
Abstract
Purpose
Chronic sugar-sweetened beverage (SSB) consumption is associated with obesity and type 2 diabetes mellitus (T2DM). Hyperglycaemia contributes to metabolic alterations observed in T2DM, such as reduced oxidative capacity and elevated glycolytic and lipogenic enzyme expressions in skeletal muscle tissue. We aimed to investigate the metabolic alterations induced by SSB supplementation in healthy individuals and to compare these with the effects of chronic hyperglycaemia on primary muscle cell cultures.
Methods
Lightly active, healthy, lean subjects (n = 11) with sporadic soft drink consumption underwent a 4-week SSB supplementation (140 ± 15 g/day, ~2 g glucose/kg body weight/day, glucose syrup). Before and after the intervention, body composition, respiratory exchange ratio (RER), insulin sensitivity, muscle metabolic gene and protein expression were assessed. Adaptive responses to hyperglycaemia (7 days, 15 mM) were tested in primary human myotubes.
Results
SSB supplementation increased fat mass (+1.0 kg, P < 0.05), fasting RER (+0.12, P < 0.05), fasting glucose (+0.3 mmol/L, P < 0.05) and muscle GAPDH mRNA expressions (+0.94 AU, P < 0.05). PGC1α mRNA was reduced (−0.20 AU, P < 0.05). Trends were found for insulin resistance (+0.16 mU/L, P = 0.09), and MondoA protein levels (+1.58 AU, P = 0.08). Primary myotubes showed elevations in GAPDH, ACC, MondoA and TXNIP protein expressions (P < 0.05).
Conclusion
Four weeks of SSB supplementation in healthy individuals shifted substrate metabolism towards carbohydrates, increasing glycolytic and lipogenic gene expression and reducing mitochondrial markers. Glucose-sensing protein MondoA might contribute to this shift, although further in vivo evidence is needed to corroborate this.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity caused by overnutrition and a sedentary lifestyle are the major risk factors for type 2 diabetes mellitus (T2DM) [1]. T2DM is characterized by defects in insulin secretion, elevated hepatic glucose output and impaired glucose uptake in target tissues, especially skeletal muscle [2]. Moreover, the metabolic phenotype of skeletal muscle in T2DM is associated with an impaired capacity to increase fat oxidation upon increased fatty acid availability and to switch between fat and glucose as the primary fuel [3]. Skeletal muscle fibres in insulin resistant and T2DM patients show an elevation in glycolytic and lipogenic enzyme expression and a reduction in oxidative capacity [4–6], accompanied by a lower mitochondrial volume density [7]. Moreover, these patients show an increase in fast glycolytic fibre type IId/x content [8]. Interestingly, these same skeletal muscle fibre alterations are already evident in obese non-diabetic subjects [9].
Although the role of lipid metabolites in the impairment of cellular insulin response is well established [10], knowledge about the contribution of glucose and associated metabolites to the development of an underlying metabolic phenotype of T2DM is still emerging. Several studies have shown that high glucose availability, in the form of hyperglycaemia, can influence signalling pathways that regulate peripheral glucose uptake and metabolic gene expression [11–13]. Under hyperglycaemic conditions, metabolic gene expression is consistently shifted towards a lower mitochondrial enzyme expression and elevated glycolytic and lipogenic expressions in skeletal muscle cells [11–13].
Chronic sugar-sweetened beverage (SSB) consumption is highly prevalent in the Western diet and has been shown to be highly correlated with the development of obesity and T2DM [14–16]. However, more evidence is needed to prove that SSB consumption contributes uniquely to obesity [17]. In the long term, periods of high glucose availability, induced by repeated glucose-based soft drink consumption, could lead to similar metabolic alterations as observed in chronic hyperglycaemia. This could contribute to the development of a metabolic phenotype such as the one found in insulin resistance and T2DM.
Glucose sensing in skeletal muscle cells, as part of a mechanism for the maintenance of cellular energy homoeostasis, has been demonstrated to be strongly dependent on the transcription factor MondoA [12]. MondoA seems to be a master regulator of glycolytic genes and indeed it activates the transcription of numerous genes encoding metabolic enzymes [18]. Glycolytic gene expression is highly upregulated in response to MondoA recruitment from cytoplasm to nuclei, building a complex with the transcription factor max-like protein x (Mlx), in high glucose conditions [12, 19]. A further target of the MondoA:Mlx complex is the thioredoxin-interacting protein (TXNIP). TXNIP impairs peripheral glucose uptake stimulating radical oxygen species production. Consequently, subjects in pre-diabetic and diabetic states show a rise in TXNIP mRNA transcripts in skeletal muscle tissue [11]. Thus, chronic high glucose availability in vitro leads to MondoA-mediated metabolic alterations in muscle cells, which seem to correspond to those found in pre-diabetic and diabetic state in vivo.
For these reasons, we have designed 2 studies. In study 1, we hypothesized that periods of high glucose availability, induced by SSB consumption for 4 weeks, can shift the metabolism towards carbohydrates, altering metabolic gene expression in the skeletal muscle tissue towards an elevation in glycolytic and lipogenic marker enzyme expression glyceraldehyde-3-phosphate dehydrogenase and acetyl-CoA carboxylase (GAPDH and ACC) and a reduction in mitochondrial marker peroxisome proliferator–activated receptor-gamma coactivator 1 α and citrate synthase (PGC1α and CS) expression. Moreover, we expected an elevated recruitment of MondoA to nuclei and an elevation of TXNIP expression. In study 2, we hypothesized that primary human myotubes exposed to chronic hyperglycaemia (15 mM) would show metabolic alterations, such as an increase in glycolytic and lipolytic capacity and a decrease in oxidative capacity and confirm the elevation of MondoA and of TXNIP expressions found in cell lines [11, 12, 18].
Materials and methods
Ethical approval
The departmental ethics committee (of Bangor University) approved the study designs in agreement with the Declaration of Helsinki. All subjects involved in these studies were given a participant information sheet and signed an informed consent form, prior to testing.
