
Abstract
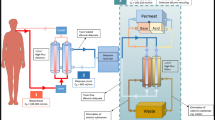
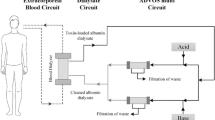
The Molecular Adsorbent Recirculating System (MARS) has been proven to prolong survival in patients with acute on chronic liver failure. MARS is a liver support therapy that is based on a modified dialysis using an albumin-containing dialysate, which is recirculated and on-line perfused through charcoal and anion exchanger columns. It allows the selective removal of albumin-bound substances from the blood.
Despite advances in medical therapy and technology, the prognosis of patients with cardiogenic shock remains poor. Mortality rates are as high as 80%, often due to persistent multiple organ failure. To find out whether patients with hypoxic liver failure following cardiogenic shock after cardiac surgery might benefit from MARS, we performed a prospective, randomized, controlled, single center study. The primary objective was to prove that MARS improves survival during ICU stay.
A total of 40 patients were included between 8/00 and 6/02; 20 patients in the MARS group (M) and 20 in the standard therapy group without MARS treatment (ST). All had bilirubin levels >8 mg/dl. Both groups had a similar risk profile. The M patients received MARS for 3 consecutive days – if bilirubin was still >6 mg/dl afterwards, MARS was continued. The ST group received conventional therapy. For ethical reasons, ST patients with increasing bilirubin levels >15 mg/dl later received MARS treatments (SM, n=13).
Results
We had 8 ICU survivors in the M group (40%) (n=20), compared to 1 (14.3%; p=0.438) in the group never treated with MARS (n=7). We conclude that despite the limited number of patients included in this analysis, MARS can be recommended for patients with acute, hypoxic liver failure as it can prolong survival. Further studies in similar patient cohorts are needed to verify these findings.
Zusammenfassung
Die MARS-Lebertherapie (Molecular Adsorbent Recirculating System) konnte zeigen, dass das Überleben von Patienten mit einer akuten Dekompensation einer chronischen Lebererkrankung durch den Einsatz der Therapie verlängert wird. MARS ist eine extrakorporale Behandlung, bei der als Dialysat Humanalbumin verwendet wird und die so albumingebundene Substanzen aus dem Blut entfernen kann. Das Albumin wird über in einem geschlossenen Kreislauf über Aktivkohle- und Anionenadsorber geleitet und so für eine kontinuierliche Behandlung gereinigt.
Trotz der Fortschritte der Technologie und der modernen Intensivtherapie, ist die Überlebensprognose von Patienten mit kardiogenem Schock schlecht. Die Mortalitätsrate beträgt bis zu 80%, häufig bedingt durch anhaltendes Multiorganversagen. Um herauszufinden, ob diese Patienten mit hypoxischem Leberversagen nach Herzoperationen von MARS profitieren, wurde eine prospektive, kontrollierte, randomisierte Studie durchgeführt. Als primäres Zielkriterium galt das Überleben auf der Intensivstation.
Im Zeitraum von 8/00 bis 6/02 wurden 40 Patienten in die Studie eingeschlossen; 20 in die MARSGruppe (M) und 20 in die Gruppe mit Standardtherapie (ST). Alle wiesen Bilirubinspiegel >8 mg/dl auf. Zwischen den beiden Gruppen zeigten sich bei Einschluss keine wesentlichen Unterschiede. Die M-Gruppe wurde an 3 aufeinander folgenden Tagen mit MARS behandelt. Wenn danach die Bilirubinspiegel >6 mg/dl waren, wurde MARS fortgesetzt. Die STGruppe erhielt intensivmedizinische Standardtherapie. ST-Patienten mit weiter ansteigendem Bilirubin >15 mg/dl erhielten aus ethischen Gründen später MARS (SM Gruppe; n=13).
