
Abstract
Background
There is a consistently reported relationship between the incidence of colon cancer and obesity. It is thought that adipose tissue, particularly visceral fat, which secretes systemic factors that alter immunological, metabolic and endocrine milieu and promotes insulin resistance by producing adipocytokines, is important in cancer progression. Systemic high concentrations of adipocytokines, such as tumour necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), and glucocorticoid metabolism-related genes have been associated with gastrointestinal cancer. However, limited information exists about the expression of these cytokines within tumour tissue.
Material and methods
mRNA expression of TNF-α, IL-6,IL-8, IL-10, IL-1RN, glucocorticoid receptor alpha (GR-α), 11β-hydroxysteroid dehydrogenase type 1 (11β-HSD1), plasminogen activator inhibitor-1 (PAI-1), Slug, vimentin, Snail and E-cadherin was analysed in paired samples of tumour tissue and normal mucosa in 60 surgical patients for Dukes B and C colorectal adenocarcinomas using quantitative reverse transcription PCR and microarray technology. The mRNA expression level of analysed genes was compared between tumour tissue and normal mucosa from the same patients, and a correlation to mRNA expression of E-cadherin in the same tissue samples was also performed.
Results
A highly significant difference in mRNA expression level of several of the analysed genes was observed between tumour tissue and the normal intestinal mucosa. Inverse correlation between mRNA expression of 11βHSD1, IL-6, GR-α and PAI-1 on one hand and mRNA expression of E-cadherin on the other hand was observed.
Conclusion
Results show that the adipocytokines and glucocorticoid metabolism-related genes are overexpressed in colorectal adenocarcinomas, and expression of these genes is associated with the downregulation of E-cadherin mRNA, connecting these genes to carcinogenesis and progression of colorectal cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Epidemiological studies have provided evidence for the association of obesity with cancer [1–3]. The adipose tissue, particularly visceral fat, has been linked to gastrointestinal cancer, including colorectal cancer [4]. Insulin resistance and metabolic syndrome are thought to link obesity and carcinogenesis, since cohort studies have demonstrated an increased risk of colorectal cancer in those with insulin resistance and metabolic syndrome [5–7]. Levels of adipose tissue affect the body’s glucose management, and adipocytokines are involved in the pathogenesis of insulin resistance [8, 9]. High concentrations of cytokines produced by adipose tissue, such as tumour necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), IL-β1, and low concentrations of adiponectin lead to chronic hyperinsulinemia.
Adipocyte-conditioned media can promote tumourigenesis in cancer cells by increasing cell proliferation, invasive potential and angiogenesis. In addition, these media can induce crosstalk between cancer cells and the surrounding extracellular matrix [10]. These actions are thought to be mediated by the production of biologically active proteins such as adiponectin and leptin and by cytokines including TNF-α, IL-6, IL-8, IL-10 and IL-1 receptor agonists, collectively termed adipocytokines. Increased expression of adipocytokines is associated with tumour invasiveness. One of the required steps in this process of tumour invasiveness is epithelial–mesenchymal transition (EMT) of the tumour cells. The hallmark of EMT is its downregulation of E-cadherin. EMT plays an important role in normal development and in cancer progression [11]. This process involves morphological and biochemical changes that result in the loss of the epithelial marker E-cadherin and the gain of mesenchymal markers, such as vimentin, Snail or Slug.
Other known factors in cancer progression are linked to matrix metalloproteinases (MMPs), such as the fibrinolytic plasminogen system (PS). PS is also important in the carcinogenic process through its inhibition and activation in fibrosis development.
Central obesity is important in the development and progression of colorectal cancer. Glucocorticoids have a profound effect on central obesity and insulin resistance. Since changes in the tumour milieu at the local site is very important in tumour invasiveness, we wanted to evaluate mRNA expression of genes related to glucocorticoid metabolism (glucocorticoid receptor alpha (GR-α), converting enzyme 11β-hydroxysteroid dehydrogenase type 1 (11β-HSD1) and plasminogen activator inhibitor-1 (PAI-1)) as well as adipocytokines (TNF-α, IL-6, IL-8, IL-10 and IL-1RN) in the colorectal adenocarcinomas and corresponding normal mucosa from same patient. We also wanted to correlate mRNA expression of these genes in the tumour tissue to mRNA expression of E-cadherin in the same tissue specimens, since alterations in E-cadherin gene expression is thought to be important in the metastatic process during its implication in EMT.