In vivo study
Subjects and study design
A pre-test–post-test within subject design was used. An initial screening for lifestyle and SSB consumption was executed via qualitative questionnaires. Healthy people with low physical activity and consuming less than 500 ml of SSB per week were considered eligible to take part in this study (32 out of 213 people screened). Eleven subjects, 5 males and 6 females (Table 1), consented to take part in this study. The subjects were informed that they would receive £100 upon completion of testing as compensation for their time. Before and after the intervention period, subjects attended our laboratories for two testing sessions. Although all the subjects included in this study had a low physical activity, they were explicitly asked to refrain from exercise for 24 h prior to all tests. Post-tests were conducted at least 36 h after the last SSB consumption. One subject was not able to attend the post-intervention oral glucose test and the muscle biopsy because of a viral infection. Only dietary and body composition data of this subject were used for the statistical analysis.
Study intervention
Subjects underwent a 4-week SSB supplementation (Lucozade Energy, GlaxoSmithKline plc, Harlow, UK) on top of their habitual diet. The ingredients of Lucozade Energy were the following: carbonated water, glucose syrup (24 %), orange juice from concentrate (5 %), citric acid, preservatives (sodium benzoate, sodium bisulphate), flavourings (including caffeine), stabilizer (acacia gum), antioxidant (ascorbic acid) and colour (beta carotene). The SSB was provided by the experimenters. Supplementation was carried out on the basis of a daily carbohydrate intake of ≈2.0 g/kg body weight. This corresponded on average to 760 mL SSB per subject per day. Empty SSB bottles were collected.
Diet diaries and body composition
Subjects were introduced to the diet diaries via standard instruction [20]. Subjects were asked to keep a 7-day diet diary for a week before the intervention started and a 14-day diet diary during the supplementation month [21]. The diet analysis was conducted using the United States Department of Agriculture food search for windows, Version 1.0, database version SR21 in combination with nutritional information labels. Lean mass, fat mass and bone mineral content were assessed by Dual-energy X-ray Absorptiometry (DXA) (QDR1500, software version 5·72; Hologic, Waltham, MA, USA) as described previously [22].
Indirect calorimetry
Subjects were asked to attend this test session in an overnight (8–12 h) fasted condition. The meal prior to the indirect calorimetry and the blood and muscle sampling met the World Health Organization recommendations [23] for an oral glucose tolerance test. Respiratory exchange ratio (RER) was measured by indirect calorimetry (MetaLyzer 3B, Cortex Biophysik, Leipzig, Germany), following da Rocha et al.’s recommendations [24]. Ambient temperature of 20 °C and 40 % humidity were kept constant throughout this test that was carried out in a climate chamber. The steady state coefficient of variation for our indirect calorimetry system was below 5 %. Subjects with a coefficient of variation above this value were excluded from the statistical analysis. Substrate oxidation rates were calculated based on indirect calorimetry, assuming a constant urinary nitrogen excretion (n) equal to 0.01 g/min. The equations used to calculate the substrate oxidation rate were:
where c and f are the grams of carbohydrate and fat oxidized per min, respectively [25].
Blood sample analysis
An overnight fasting venous blood sample (4 mL) was collected in heparinized vacutainers from the antecubital vein of each subject. Then, a 75-g oral glucose load was administered to the subjects and after 1 h a new venous blood sample was drawn. Plasma glucose was analysed for each sample by immobilized enzymatic assay (YSI 2300 STAT, Incorporated Life Sciences, Yellow Springs, OH, USA). Lipid profile was analysed from the fasting plasma samples by optic enzymatic assay (Reflotron®, Roche Diagnostics, Mannheim, Germany). The plasma samples were then stored at -40 °C for later plasma insulin analysis. Plasma insulin was analysed by ELISA (Ultrasensitive human insulin ELISA-kit, Mercodia, Uppsala, Sweden). Homeostasis model assessment (HOMA) calculator, version 2.2.2., was used to compute steady state beta cell function (%B), insulin sensitivity (%S) and insulin resistance (IR) (http://www.dtu.ox.ac.uk/homa).
Muscle biopsies
The needle muscle biopsies were taken 1 h after the glucose load. After local anaesthesia (1 % lignocaine), 2 needle muscle biopsies were collected at a mid-distance between the great trochanter and the femorotibial joint on the vastus lateralis (VL) muscle of the left leg of the volunteers. Biopsies were taken with a 14-gauge needle (14ga × 10 cm, Tru•Core® II Biopsy Instrument, Angiotech Gainesville, FL, USA). The biopsies for the post-test were taken about 0.5–1 cm from the pre-test biopsies. Muscle specimens were snap-frozen and stored in liquid nitrogen until further analysis.
Real-Time PCR
The frozen muscle biopsies (15.6 ± 0.30 mg) were pulverized (1,900 rpm for 15 s) at liquid nitrogen temperature by using a micro-dismembrator (Sartorius-Stedim Biothec, Goettingen, Germany). Total RNA was isolated using an RNeasy Fibrous Tissue Kit (RNeasy, Qiagen Ltd, Crawley, West Sussex, UK) with DNase treatment following the manufacturer’s instructions. RNA concentration and purity were measured at 260 nm and 280 nm. Total RNA concentrations averaged around 108 ± 37 μg/mL. cDNA was synthesized from 50 ng RNA using a reverse transcription kit (Sensiscript, Qiagen Ltd, Crawley, West Sussex, UK) at 37 °C for 60 min after heating for 5 min at 65 °C. cDNA was stored at -80 °C until use.