Ergebnisse
In der M-Gruppe (n=20) gab es 8 Überlebende (40%) auf der Intensivstation, in der Gruppe der Patienten, die niemals mit MARS (KM) behandelt wurden (n=7) nur einen Überlebenden (14,3%) (p=0,438). Trotz der geringen Anzahl von Patienten in dieser Analyse, kann MARS empfohlen werden für die Therapie von akutem hypoxischen Leberversagen, da die Therapie lebensverlängernd sein kann. Weitere Studien sind nötig um diese Ergebnisse zu verifizieren.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Literatur
Mitzner SR, Stange J, Klammt S, Risler T, Erley M, Bader BD, Berger ED, Lauchart W, Peszynski P, Freytag J, Hickstein H, Loock J, Lohr JM, Liebe S, Emmrich J, Korten G, Schmidt R (2000) Improvement of hepatorenal syndrome with exrtracorporeal albumin dialysis MARS: results of a prospective, randomized, controlled clinical trial. Liver Transpl 6(3):277–286
Awad SS, Rich PB, Kolla S, Younger JG, Reickert CA, Downing VP, Bartlett RH (1997) Characteristics of an albumin dialysate hemodiafiltration system for the clearance of unconjugated bilirubin. ASAIO 43:M745–M749
Stange J, Mitzner S, Risler T, Erley CM, Lauchart W, Goehl H, Klammt S, Peszynski P, Freytag J, Hickstein H, Löhr M, Liebe S, Scharek W, Hopt UT, Schmidt R (1999) Molecular Adsorbent Recirculating System (MARS) – Clinical results of a new membrane based blood purification system for bioartificial liver support. Artif Organs 23:319–330
Awad SS, Sawada S, Soldes OS, Rich PB, Klein R, Alarcon WH, Bartlett RH (1999) Can the clearance of tumor necrosis factor alpha and interleukin 6 be enhanced using an albumin dialysate hemodiafiltration system? ASAIO 45:47–49
Stange J, Mitzner S (1996) A carriermediated transport of toxins in a hybrid membrane. Internat J Artif Organs 19:677–691
Goldberg R, Gore J, Alpert J et al (1991) Cardiogenic shock after acute myocardial Incidence infarction and mortality from a community wide perspective, 1975–1988. N Engl J Med 325:1117–1122
Hands ME, Rutherford JD, Muller JE, et al (1989) The in-hospital development of cardiogenic shock after myocardial infarction. Incidence, predictors of occurrence, outcome and prognostic factors. J Am Coll Cardiol 14:40–46
Leor J, Goldbourt U, Reicher-Riess H, Kaplinsky E, Behar S, SPRINT Study Group (1993) Cardiogenic Shock complicating acute myocardial infarction in patients without heart failure on admission: Incidence, risk factors and outcome. Am J Med 94:265–273
Califf RM, Bengston JR (1994) Cardiogenic shock. N Engl J Med 330:1724–1730
Rahmann TM, Hodgson HJF (1999) Review article: liver support systems in acute hepatic failure. Aliment Pharmacol Ther 13:1255–1272
Hughes RD, Courtney JM (1997) Dialysis/adsorption techniques for acute liver failure, in: Lee W and Williams R (eds), Acute liver failure, Cambridge, New York, Melbourne, Cambridge University Press, pp 278–284
Kragh-Hansen U (1990) Structure and ligand binding properties of human serum albumin. Dan Med BULL 37:57–84
Mitzner SR, Stange J, Klammt S, Peszynski P, Schmidt R, Noeldge-Schomburg G (2001) Extracorporeal Detoxification Using the Molecular Recirculating System for Critically ill Patients with Liver Failure. J Am Soc Nephrol 12:S75–S82
Heemann U, Treichel U, Loock J, Philipp T, Gerken G, Malago M, Klammt S, Loehr M, Liebe S, Mitzner S, Schmidt R, Stange J (2002) Albumin Dialysis in Cirrhosis with Superimposed Acute Liver Injury: A Prospective, Controlled Study. Hepatology 36:949–958
Hassanein T, Tofteng F, Brown RS, McGuire BM, Lynch P, Mehta R, Larsen FS, Gornbein J, Sange S, Blei AT (2004) Efficacy of Albumin Dialysis (MARS) in Patients with Cirrhosis and Advanced Grades of Hepatic Encephalopathy: A Prospective, Controlled, Randomized Multicenter Trial (Abstract AASLD)
Schmidt LE, Sørensen VR, Svendsen LB, Hansen BA, Larsen FS (2001) Hemodynamic changes during a single treatment with the Molecular Adsorbent Recirculating System in patients with Acute-on-Chronic Liver Failure. Liver Transpl 7:1034–1039
Schmidt LE, Wang LP, Hansen BA, Larsen FS (2003) Systemic hemodynamic effects of treatment with the molecular adsorbents recirculating system in patients with hyperacute liver failure: A prospective controlled trial. Liver Transpl 9(3):290–297
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
El Banayosy, A., Cobaugh, D., Pauly, A. et al. Albumindialyse bei Patienten mit sekundärem Leberversagen nach kardiogenem Schock. Intensivmed 44, 149–157 (2007). https://doi.org/10.1007/s00390-007-0744-3
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s00390-007-0744-3