Another glucocorticoid metabolism-related gene which has been shown to be overexpressed in colorectal adenocarcinomas is PAI-1. PAI-1 is known to be involved in insulin metabolism but has also been shown to be overexpressed in colorectal adenocarcinomas. Overexpression of PAI-1 has been shown to be associated with poor prognosis of colorectal cancer patients [12, 13], although theoretically overexpression of PAI-1 should prevent metastases. We wanted to evaluate whether mRNA expression of PAI-1 may also be correlated to the mRNA expression of E-cadherin, explaining, in part, why PAI-1 overexpression in the tumour tissue may lead to poor prognosis of colorectal cancer patients.
Materials and methods
Sixty paired tumours and normal mucosa from patients operated on for Dukes B and C colorectal adenocarcinomas were analysed, using quantitative reverse transcription PCR (qRT-PCR) and microarray technology, for mRNA expression of TNF-α, IL-6, Il-8, IL-10, IL-1RN, GR-α, 11β-HSD1, PAI-1, vimentin, Slug and Snail and E-cadherin. The median patient age was 64 years (range 34–83 years) for rectal adenocarcinomas (23 Dukes B, and 17 Dukes C) and 63 years (range 47–71 years) for colonic adenocarcinomas (8 Dukes B, and 9 Dukes C).
None of the patients had known hereditary cancers or received preoperatively neoadjuvant treatment. Tumour tissue and corresponding normal mucosa was taken at the time of surgery and preserved in RNAlater (Ambion Inc., Austin, TX). The specimens were kept at 4 °C for less than 2 weeks before removing the RNAlater. The tissue specimens were stored at −80 °C. The tumours were all classified as Dukes B or C colonic or rectal tumours. Two pathologists independently performed the staging, without any discrepancies in their classification. Only biopsies that contained between 60 and 100 % tumour tissue (median 80 %) were included in the study. This was confirmed in tissue taken as a section next to the tumour tissue used for RNA isolation. Rectum was defined to extend to 15 cm from the anal canal [14].
RNA isolation
Total RNA was isolated from frozen samples according to the protocol of TRIzol Reagent (Life Technologies, Inc., Gaithersburg, MD) and RNeasy Mini Kit (Qiagen, Hilden, Germany), with DNase treatment. RNA was dissolved in nuclease-free water (Ambion Inc.). Tissue samples (25–100 mg) were homogenised in 1.2 ml of TRIzol Reagent with a MixerMill MM301 (Retsch GMbH & Co., Haan, Germany). The quality and quantity of total isolated RNA were determined using Agilent’s 2100 Bioanalyser with RNA Nano LabChip (Agilent Technologies, Palo Alto, CA) and the NanoDrop ND-1000 Spectrophotometer (NanoDrop Technologies, Wilmington, DE). Samples that showed RNA degradation were not included in the study. The purified RNA was stored at −80 °C.
Oligo microarray processing
Total RNA was amplified with the Amino Allyl MessageAmp II aRNA Amplification Kit (Ambion Inc.). The quality and quantity of the amplified aRNA were determined using Agilent’s 2100 Bioanalyser. Five micrograms of amplified aRNA was indirectly labelled with a Cy5 or Cy3 Mono-reactive Dye Pack (Amersham Biosciences, Buckinghamshire, UK), as described in the Ambion’s RNA amplification protocol. The labelled aRNA was checked on the NanoDrop ND-1000 Spectrophotometer. To minimise a potential dye effect, half of the samples were labelled with Cy5 and the other half with Cy3. Universal Human Reference RNA (UHR-RNA) (Stratagene, La Jolla, CA) was used as a common reference. UHR-RNA was amplified with the same procedure as the other samples, and the same batch of amplified UHR-RNA was used for all these experiments. Microarray hybridisation and processing were performed using Agilent’s Human Whole Genome Oligo Microarrays (44 K), which contains ~41,000 probes of genes and transcripts, following the manufacturer’s 60-mer oligo microarray processing protocol. Briefly, the slides were hybridised with 15 pmol of labelled amplified tumour aRNA and 15 pmol of labelled amplified UHR-RNA aRNA for 17 h in a rotating hybridisation oven. The slides were subsequently washed using a 6× SSC and 0.0005 % Triton X-102 wash solution for 10 min at room temperature followed by a second wash with a 0.1× SSC and 0.0005 % Triton X-102 solution for 5 min at 4 °C. The slides were dried in a spin centrifuge and scanned using an Agilent G2565BA Microarray Scanner (Agilent).