Real-time RT-PCR was performed using 2× Quantitect SYBR green PCR master mix (Qiagen Ltd, Crawley, West Sussex, UK) on a fast real-time PCR system (7900HT, Applied Biosystems, Carlsbad, California, USA). Primers for each gene (supplementary Table 1) were selected from published sources or designed using reference mRNA sequences (National Centre for Biotechnology Information, National Library of Medicine, Bethesda, MD, USA) and Primer3 software (http://frodo.wi.mit.edu/primer3/). All primers were confirmed for homologous binding to the desired mRNA targets by conducting a BLAST search (http://blast.ncbi.nlm.nih.gov/) once chosen primers were synthesized (Eurofins MWG Operon, Ebersberg, Germany). cDNA transcripts of all genes of interest were measured simultaneously in duplicates. To normalize the gene expression, 18s rRNA was used as an endogenous control. Each reaction contained PCR master mix, forward and reverse primers (0.3 μM), RNase free water and 2.5 μL cDNA in 25 μL final volume. Thermal cycling conditions were as follows: PCR initial activation step of 15 min at 95 °C, 3 step cycling of 15 s denaturation at 94 °C, 30 s annealing at 50–60 °C (varied with primer) and 30s extension at 72 °C for 45 cycles. The melting curves that were performed after all runs showed single products in each case. Critical threshold (CT) values were recorded for the target gene and the endogenous control, and these values were used to quantify mRNA expression. The standard curve method (User Bulletin 2 ABI PRISM 7700 Sequence Detection System) was used to quantify relative amounts of mRNA for each gene. The standard curve was made by preparing a series of 10 dilutions of template cDNA for both the target gene and the endogenous control; these were run simultaneously with all samples.
Western blotting and myosin heavy chain (MHC) analysis
The frozen muscle biopsies and 150 μL of frozen buffer, containing 10 % PBS, 5 % protein phosphatase inhibitors, 0.1 % of 1 M DTT, 0.05 % protease inhibitor and 0.1 % detergent (Nuclear Extraction Kit, Activemotif, Rixensart, Belgium) were pulverized (1,900 rpm for 15 s) at liquid nitrogen temperature by using a micro-dismembrator (Mikro-Dismembrator S, Sartorius-Stedim Biotech, Goettingen, Germany). The pulverized muscle samples were thawed on ice and centrifuged at 4 °C (20,000×g for 5 min). The supernatants were used to assess ACC, fumarate hydratase (FUM), GAPDH and TXNIP expression levels. Pellets, containing nuclei and muscle fibrils were extracted on ice by means of an ultrasonic processor (VCX 130, Sonics & Materials INC, Newtown, CT, USA), with myosin extraction buffer (0.6 M KCl, 1 mM EGTA, 10 mM sodium phosphate dibasic, 1 mM PMSF, pH 6.8) at 0 °C. Extracts were centrifuged at 20,000×g for 20 min at 4 °C and crude nuclear membrane fraction resuspended in SDS-sample buffer and used to assess MondoA expression levels. The protein content of the muscle samples was assessed by Lowry protein assay (Sigma-Aldrich, Saint Louis, MO, USA). Equal amounts of total protein per lane were separated electrophoretically in 10 or 5 % SDS-PAGE and were then transferred to a nitrocellulose membrane (Hybond ECL 6 × 8 cm, GE Healthcare, Amersham, Slough, UK). Loading control was performed using India ink staining of the nitrocellulose membranes after blotting and normalization was carried out based on α-actin signal levels. After blocking in PBS, containing 0.2 % Tween and 5 % low-fat dry milk, blots were probed with primary antibodies for 4 h at dilutions of 1:250, 1:2,000 and 1:10,000 for ACC (H-76) (sc-30212), FUM (J-13) (sc-100743) and GAPDH (0411) (sc-47724), respectively (Santa Cruz Biotechnology Inc, Santa Cruz, CA, USA). MondoA (1:500) [18] and TXNIP (1:1,000) (MBL, Naka-ku Nagoya, Japan) were incubated overnight. As secondary antibodies, goat anti-rabbit IgG-HRP 1:15,000 (Sigma-Aldrich, St. Louis, MO, USA) or goat anti-mouse IgG-HRP 1:5,000 (Santa Cruz Biotechnology Inc, Santa Cruz, CA, USA) were used. ECL (Amersham Hyperfilm ECL, 18 × 24 cm, GE Healthcare Life Sciences, Little Chalfont, UK) detection was carried out using the SuperSignal West Pico or Femto ECL kit (Pierce, Rockford, IL, USA). If necessary, membranes were stripped for 45 min at 50 °C in stripping buffer (10 % SDS, 0.5 M Tris, pH 6.8 and 0.08 % β-mercaptoethanol), washed for 1 h and re-probed. Densitometry was then used to quantify protein bands (Gel Doc 2000 and software Quantity One-4.6.3, Bio-Rad, Hercules, CA, USA). MHC extraction and electrophoresis were executed as described in Sartor et al. [22].
In vitro study
Primary cell cultures
Four muscle biopsies were taken from healthy male subjects (age, 38 ± 13 years; height, 1.79 ± 0.06; weight, 72 ± 6 kg) for the isolation of satellite cells. After muscle biopsies were taken, tissue was immediately transferred to RT skeletal muscle growth medium (SMGM) with 5 % foetal calf serum (FCS), 1 % l-glutamine with penicillin/streptomycin plus supplements (PromoCell, Heidelberg, Germany), and washed in medium twice. This was followed by disintegration with surgical blades with 0.05 % trypsin (PAA, Pasching, Austria) in PBS for 30 min, after which trypsination was stopped by trypsin inhibitor (Sigma-Aldrich, St. Louis, MO, USA) with a final concentration of 0.14 mg/mL. After centrifugation at 800×g for 5 min at 10 °C, the pellet was resuspended in accutase (PAA, Pasching, Austria) and additionally incubated for 20 min at 37 °C. After sedimentation, the cell suspension was centrifuged again at 800×g for 5 min at 10 °C, and the cell pellet was resuspended in SMGM with 5 % FCS, 1 % l-glutamine with penicillin/streptomycin plus supplements (PromoCell, Heidelberg, Germany). The cell suspension was transferred into 75-cm2 TC flasks (Greiner, Frickenhausen, Germany) and incubated at 37 °C, 5 % CO2 and 95 % humidity until passage. Half-medium change was performed every second day. Three passages were completed before the initiation of differentiation (Supplementary Fig. 1). The samples of the human primary myotubes were tested for creatine kinase activity after the initiation of differentiation in DMEM (PAA, Pasching, Austria) with 2 % FCS for 4 days.
