D, Bueno-de-Mesquita HB, Peeters PH, Lund E, Engeset D, Gonzalez CA, Barricarte A, Berglund G, Hallmans G, Day NE, Key TJ, Kaaks R, Saracci R (2002) European Prospective Investigation into Cancer and Nutrition (EPIC): study populations and data collection. Public Health Nutr 5:1113–1124
Vesper HW, Slimani N, Hallmans G, Tjonneland A, Agudo A, Benetou V, Bingham S, Boeing H, Boutron-Ruault MC, Bueno-de-Mesquita HB, Chirlaque D, Clavel-Chapelon F, Crowe F, Drogan D, Ferrari P, Johansson I, Kaaks R, Linseisen J, Lund E, Manjer J, Mattiello A, Palli D, Peeters PH, Rinaldi S, Skeie G, Trichopoulou A, Vineis P, Wirfalt E, Overvad K, Stromberg U (2008) Cross-sectional study on acrylamide hemoglobin adducts in subpopulations from the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. J Agric Food Chem 56:6046–6053
Slimani N, Kaaks R, Ferrari P, Casagrande C, Clavel-Chapelon F, Lotze G, Kroke A, Trichopoulos D, Trichopoulou A, Lauria C, Bellegotti M, Ocke MC, Peeters PH, Engeset D, Lund E, Agudo A, Larranaga N, Mattisson I, Andren C, Johansson I, Davey G, Welch AA, Overvad K, Tjonneland A, Van Staveren WA, Saracci R, Riboli E (2002) European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study: rationale, design and population characteristics. Public Health Nutr 5:1125–1145
Vesper HW, Ospina M, Meyers T, Ingham L, Smith A, Gray JG, Myers GL (2006) Automated method for measuring globin adducts of acrylamide and glycidamide at optimized Edman reaction conditions. Rapid Commun Mass Spectrom 20:959–964
Mowrer J, Tornqvist M, Jensen S, Ehrenberg L (1986) Modified Edman degradation applied to hemoglobin for monitoring occupational exposure to alkylating agents. Toxicol Environ Chem 11:215–231
Slimani N, Ferrari P, Ocke M, Welch A, Boeing H, Liere M, Pala V, Amiano P, Lagiou A, Mattisson I, Stripp C, Engeset D, Charrondiere R, Buzzard M, Staveren W, Riboli E (2000) Standardization of the 24-h diet recall calibration method used in the european prospective investigation into cancer and nutrition (EPIC): general concepts and preliminary results. Eur J Clin Nutr 54:900–917
Kleinbaum D, Kupper L, Muller K (1988) Applied regression analysis and other multivariable method. Duxbury Press, Belmont
Fisher RA (1970) Statistical methods for research workers. Hafner Publishing Company, Davien
SAS Institute Inc (2002) NC, USA, Cary
Vikstrom AC, Wilson KM, Paulsson B, Athanassiadis I, Gronberg H, Adami HO, Adolfsson J, Mucci LA, Balter K, Tornqvist M (2010) Alcohol influence on acrylamide to glycidamide metabolism assessed with hemoglobin-adducts and questionnaire data. Food Chem Toxicol 48:820–824
Vikstrom AC, Warholm M, Paulsson B, Axmon A, Wirfalt E, Tornqvist M (2012) Hemoglobin adducts as a measure of variations in exposure to acrylamide in food and comparison to questionnaire data. Food Chem Toxicol 50:2531–2539
Kaaks R, Ferrari P, Ciampi A, Plummer M, Riboli E (2002) Uses and limitations of statistical accounting for random error correlations, in the validation of dietary questionnaire assessments. Public Health Nutr 5:969–976
Kipnis V, Subar AF, Midthune D, Freedman LS, Ballard-Barbash R, Troiano RP, Bingham S, Schoeller DA, Schatzkin A, Carroll RJ (2003) Structure of dietary measurement error: results of the OPEN biomarker study. Am J Epidemiol 158:14–21