Microarray data analysis
Data collection and quality assessment were performed using Agilent G2567AA Feature Extraction software v8.5 with default parameters. Further data analysis was performed using J-Express Pro v2.7 (MolMine, Bergen, Norway). Poor spots flagged by Feature Extraction were filtered out. In order to reduce colour bias and other technical noise, Lowess normalisation was used, and missing values were calculated using the LSImpute function (maximum 30 % missing values allowed). Differentially expressed genes were found using significance analysis of microarrays [15], as implemented in J-Express with 1,000 permutations and false discovery rate (FDR) <10. Gene expression profiles were compared between the two groups using principal component analysis and hierarchical clustering.
Quantitative reverse transcription PCR
Three micrograms of total RNA was reverse transcribed into complementary DNA (cDNA) using Invitrogen’s SuperScript First-Strand Synthesis System for RT-PCR with Oligo (dT) primer (Invitrogen, Carlsbad, CA). Primers and probes for 11β-HSD1 and GR-α have previously been described and were purchased from the Thermo Electron Corporation. TaqMan gene expression assays for PAI-1, TNF-α, IL-6 and E-cadherin were purchased from Applied Biosystems (Carlsbad, CA; serial numbers: Hs01126605_g1, Hs01113624_g1, Hs99999032_m1 and Hs01023894_m1). The assay for GAPDH was purchased from Integrated DNA Technologies (Coralville, IA; assay ID: Hs.PT.47.18816943). The final concentration of the TaqMan gene expression assay used was 900 nM for each primer and 250 nM for each probe. Both primers and probes of 11β-HSD1 and GR-α had a concentration of 10 μM. Forward and reverse primers (2.5 μl) and 0.625 μl of the probe were used in a final volume of 25 μl. Fifteen nanograms of cDNA was applied per reaction and run in duplicates and on an ABI Prism 7900HT Sequence Detection System, using ABI Prism SDS2.3 software for evaluation (Applied Biosystems). Expression levels were quantified by generating a five-point serial standard curve using pooled cDNA from the samples. The expression levels of target genes were normalised to the level of the TPB reference gene. The microarray data have been deposited in ArrayExpress (http://www.ebi.ac.uk/arrayexpress/), accession no E-MTAB-833.
qRT-PCR statistical analyses
Comparisons of each gene’s mRNA expression between colorectal tumour and normal mucosa samples were performed by paired Wilcoxon’s rank sum tests for non-parametric data. Statistical analyses were performed using the R statistical software. A two-sided p value of <0.05 was considered statistically significant.
Results
Gene expression profiling
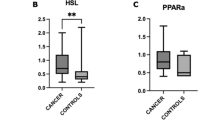
In the microarray study, we identified significant (FDR <10) differentially expressed genes compared to normal mucosa that characterised malignant tumours in the colon and rectum. There were significantly higher levels of PAI-1, TNF-α, IL-6 and11β-HSD-1 and significantly lower levels of GR-α in tumour tissue compared to normal mucosa (Fig. 1). The qRT-PCR analyses and the DNA microarray analyses showed the same significant differences and tendencies between the adenocarcinomas and their associated normal tissue, although some of the genes analysed did not reach statistical significant (Table 1). There were also significantly different levels of TNF-α between Dukes B adenocarcinomas and Dukes C adenocarcinomas (p = 0.006; Fig. 2). We also evaluated the correlation between mRNA expression of analysed genes and E-cadherin, and we observed a statistically significant inverse correlation between 11β HSD-1, IL-6, GR-α and PAI-1 and E-cadherin (p < 0.005; Table 1). EMT markers such as vimentin, Snail and Slug also showed the same inverse correlation to E-cadherin (Table 2). In addition, there was an internal correlation among upregulation of the different adipocytokines (Table 3).

Mean value of mRNA expression in both colonic and rectal adenocarinomas and normal mucosa by RT-qPCR. mRNA expressions are shown relative to reference gene glyceraldehyde-3 phosphate dehydrogenase (GAPDH). Data are mean ± SE. p values are from pairwise Wilcoxon’s tests. Except for GR-α all the genes are upregulated in tumour tissue

Different mRNA expressions in colorectal tissue and normal mucosa by RT-qPCR. The upper line shows the differences between Stadium Dukes B (B) and Stadium Dukes C (C). The lower line shows the differences between colonic adenocarcinomas (Col) and rectal adenocarcinomas (Rec) by qRT-PCR. There is significant difference in TNF-α between Dukes B and Dukes C
Discussion
In the present study, we analysed the mRNA expression of TNF-α, IL-6, IL-8, IL-10, IL-1RN, GR-α, 11β-HSD-1, PAI-1, Snail, vimentin, Slug and E-cadherin in tumour tissue and corresponding normal mucosa from patients operated on for Dukes B and C colorectal cancer. TNF-α, IL-6, 11β-HSD-1 and PAI-1 were upregulated in the tumour tissue compared to the normal mucosa, indicating an important role played by these genes in the pathogenesis and progression of colorectal carcinomas.