For the cultivation of the differentiated myocytes, grown on microcarriers, 5 × 106 cells per 10 mL medium were seeded on microcarriers in suspension (0.015 g microcarriers, CultiSpher-GL; Percell Biolytica, Astorp, Sweden) in 25-cm2 flasks. Flasks were placed on a circular shaker (53 rpm) to guarantee adequate O2 supply to the cells and to prevent the cells and microcarriers from settling down. After 12 days of differentiation in DMEM with 2 % FCS, myotubes were exposed to high glucose, DMEM with 2 % FCS, 15 mM d-glucose (Sigma-Aldrich, St. Louis, MO, USA) and 10 μg/mL of insulin (Actrapid, Novo Nordisk A/S, Bagsvaerd, Denmark). Control myotubes were cultivated in DMEM with 2 % FCS, 5 mM d-glucose and 10 μg/mL insulin. Exposure time to high glucose or control conditions was 7 days.
Cell harvest and Western blotting
The myotubes on microcarriers were washed with PBS, lysed and denatured with SDS-PAGE sample buffer at 95 °C for 3 min and cooled on ice. The samples were cleared by centrifugation at 16,000×g in QIAshredder columns (Qiagen, Hilden, Germany). The eluates were frozen in liquid nitrogen and kept at −80 °C until use. Nuclear and cytoplasmic fractions from myotubes grown on microcarriers for 12 days followed by exposure to high glucose (15 mM) and control conditions (5 mM) in DMEM with 2 % FCS, 10 μg/mL insulin for 7 days were prepared according to the manufacturer’s protocols using a nuclear extraction kit (Kit No400010&No40410, Activemotif, Rixensart, Belgium).
Statistics
The statistical analysis was performed using SPSS 11.5. Unless otherwise specified, all data are reported as means ± SDs. Outcomes of the in vivo study were analysed with Student’s paired samples t-tests. The in vitro outcomes were analysed with non-parametric Mann–Whitney U tests. Pearson correlations for the differences between pre- and post-tests were conducted. The significance level was set at 0.05 (two-tailed). The level for trends was set at 0.10.
Results
In vivo study
Resting glucose levels, insulin sensitivity and metabolic substrate preference
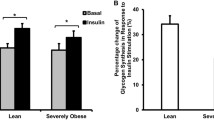
The SSB supplementation significantly increased fasting plasma glucose levels, while fasting plasma insulin levels showed a clear trend towards an elevation (pre, 4.83 ± 0.43 mmol/L, post, 5.13 ± 0.38 mmol/L, P < 0.05; pre, 4.95 ± 1.90 mU/L, post, 6.40 ± 1.62 mU/L, P = 0.09, respectively) (Fig. 1a and b). Moreover, HOMA 2 revealed that %S was diminished, and IR was increased (Table 1). %B showed no response. Blood lipids (Table 1) did not change after the 4-week intervention. The analysis of resting substrate metabolism after overnight fasting, measured by indirect calorimetry, revealed a significant increase in RER (pre, 0.75 ± 0.09, post, 0.87 ± 0.08; P < 0.05, n = 8) (Fig. 1d). Calculation of the preferred substrate oxidation demonstrated that metabolism changed from the expected high level of fat oxidation to a strong preference for carbohydrate oxidation after only 4 weeks intervention (Fig. 1c).

Fasting plasma glucose, insulin, substrate utilization and respiratory exchange ratio (RER). a Overnight fasting plasma glucose levels and b Fasting plasma insulin levels before and after 4 weeks of sugar-sweetened beverage (SSB) supplementation. c Substrate oxidation rate derived from the RER, measured after overnight fast before and after 4 weeks of SSB supplementation. d RER (VCO2/VO2) measured by indirect calorimetry after overnight fast before and after the intervention. Data are presented as means ± SEMs. *P < 0.05 and # P < 0.10 for differences between pre- and post-intervention (a and b, n = 10; c and d, n = 8)
Diet diary analysis and body composition
The analysis of daily macronutrient intake (Table 2) shows that the energy intake during the SSB supplementation was not significantly different from the energy intake at baseline. Moreover, carbohydrate and especially sugar intake were strongly increased during the intervention, with a concomitant reduction in protein intake and PUFA (Table 2). The body composition analysis by DXA revealed a significant increase in fat mass while lean mass did not change (Table 1).
Myosin heavy chains and metabolic gene/protein expression in skeletal muscle
MHC electrophoresis and quantification showed no difference in fibre type composition between pre- and post-intervention, confirming that results were not confounded by variability in the origin of the muscle biopsies (Table 3). Post-supplementation metabolic gene expressions in the VL muscle were altered. The gene expression of the glycolytic marker GAPDH increased significantly, and the gene expression of the lipogenic marker ACC revealed a trend towards an increase (P < 0.05, P = 0.09, respectively), while the gene expression of the co-transcription factor PGC1α used as a marker for mitochondrial gene expression was significantly reduced (P < 0.05). No alteration in the expression of CS mRNA was detected (Table 3). Western blot analysis of metabolic markers (GAPDH, ACC, FUM) on protein levels showed no significant alterations (pre, 1.00 ± 0.24 AU, post, 0.93 ± 0.37 AU, P = 0.393; pre, 1.00 ± 0.55 AU, post, 0.84 ± 0.47 AU, P = 0.328; pre, 1.00 ± 0.35 AU, post, 0.79 ± 0.41 AU, P = 0.179, respectively).
MondoA expression in skeletal muscle biopsies
Western blot analysis of MondoA content in the crude nuclei membrane fraction of biopsy samples showed a strong trend towards an elevated protein content of this transcription factor (pre, 1.00 ± 1.08 AU; post, 2.58 ± 2.46 AU; P = 0.08) (Fig. 2a and b). However, TXNIP protein expression did not change significantly (pre, 1.00 ± 0.38 AU; post, 1.24 ± 0.49 AU; P = 0.21) (Fig. 2c and d). Changes in TXNIP expression correlated significantly with changes in MondoA expression (r = 0.88, P < 0.01, n = 10) (Fig. 2e). In line with the results for MondoA on protein level, RT-PCR analysis revealed a strong trend towards an elevated MondoA mRNA transcription after the SSB supplementation (P = 0.057).