Ferrari P, Roddam A, Fahey MT, Jenab M, Bamia C, Ocke M, Amiano P, Hjartaker A, Biessy C, Rinaldi S, Huybrechts I, Tjonneland A, Dethlefsen C, Niravong M, Clavel-Chapelon F, Linseisen J, Boeing H, Oikonomou E, Orfanos P, Palli D, de Santucci MM, Bueno-de-Mesquita HB, Peeters PH, Parr CL, Braaten T, Dorronsoro M, Berenguer T, Gullberg B, Johansson I, Welch AA, Riboli E, Bingham S, Slimani N (2009) A bivariate measurement error model for nitrogen and potassium intakes to evaluate the performance of regression calibration in the European Prospective Investigation into Cancer and Nutrition study. Eur J Clin Nutr 63(Suppl 4):S179–S187
Kaaks R, Slimani N, Riboli E (1997) Pilot phase studies on the accuracy of dietary intake measurements in the EPIC project: overall evaluation of results. European Prospective Investigation into Cancer and Nutrition. Int J Epidemiol 26(Suppl 1):S26–S36
Willett W (1989) An overview of issues related to the correction of non-differential exposure measurement error in epidemiologic studies. Stat Med 8:1031–1040
Ferrari P, Roddam A, Fahey MT, Jenab M, Bamia C, Ocke M, Amiano P, Hjartaker A, Biessy C, Rinaldi S, Huybrechts I, Tjonneland A, Dethlefsen C, Niravong M, Clavel-Chapelon F, Linseisen J, Boeing H, Oikonomou E, Orfanos P, Palli D, de Santucci MM, Bueno-de-Mesquita HB, Peeters PH, Parr CL, Braaten T, Dorronsoro M, Berenguer T, Gullberg B, Johansson I, Welch AA, Riboli E, Bingham S, Slimani N (2009) A bivariate measurement error model for nitrogen and potassium intakes to evaluate the performance of regression calibration in the European Prospective Investigation into Cancer and Nutrition study. Eur J Clin Nutr 63(Suppl 4):S179–S187
Ferrari P, Al-Delaimy WK, Slimani N, Boshuizen HC, Roddam A, Orfanos P, Skeie G, Rodriguez-Barranco M, Thiebaut A, Johansson G, Palli D, Boeing H, Overvad K, Riboli E (2005) An approach to estimate between- and within-group correlation coefficients in multicenter studies: plasma carotenoids as biomarkers of intake of fruits and vegetables. Am J Epidemiol 162:591–598
Ferrari P, Day NE, Boshuizen HC, Roddam A, Hoffmann K, Thiebaut A, Pera G, Overvad K, Lund E, Trichopoulou A, Tumino R, Gullberg B, Norat T, Slimani N, Kaaks R, Riboli E (2008) The evaluation of the diet/disease relation in the EPIC study: considerations for the calibration and the disease models. Int J Epidemiol 37:368–378
Ferrari P, Carroll RJ, Gustafson P, Riboli E (2008) A Bayesian multilevel model for estimating the diet/disease relationship in a multicenter study with exposures measured with error: the EPIC study. Stat Med 27:6037–6054
Freisling H, Moskal A, Ferrari P, Nicolas G, Knaze V, Clavel-Chapelon F, Boutron-Ruault M-C, Nailler L, Teucher B, Grote V, Boeing H, Clemens M, Tjønneland A, Olsen A, Overvad K, Quirós JR, Duell EJ, Sánchez M-J, Amiano P, Chirlaque M-D, Barricarte A, Khaw K-T, Wareham NJ, Crowe FL, Gallo V, Oikonomou E, Naska A, Trichopoulou A, Palli D, Agnoli C, Tumino R, Polidoro S, Mattiello A, Bas Bueno-de-Mesquita H, Ocké MC, Peeters PHM, Wirfält E, Ericson U, Bergdahl IA, Johansson I, Hjartåker A, Engeset D, Skeie G, Riboli E, Slimani N. Dietary acrylamide exposure differs greatly across ten countries participating in the European Prospective Investigation into Cancer and Nutrition. EJN (in press)
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Ferrari, P., Freisling, H., Duell, E.J. et al. Challenges in estimating the validity of dietary acrylamide measurements. Eur J Nutr 52, 1503–1512 (2013). https://doi.org/10.1007/s00394-012-0457-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-012-0457-7