The expression of adipocytokines and metabolic active genes analysed in the present study were correlated to the mRNA expression of E-cadherin to evaluate their possible role in the progression of colorectal cancer. We chose E-cadherin gene since downregulation of E-cadherin plays an important role in the metastatic process. We observed an inverse correlation between mRNA expression of several of the analysed genes and mRNA expression of E-cadherin, a correlation which has not been shown previously. To further explore the role of E-cadherin in the metastatic process, we analysed mRNA expression of some of the EMT-related genes (vimentin, Snail and Slug) and compared to mRNA expression of E-cadherin gene in the same tumour tissue. We observed a statistically significant inverse correlation between mRNA expression of EMT-related genes and mRNA expression of E-cadherin gene (Table 2). Transforming growth factor-β (TGF-β) gene plays an important role in the EMT process [16], and the effect of TGF-β on EMT is accelerated by induction TNF-α. Another inflammatory cytokine that plays an important role in colorectal carcinogenesis is IL-6, a multifunctional cytokine involved in the response to injury or infection, immune response, inflammation and haematopoiesis. Its deregulation impacts several diseases, including gastrointestinal cancer [17–19]. IL-6 exhibits growth-stimulatory effects on a panel of colon cancer cell lines [20]. It has also been observed that IL-6 expression and its growth-stimulating effect is more pronounced in metastatic colon cancer cell lines [21], indicating its role in invasion. The present study indicates that the metastatic potential of TNF-α and IL-6 may be due to downregulation of E-cadherin mRNA, since a high expression of these genes was associated with downregulation of E-cadherin mRNA. It is also notable that the expression of TNF-α was different in Dukes B and C tumour stages, indicating an important role of this protein in the metastatic process.
PAI-1 has also a central role in the cancer progression, since the PS is closely linked to TGF-β1 and MMPs through inhibition and activation. The PS consists of two activators: tissue plasminogen activator and urokinase plasminogen activator, as well as two inhibitors: PAI-1 and -2. The balance between activators and inhibitors of the fibrinolytic plasminogen system is important regarding cancer progression. PAI-1 is pivotal in fibrosis development [22, 23], and the PAI-1 gene is activated by radiotherapy [24]. Theoretically, overexpression of PAI-1 should prevent invasiveness, but in clinical and in in vitro studies, overexpression of PAI-1 has been shown to correlate with impaired patient outcome in both breast cancer patients and colorectal cancer patients [25, 26]. An explanation of this effect is lacking in the literature. However, no previous studies have analysed the correlation between the expression of PAI-1 and that of E-cadherin. Results from the present study suggest that the PAI-1 may carry out its metastatic effect during downregulation of E-cadherin, although the exact mechanism by which this would occur is impossible to explore in a clinical study.
There is growing evidence that adipocytokines and glucocorticoids, through an insulin signalling pathway, play a role in the carcinogenesis of gastrointestinal cancers. Overexpression of glucocorticoids leads to impaired insulin sensitivity in skeletal muscle and adipose tissue by its direct effect on insulin signalling pathways, glucose transport and glucose oxidation, and by their indirect effect on lipid metabolism and protein metabolism [26, 27]. The output of glucocorticoids is regulated by glucocorticoid receptors and converting enzyme 11β-HSD1, which functions as an oxyreductase that converts cortisone into cortisol. The provision of cofactor, nicotinamide adenine dinucleotide phosphate, by a second regulatory enzyme, hexose-6-phosphate dehydrogenase, mediates the glucocorticoid receptor (GR) response [28, 29]. However, there are few studies in which the expression of these adipocytokines and glucocorticoids have been analysed in tumour tissue of colorectal adenocarcinomas and in the normal mucosa of the same patient. The results from this present study show that the expression of GR-α is reduced in the tumour, while 11β-HSD-1 is upregulated in the tumour. Overexpression of 11β-HSD1 mRNA was also associated with downregulation of E-cadherin mRNA, indicating an important role of these genes in the progression of colorectal cancer.