MondoA and thioredoxin-interacting protein (TXNIP) expression. a Western blot analysis of MondoA in nuclear membrane fraction from skeletal muscle biopsies before and after 4 weeks of sugar-sweetened beverage (SSB) supplementation, with α-actin as loading control. Image insert shows an example of MondoA Western blots of strong responders to the SSB consumption. b Densitometric quantification of Western blots for MondoA, pre- and post-intervention. c Western blot analysis of TXNIP in cytoplasmic fraction of skeletal muscle biopsies pre- and post-intervention. d Densitometric quantification of Western blots for TXNIP, pre- and post-intervention. e Correlation between changes in MondoA and changes in TXNIP expression (r = 0.88, P < 0.01, n = 10). Data are presented as means ± SEMs. # P < 0.10 for differences between pre- and post-intervention (n = 10)
In vitro study
MondoA and TXNIP protein expressions in human primary myotubes
Western blot analysis of cell homogenates revealed that expression levels of MondoA and TXNIP were increased after 7 days of high glucose availability (190 ± 30 % and 352 ± 47 % of control; P < 0.05) (Fig. 3a and b). The expression of TXNIP was highly correlated with the expression of MondoA (r = 0.87; P < 0.011; n = 7) (Fig. 3c). Additionally, nuclear and cytoplasmic fractions derived from the cultured myocytes showed that MondoA is strongly recruited to the nuclei membrane fraction under hyperglycaemic conditions (Fig. 3a).

MondoA and thioredoxin-interacting protein (TXNIP) expression in vitro. a Western blot analysis of MondoA and TXNIP expression in primary muscle cell culture under conditions of hyperglycaemia (15 mM) and control (5 mM)—12 days plus 7 days exposure, with α-actin as loading control. MondoA cytoplasmic and nuclear fractions were derived from the same cultures. b Densitometric quantification of Western blots for MondoA and TXNIP, expressed as a percentage of control. c Pearson correlation between MondoA and TXNIP. Open dots represent myotube cultures exposed to normal glucose (5 mM); closed dots represent myotube cultures exposed to high glucose (15 mM) (r = 0.87; P < 0.01; n = 7). Data are presented as means ± SEMs, *P < 0.05 for differences between glucose conditions
Glycolytic and lipogenic enzymes
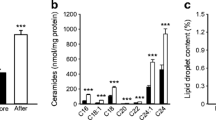
Western blot analysis of glycolytic, oxidative and lipogenic marker enzymes from myotubes exposed to hyperglycaemia for 7 days showed a significant increase in glycolytic GAPDH and lipogenic ACC expressions compared with controls (173 ± 32 % and 177 ± 18 % of control; P < 0.05). The oxidative marker enzyme FUM did not respond to the high glucose exposure (91 ± 30 % of control; P = 0.44) (Fig. 4).

Metabolic marker enzyme expressions in vitro. a Western blot analysis of metabolic markers acetyl CoA Carboxylase (ACC), fumarate hydratase (FUM) and glyceraldehyde-3-phosphate dehydrogenase (GAPDH) in primary muscle cell culture (after 12 days cultivation) exposed to hyperglycaemia (15 mM) and control (5 mM) for a further 7 days. b Densitometric quantification of Western blots for ACC, FUM and GAPDH, expressed as a percentage of control. Data are presented as means ± SEMs. *P < 0.05 for differences between glucose conditions (n = 7)
Discussion
The major finding of this work is that 4 weeks of periodic high glucose availability can induce metabolic alterations in skeletal muscle in vivo comparable to adaptations of muscle cells towards chronic hyperglycaemic conditions in vitro. Because of the limited duration of the SSB supplementation, for evident ethical reasons and its periodic nature, 2 drinks per day, in vivo skeletal muscle metabolic changes were visible mainly at mRNA level. However, a clear metabolic shift towards carbohydrates was detectible at a protein level in vitro.
In detail, we observed that 4 weeks of SSB supplementation led to a significant increase in fasting plasma glucose and a strong trend towards a reduction in insulin sensitivity in healthy lean individuals with low physical activity, who otherwise consumed less than 500 mL SSB per week. This selection was necessary to avoid any pre-existing physiological adaptation to soft drink consumption. These outcomes are in line with previous investigations in healthy as well as hyperinsulinemic subjects [26, 27]. The SSB supplementation elicited adipose tissue deposition, and this may have contributed to the alterations found in the insulin system and in the metabolism of the skeletal muscle cells. However, it has been shown that changes in insulin sensitivity can be independent of changes in fat mass [28]. Additionally, in our human myotubes metabolic changes were found in the absence of extracellular adipose tissue activity. Several studies have shown that neither high-glycemic-index food intake nor glucose intake just before bedtime increases overnight fasting blood glucose and insulin levels [29–31]. Therefore, the alterations that we have detected should be related to long-lasting adaptations in glucose homoeostasis and metabolism, produced by the 4 weeks of SSB supplementation. It is highly unlikely that our outcome could be explained merely by an acute effect of the last soft drink intake, which occurred not less than 36 h before the post-intervention blood tests.
Certainly, limited glycogen storage capacity may contribute to these adaptational responses, and it is plausible that after 4 weeks of periodic high glucose load, glycogen storage capacity gradually reached its maximum, increasing the need for enhanced glycolysis, glucose oxidation and lipogenesis to reduce intracellular glucose availability [32]. This interpretation is supported by the increase in overnight-fasted resting RER, which represents a ~40 % reduction in lipid oxidation and concomitant increase in carbohydrate oxidation. The high-carbohydrate-induced RER increase is in line with previous investigations [33]. Lipid oxidation is known to be inhibited following carbohydrate ingestion during exercise [34, 35], and it has also been shown to be reduced in post-prandial periods [36]. Work on rodents has shown that fat oxidation is reduced after a high-glycemic-index diet as early as 3 weeks after onset of the diet preceding the development of obesity [37], and more recently, Roberts and colleagues [38] have shown that a 3-day sugar-rich diet leads to a reduced post-prandial fat oxidation in non-obese subjects, even without a change in fasting RER.