As expected, we observed lower, although not significant, mRNA expression of E-cadherin in tumour tissue compared to normal mucosa. We think the reason for that mRNA expression of E-cadherin was not statistically lower in the tumour tissue may be that the group is heterogeneous and small, and since this is an average of mRNA expression among all tumours, the results did not show statistical differences.
In sum, we have in the present study evaluated the mRNA expression of TNF-α, IL-6, IL-8, IL-10, IL-1RN, GR-α, 11β-HSD-1, PAI-1, Snail, Slug and vimentin in colorectal adenocarcinomas and correlated the expression of these genes to the expression of E-cadherin gene. Except for TNF-α, all of the analysed genes showed a strong inverse correlation to the mRNA expression of the E-cadherin gene, indicating a possible mechanism behind the effect of these genes on colorectal carcinogenesis and progression.
References
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371:569–578
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003) Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 348:1625–1638
Calle EE, Kaaks R (2004) Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer 4:579–591
Wajchenberg BL (2000) Subcutaneous and visceral adipose tissue: their relation to the metabolic syndrome. Endocr Rev 21:697–738
Colangelo LA, Gapstur SM, Gann PH, Dyer AR, Liu K (2002) Colorectal cancer mortality and factors related to the insulin resistance syndrome. Cancer Epidemiol Biomarkers Prev 11:385–391
Trevisan M, Liu J, Muti P, Misciagna G, Menotti A, Fucci F (2001) Markers of insulin resistance and colorectal cancer mortality. Cancer Epidemiol Biomarkers Prev 10:937–941
Schoen RE, Tangen CM, Kuller LH, Burke GL, Cushman M, Tracy RP, Dobs A, Savage PJ (1999) Increased blood glucose and insulin, body size, and incident colorectal cancer. J Natl Cancer Inst 91:1147–1154
Fasshauer M, Paschke R (2003) Regulation of adipocytokines and insulin resistance. Diabetologia 46:1594–1603
Rajala MW, Scherer PE (2003) Minireview: The adipocyte—at the crossroads of energy homeostasis, inflammation, and atherosclerosis. Endocrinology 144:3765–3773
Iyengar P, Combs TP, Shah SJ, Gouon-Evans V, Pollard JW, Albanese C, Flanagan L, Tenniswood MP, Guha C, Lisanti MP, Pestell RG, Scherer PE (2003) Adipocyte-secreted factors synergistically promote mammary tumorigenesis through induction of anti-apoptotic transcriptional programs and proto-oncogene stabilization. Oncogene 22:6408–6423
Thiery JP (2002) Epithelial–mesenchymal transitions in tumour progression. Nat Rev Cancer 2:442–454
Loskutoff DJ, Quigley JP (2000) PAI-1, fibrosis, and the elusive provisional fibrin matrix. J Clin Invest 106:1441–1443
Schmitt M, Harbeck N, Thomssen C, Wilhelm O, Magdolen V, Reuning U, Ulm K, Hofler H, Janicke F, Graeff H (1997) Clinical impact of the plasminogen activation system in tumor invasion and metastasis: prognostic relevance and target for therapy. Thromb Haemost 78:285–296
Zhao H, Langerod A, Ji Y, Nowels KW, Nesland JM, Tibshirani R, Bukholm IK, Karesen R, Botstein D, Borresen-Dale AL, Jeffrey SS (2004) Different gene expression patterns in invasive lobular and ductal carcinomas of the breast. Mol Biol Cell 15:2523–2536
Andrews RC, Walker BR (1999) Glucocorticoids and insulin resistance: old hormones, new targets. Clin Sci (Lond) 96:513–523
Qi D, Rodrigues B (2007) Glucocorticoids produce whole body insulin resistance with changes in cardiac metabolism. Am J Physiol Endocrinol Metab 292:E654–E667
Bujalska IJ, Draper N, Michailidou Z, Tomlinson JW, White PC, Chapman KE, Walker EA, Stewart PM (2005) Hexose-6-phosphate dehydrogenase confers oxo-reductase activity upon 11 beta-hydroxysteroid dehydrogenase type 1. J Mol Endocrinol 34:675–684