Alterations towards higher glycolytic and lipogenic capacity in skeletal muscle cells are typical of the metabolic phenotype seen in T2DM [39]. Glycolytic and lipogenic enzymes have been shown to possess carbohydrate response elements (ChoRE) in their promoter sequences [40, 41]. Indeed, we found that after 4 weeks of SSB consumption, skeletal muscle metabolic gene expressions were altered towards a higher expression of glycolytic enzyme (GAPDH), a known target gene of MondoA in skeletal muscle, a tendency towards a higher lipogenic (ACC) gene expression and a reduced gene expression of mitochondrial co-transcription factor PGC1α, a master regulator of mitochondrial transcription [42]. However, CS mRNA expression was not altered; this could possibly due to the level of physical activity of our subjects leading to calcium transients and calcium-dependent signal transduction in skeletal muscle [43]. It has been shown recently that calcium-dependent activation of CS transcription can suppress the negative influence of glucose signalling on CS expression in muscle cell culture experiments [13]. Otherwise, this does not exclude strong effects of sugar consumption on mitochondrial gene expression in sedentary people and after longer exposure times. An elevated ratio of glycolytic to mitochondrial enzymes has been shown in insulin-resistant and T2DM muscle [6], and reduced mitochondrial transcription has also been shown to be dependent on glycogen levels [44, 45]. Moreover, a similar adaptational response, as shown by elevations of GAPDH and ACC on protein level, was found in our in vitro study, during which primary muscle cell cultures were exposed to hyperglycaemia for 1 week. These findings are in line with the results seen in primary muscle cell cultures from rabbit and from a C2C12 cell line under hyperglycaemic conditions [13] and hypoglycaemic conditions [44].
While hyperglycaemia in T2DM may be the result of processes related to impaired beta cell function [46], adipokine signalling [47] or influence of lipid metabolites [10], the contribution of glucose-dependent signalling for the development of the metabolic phenotype found in skeletal muscle in T2DM seems a highly plausible explanation too. The development of this metabolic phenotype could be enhanced by glucose-sensing transcription factors such as MondoA. To our knowledge, this was the first attempt to study MondoA responses in vivo. SSB consumption for 4 weeks led to a trend towards an increased protein expression of MondoA and to a significant correlation between changes in MondoA and changes in TXNIP protein expressions in skeletal muscle in vivo. Our in vitro work with human skeletal muscle cell cultures, which we exposed to hyperglycaemia for 7 days, showed a stronger response and correlation, suggesting a key role for MondoA in glucose-induced metabolic adaptations. In fact, in vitro MondoA and TXNIP were upregulated, and MondoA was found predominantly in the nuclear fraction. This is in accordance with the findings of Stoltzman and colleagues [12] in L6 cells. MondoA has been shown to contribute to 75 % of glucose-induced gene expression in HA1ER cells using Agilent 44 K human microarrays [12], and MondoA is certainly both necessary and sufficient for glycolytic enzyme expression, as demonstrated in C2C12 and K562 cells [18]. However, the influence of intramuscular lipids cannot be excluded. MondoA has also been recognized as the transcription factor that upregulates the expression of TXNIP [12]. TXNIP is involved in peripheral glucose uptake inhibition, especially in skeletal muscle [11] and it is a critical regulator in glucose production in the liver [48]. Moreover, TXNIP has been shown to be increasingly transcribed in skeletal muscle of pre-diabetics and T2DM patients, and it has been suggested that it contributes to the development of T2DM [11, 49]. The lack of a clear TXNIP response in our in vivo study might be explained by the limited duration of the periodic high glucose availability, but also by the increase in circulating insulin induced by the SSB supplementation in healthy individuals. In fact, Kaadige and colleagues [50] have shown that in the presence of glutamine, high glucose availability still activates MondoA, thereby inhibiting TXNIP, and insulin is known to stimulate glutamine transport into the muscles [51]. This was observed also in human adipocytes [11]. In addition, the more marked cellular adaptations (i.e. MondoA and ACC) observed in vitro compared with those detected in vivo are likely also due to the higher and chronic glucose exposure. In our in vitro study, we have used 15 mmol/L (270 mg/dL) of glucose, a concentration observable in post-prandial T2DM patients [52, 53]. Conversely, in our in vivo study, healthy subjects were exposed to circa 65 g of glucose twice a day causing two blood glucose peaks of around 7–8 mmol/L. Importantly, the amount of SSB that we have used in our study does not differ much (760 mL) from the mean value of soft drink consumption per capita per day in the United Kingdom (~650 mL) in 2010 [54]. In real life, SSB users are often exposed to similar sugar levels for years; making our in vitro results a good indication of what might occur in the long run. However, care must be taken when drawing conclusions; in fact, in this study we used a commercially available, glucose syrup-based SSB, but more and more frequently, even in Europe, SSBs are made with high fructose corn syrups (glucose and fructose); thus, the role of fructose on metabolism, next to the one played by glucose investigated here, should not be underestimated.
It has been shown that SSBs play an important role in the aetiology of obesity and that they may increase the risk of T2DM [14–16]. The results presented in present article, on the metabolic effects of SSBs, along with the effects of SSBs on taste perception [21] add experimental evidence in favour of an important role played by SSBs in the development of obesity and T2DM. The alterations that we have found as a result of the SSB supplementation do not only include metabolic responses based on the altered substrate availability, but also transcriptional responses that could lead to chronic alterations in metabolism. The reasons why periods of high glucose availability can achieve similar metabolic responses to chronic hyperglycaemia might be found on various levels. However, we suggest that carbohydrate dependent signalling systems such as MondoA in muscle, and possibly MondoB in liver, might contribute to our findings. Further evidence, such as larger and if possible longer trials, is needed to consolidate and clarify the role of MondoA in the metabolic shift caused by SSB consumption. In conclusion, 4 weeks of SSB supplementation shifted substrate metabolism towards carbohydrates, increasing glycolytic and lipogenic gene expression in muscle.
References
Chopra M, Galbraith S, Darnton-Hill I (2002) A global response to a global problem: the epidemic of overnutrition. Bull World Health Organ 80:952–958
Kahn CR (1994) Banting Lecture. Insulin action, diabetogenes, and the cause of type II diabetes. Diabetes 43:1066–1084
Corpeleijn E, Saris WH, Blaak EE (2009) Metabolic flexibility in the development of insulin resistance and type 2 diabetes: effects of lifestyle. Obes Rev 10:178–193
Kelley DE, Mandarino LJ (2000) Fuel selection in human skeletal muscle in insulin resistance: a reexamination. Diabetes 49:677–683
Kelley DE, Simoneau JA (1994) Impaired free fatty acid utilization by skeletal muscle in non-insulin-dependent diabetes mellitus. J Clin Invest 94:2349–2356
Simoneau JA, Kelley DE (1997) Altered glycolytic and oxidative capacities of skeletal muscle contribute to insulin resistance in NIDDM. J Appl Physiol 83:166–171
Lowell BB, Shulman GI (2005) Mitochondrial dysfunction and type 2 diabetes. Science 307:384–387
Gaster M, Staehr P, Beck-Nielsen H, Schroder HD, Handberg A (2001) GLUT4 is reduced in slow muscle fibers of type 2 diabetic patients: is insulin resistance in type 2 diabetes a slow, type 1 fiber disease? Diabetes 50:1324–1329
Tanner CJ, Barakat HA, Dohm GL, Pories WJ, MacDonald KG, Cunningham PR, Swanson MS, Houmard JA (2002) Muscle fiber type is associated with obesity and weight loss. Am J Physiol Endocrinol Metab 282:E1191–E1196
Ellis BA, Poynten A, Lowy AJ, Furler SM, Chisholm DJ, Kraegen EW, Cooney GJ (2000) Long-chain acyl-CoA esters as indicators of lipid metabolism and insulin sensitivity in rat and human muscle. Am J Physiol Endocrinol Metab 279:E554–E560
Parikh H, Carlsson E, Chutkow WA, Johansson LE, Storgaard H, Poulsen P, Saxena R, Ladd C, Schulze PC, Mazzini MJ, Jensen CB, Krook A, Bjornholm M, Tornqvist H, Zierath JR, Ridderstrale M, Altshuler D, Lee RT, Vaag A, Groop LC, Mootha VK (2007) TXNIP regulates peripheral glucose metabolism in humans. PLoS Med 4:e158
Stoltzman CA, Peterson CW, Breen KT, Muoio DM, Billin AN, Ayer DE (2008) Glucose sensing by MondoA:Mlx complexes: a role for hexokinases and direct regulation of thioredoxin-interacting protein expression. Proc Natl Acad Sci USA 105:6912–6917
Hanke N, Scheibe RJ, Manukjan G, Ewers D, Umeda PK, Chang KC, Kubis HP, Gros G, Meissner JD (2011) Gene regulation mediating fiber-type transformation in skeletal muscle cells is partly glucose- and ChREBP-dependent. Biochim Biophys Acta 1813:377–389
Hu FB, Malik VS (2010) Sugar-sweetened beverages and risk of obesity and type 2 diabetes: epidemiologic evidence. Physiol Behav 100:47–54
Malik VS, Popkin BM, Bray GA, Despres JP, Hu FB (2010) Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 121:1356–1364
Malik VS, Popkin BM, Bray GA, Despres JP, Willett WC, Hu FB (2010) Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: a meta-analysis. Diabetes Care 33:2477–2483
Mattes RD, Shikany JM, Kaiser KA, Allison DB (2011) Nutritively sweetened beverage consumption and body weight: a systematic review and meta-analysis of randomized experiments. Obes Rev 12:346–365
Sans CL, Satterwhite DJ, Stoltzman CA, Breen KT, Ayer DE (2006) MondoA-Mlx heterodimers are candidate sensors of cellular energy status: mitochondrial localization and direct regulation of glycolysis. Mol Cell Biol 26:4863–4871
Billin AN, Eilers AL, Coulter KL, Logan JS, Ayer DE (2000) MondoA, a novel basic helix-loop-helix-leucine zipper transcriptional activator that constitutes a positive branch of a max-like network. Mol Cell Biol 20:8845–8854
Gibson R (1993) Nutritional assessment. A laboratory manual. Oxford University Press, New York
Sartor F, Donaldson LF, Markland DA, Loveday H, Jackson MJ, Kubis HP (2011) Taste perception and implicit attitude toward sweet related to body mass index and soft drink supplementation. Appetite 57:237–246
Sartor F, de Morree HM, Matschke V, Marcora SM, Milousis A, Thom JM, Kubis HP (2010) High-intensity exercise and carbohydrate-reduced energy-restricted diet in obese individuals. Eur J Appl Physiol 110:893–903
WHO (1999) Definition, diagnostic and classification of diabetes mellitus and its complications. In: Report of a WHO Consultation. World Health Organization, Geneva
da Rocha EE, Alves VG, da Fonseca RB (2006) Indirect calorimetry: methodology, instruments and clinical application. Curr Opin Clin Nutr Metab Care 9:247–256
Frayn KN (1983) Calculation of substrate oxidation rates in vivo from gaseous exchange. J Appl Physiol 55:628–634
Reiser S, Bohn E, Hallfrisch J, Michaelis OEt, Keeney M, Prather ES (1981) Serum insulin and glucose in hyperinsulinemic subjects fed three different levels of sucrose. Am J Clin Nutr 34:2348–2358
Reiser S, Handler HB, Gardner LB, Hallfrisch JG, Michaelis OEt, Prather ES (1979) Isocaloric exchange of dietary starch and sucrose in humans. II. Effect on fasting blood insulin, glucose, and glucagon and on insulin and glucose response to a sucrose load. Am J Clin Nutr 32:2206–2216
Black SE, Mitchell E, Freedson PS, Chipkin SR, Braun B (2005) Improved insulin action following short-term exercise training: role of energy and carbohydrate balance. J Appl Physiol 99:2285–2293
Nilsson A, Granfeldt Y, Ostman E, Preston T, Bjorck I (2006) Effects of GI and content of indigestible carbohydrates of cereal-based evening meals on glucose tolerance at a subsequent standardised breakfast. Eur J Clin Nutr 60:1092–1099
Stevenson E, Williams C, Nute M (2005) The influence of the glycaemic index of breakfast and lunch on substrate utilisation during the postprandial periods and subsequent exercise. Br J Nutr 93:885–893