Draper N, Walker EA, Bujalska IJ, Tomlinson JW, Chalder SM, Arlt W, Lavery GG, Bedendo O, Ray DW, Laing I, Malunowicz E, White PC, Hewison M, Mason PJ, Connell JM, Shackleton CH, Stewart PM (2003) Mutations in the genes encoding 11beta-hydroxysteroid dehydrogenase type 1 and hexose-6-phosphate dehydrogenase interact to cause cortisone reductase deficiency. Nat Genet 34:434–439
Look MP, van Putten WL, Duffy MJ, Harbeck N, Christensen IJ, Thomssen C, Kates R, Spyratos F, Ferno M, Eppenberger-Castori S, Sweep CG, Ulm K, Peyrat JP, Martin PM, Magdelenat H, Brunner N, Duggan C, Lisboa BW, Bendahl PO, Quillien V, Daver A, Ricolleau G, Meijer-Van Gelder ME, Manders P, Fiets WE, Blankenstein MA, Broet P, Romain S, Daxenbichler G, Windbichler G, Cufer T, Borstnar S, Kueng W, Beex LV, Klijn JG, O'Higgins N, Eppenberger U, Janicke F, Schmitt M, Foekens JA (2002) Pooled analysis of prognostic impact of urokinase-type plasminogen activator and its inhibitor PAI-1 in 8377 breast cancer patients. J Natl Cancer Inst 94:116–128
Praus M, Wauterickx K, Collen D, Gerard RD (1999) Reduction of tumor cell migration and metastasis by adenoviral gene transfer of plasminogen activator inhibitors. Gene Ther 6:227–236
Wibe A, Eriksen MT, Syse A, Tretli S, Myrvold HE, Soreide O (2005) Effect of hospital caseload on long-term outcome after standardization of rectal cancer surgery at a national level. Br J Surg 92:217–224
Tusher VG, Tibshirani R, Chu G (2001) Significance analysis of microarrays applied to the ionizing radiation response. Proc Natl Acad Sci USA 98:5116–5121
Hashimoto K, Goto S, Kawano S, Aoki-Kinoshita KF, Ueda N, Hamajima M, Kawasaki T, Kanehisa M (2006) KEGG as a glycome informatics resource. Glycobiology 16:63R–70R
Wakefield LM, Roberts AB (2002) TGF-beta signaling: positive and negative effects on tumorigenesis. Curr Opin Genet Dev 12:22–29
Atreya R, Neurath MF (2005) Involvement of IL-6 in the pathogenesis of inflammatory bowel disease and colon cancer. Clin Rev Allergy Immunol 28:187–196
Lahm H, Petral-Malec D, Yilmaz-Ceyhan A, Fischer JR, Lorenzoni M, Givel JC, Odartchenko N (1992) Growth stimulation of a human colorectal carcinoma cell line by interleukin-1 and -6 and antagonistic effects of transforming growth factor beta 1. Eur J Cancer 28A:1894–1899
Isomoto H, Mott JL, Kobayashi S, Werneburg NW, Bronk SF, Haan S, Gores GJ (2007) Sustained IL-6/STAT-3 signaling in cholangiocarcinoma cells due to SOCS-3 epigenetic silencing. Gastroenterology 132:384–396
Schneider MR, Hoeflich A, Fischer JR, Wolf E, Sordat B, Lahm H (2000) Interleukin-6 stimulates clonogenic growth of primary and metastatic human colon carcinoma cells. Cancer Lett 151:31–38
Herszenyi L, Plebani M, Carraro P, De PM, Roveroni G, Cardin R, Tulassay Z, Naccarato R, Farinati F (1999) The role of cysteine and serine proteases in colorectal carcinoma. Cancer 86:1135–1142
Acknowledgments
This work was supported with grants from Southern and Eastern Norway Regional Health Authority and Østfold Hospital Trust. Torkil Pettersen, MD and Arvid Stordahl, MD were supported by Østfold Hospital Trust, Surgical Department, 1600 Fredrikstad, Norway. Ole Christian Olsen, MD received support from Buskerud Hospital Trust, Surgical Department, 3004 Drammen, Norway and Jan Godøy, MD from Akershus University Hospital, Dept. of Pathology, 1474 Lørenskog, Norway.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Størkson, R.H., Aamodt, R., Vetvik, K.K. et al. mRNA expression of adipocytokines and glucocorticoid-related genes are associated with downregulation of E-cadherin mRNA in colorectal adenocarcinomas. Int J Colorectal Dis 27, 1021–1027 (2012). https://doi.org/10.1007/s00384-012-1442-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-012-1442-6