Wolever TM, Jenkins DJ, Ocana AM, Rao VA, Collier GR (1988) Second-meal effect: low-glycemic-index foods eaten at dinner improve subsequent breakfast glycemic response. Am J Clin Nutr 48:1041–1047
Acheson KJ, Schutz Y, Bessard T, Anantharaman K, Flatt JP, Jequier E (1988) Glycogen storage capacity and de novo lipogenesis during massive carbohydrate overfeeding in man. Am J Clin Nutr 48:240–247
Aitken JC, Thompson J (1989) The effects of dietary manipulation upon the respiratory exchange ratio as a predictor of maximum oxygen uptake during fixed term maximal incremental exercise in man. Eur J Appl Physiol Occup Physiol 58:722–727
Horowitz JF, Mora-Rodriguez R, Byerley LO, Coyle EF (1997) Lipolytic suppression following carbohydrate ingestion limits fat oxidation during exercise. Am J Physiol 273:E768–E775
Trenell MI, Stevenson E, Stockmann K, Brand-Miller J (2008) Effect of high and low glycaemic index recovery diets on intramuscular lipid oxidation during aerobic exercise. Br J Nutr 99:326–332
Stevenson E, Williams C, Nute M, Humphrey L, Witard O (2008) Influence of the glycaemic index of an evening meal on substrate oxidation following breakfast and during exercise the next day in healthy women. Eur J Clin Nutr 62:608–616
Isken F, Klaus S, Petzke KJ, Loddenkemper C, Pfeiffer AF, Weickert MO (2010) Impairment of fat oxidation under high- vs. low-glycemic index diet occurs before the development of an obese phenotype. Am J Physiol Endocrinol Metab 298:E287–E295
Roberts R, Bickerton AS, Fielding BA, Blaak EE, Wagenmakers AJ, Chong MF, Gilbert M, Karpe F, Frayn KN (2008) Reduced oxidation of dietary fat after a short term high-carbohydrate diet. Am J Clin Nutr 87:824–831
He J, Kelley DE (2004) Muscle glycogen content in type 2 diabetes mellitus. Am J Physiol Endocrinol Metab 287:E1002–E1007
Merla G, Howald C, Antonarakis SE, Reymond A (2004) The subcellular localization of the ChoRE-binding protein, encoded by the Williams-Beuren syndrome critical region gene 14, is regulated by 14–3-3. Hum Mol Genet 13:1505–1514
Kabashima T, Kawaguchi T, Wadzinski BE, Uyeda K (2003) Xylulose 5-phosphate mediates glucose-induced lipogenesis by xylulose 5-phosphate-activated protein phosphatase in rat liver. Proc Natl Acad Sci USA 100:5107–5112
Puigserver P, Spiegelman BM (2003) Peroxisome proliferator-activated receptor-gamma coactivator 1 alpha (PGC-1 alpha): transcriptional coactivator and metabolic regulator. Endocr Rev 24:78–90
Kubis HP, Hanke N, Scheibe RJ, Meissner JD, Gros G (2003) Ca2 + transients activate calcineurin/NFATc1 and initiate fast-to-slow transformation in a primary skeletal muscle culture. Am J Physiol Cell Physiol 285:C56–C63
Hanke N, Meissner JD, Scheibe RJ, Endeward V, Gros G, Kubis HP (2008) Metabolic transformation of rabbit skeletal muscle cells in primary culture in response to low glucose. Biochim Biophys Acta 1783:813–825
Pilegaard H, Keller C, Steensberg A, Helge JW, Pedersen BK, Saltin B, Neufer PD (2002) Influence of pre-exercise muscle glycogen content on exercise-induced transcriptional regulation of metabolic genes. J Physiol 541:261–271
Pick A, Clark J, Kubstrup C, Levisetti M, Pugh W, Bonner-Weir S, Polonsky KS (1998) Role of apoptosis in failure of beta-cell mass compensation for insulin resistance and beta-cell defects in the male Zucker diabetic fatty rat. Diabetes 47:358–364
Arner P (2005) Insulin resistance in type 2 diabetes—role of the adipokines. Curr Mol Med 5:333–339
Chutkow WA, Patwari P, Yoshioka J, Lee RT (2008) Thioredoxin-interacting protein (Txnip) is a critical regulator of hepatic glucose production. J Biol Chem 283:2397–2406
Muoio DM (2007) TXNIP links redox circuitry to glucose control. Cell Metab 5:412–414
Kaadige MR, Looper RE, Kamalanaadhan S, Ayer DE (2009) Glutamine-dependent anapleurosis dictates glucose uptake and cell growth by regulating MondoA transcriptional activity. Proc Natl Acad Sci USA 106:14878–14883
Rennie MJ, Ahmed A, Khogali SE, Low SY, Hundal HS, Taylor PM (1996) Glutamine metabolism and transport in skeletal muscle and heart and their clinical relevance. J Nutr 126:1142S–1149S
Matsuda M, DeFronzo RA (1999) Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care 22:1462–1470
Monnier L, Mas E, Ginet C, Michel F, Villon L, Cristol JP, Colette C (2006) Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 295:1681–1687
BSDA (2011) The 2011 UK soft drinks report: by popular demand. In: British Soft Drinks Association. http://www.britishsoftdrinks.com
Acknowledgments
We would like to thank Dr Matschke for her help with the data collection and Dr Caspari for letting us use part of the NWCRF Institute facilities. We are also grateful to Dr de Morree for proofreading the manuscript. All authors read and approved the final manuscript.
Conflict of interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
394_2012_401_MOESM1_ESM.pdf
Supplementary Figure 1. Myocytes grown on microcarriers for 14 days in culture, photographed at ×20 magnficication (B,D) and seeded in conventional culture flasks, 40X magnification (A,C). (PDF 4480 kb)
Rights and permissions
About this article
Cite this article
Sartor, F., Jackson, M.J., Squillace, C. et al. Adaptive metabolic response to 4 weeks of sugar-sweetened beverage consumption in healthy, lightly active individuals and chronic high glucose availability in primary human myotubes. Eur J Nutr 52, 937–948 (2013). https://doi.org/10.1007/s00394-012-0401-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-012-0401-x