
Abstract
Background and aims
Several studies over the last 20 years have confirmed the safety and efficacy of strictureplasty in the treatment of obstructive Crohn's disease. However, almost all of these studies use strictureplasty to treat fibrotic strictures: limited resection being preferred to treat active disease strictures. One study dating from 1986 used strictureplasty to treat purely active disease strictures, with disappointing results. No other similar studies have been published. We investigate the complication and recrudescence rates together with the intervention-free intervals in patients undergoing strictureplasty for active disease strictures.
Methods
A retrospective review of 14 patients who underwent strictureplasty either in isolation or in combination with limited resection for active small bowel Crohn's disease between 1996 and 2004 was undertaken.
Results
A total of 73 strictureplasties were carried out. There was no operative mortality; however, one patient subsequently died from metastatic small bowel adenocarcinoma arising from existing Crohn's disease. One patient subsequently developed complications directly attributed to strictureplasty and required further surgery. Three patients developed recrudescent disease and required further surgery in the form of either strictureplasty, limited resection or both. All patients undergoing strictureplasty with resection and over 70% of patients undergoing strictureplasty alone were intervention-free at 41 months. With extended follow-up, the same proportion of patients would remain intervention-free at 70 months or longer.
Conclusions
The use of strictureplasty in active disease strictures is well tolerated and has similar, if not better, recurrence and complication rates when compared with limited resection in patients with similar disease profiles.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Crohn's disease, in the uncomplicated early stages, has traditionally been treated by gastroenterologists using medical therapies such as steroids to induce remission of disease and aminosalicylates or immunosuppressants (or a combination of both) to maintain remission. Surgery is usually reserved for disease that has become complicated by the presence of strictures, fistulae or in cases of sepsis. Such surgery can either be in the form of limited resection of the small bowel or bowel-sparing methods such as strictureplasty. The concept of strictureplasty was first introduced into surgical practice in India by Katariya et al. in the 1970s [1], where it was utilised in the treatment of tuberculous strictures in the large bowel. The use of strictureplasty in Crohn's disease was subsequently documented by Lee and Papaioannou [2], where it was successfully used to treat patients with complicated Crohn's disease in either isolation or conjunction with limited resection.
The safety and efficacy of strictureplasty has been shown in several series [3–8] to be comparable to that of limited resection. Although there were initial doubts regarding the possibility of an increased rate of disease recrudescence following strictureplasty, those doubts have largely proven to be unfounded, as recurrence is not simply limited to the sites of existing disease [9–11]. Strictures in Crohn's disease can be due to fibrosis caused either by the healing process following active disease or by active disease itself. However, almost all published series on the long-term results of strictureplasty have been concerned with strictureplasty for fibrotic strictures. Previously, indications for strictureplasty, such as those put forward by Laureti and Fazio [12], have mentioned that strictureplasty should not be carried out in a segment of small bowel, which is involved by an acute and inflammatory process. However, as surgical experience has increased, this contra-indication has become more relative.
Recent evidence shows that the early use of limited resection in uncomplicated Crohn's disease involving the ileocaecal region can result in a “cure” in approximately 70% of patients [13], i.e. 70% of patients will not require further surgery for Crohn's disease. It should therefore be possible to perform early strictureplasty on patients with a similar disease profile, and this will have the added benefit of being bowel-conserving, thus limiting any reduction in terminal ileal absorption, which may otherwise result from resection. To date, there has been only one published series on strictureplasty for active disease strictures [14]; the results obtained were generally poor. This study analysed the surgical outcome of patients with obstructive Crohn's disease secondary to active disease strictures, who underwent either strictureplasty in isolation or with concomitant small bowel resection. The results have been reviewed with reference to recurrence, re-operation rates and complications.
Materials and methods
The medical records of 14 patients who underwent strictureplasty for active, obstructive jejunoileal Crohn's disease at St. George's Hospital between September 1996 and March 2004 were retrospectively reviewed. Nine patients underwent 55 primary strictureplasties in isolation, while the remaining seven patients had 18 strictureplasties combined with limited resection. We have defined active disease strictures as being those where there was near total obliteration of the bowel lumen through transmural inflammation. This was noted at laparotomy and subsequently demonstrated on histology. In addition, all patients showed systemic signs and symptoms of active Crohn's disease, which, while non-specific, were not likely to be due to other concurrent pathology as none of the patients had coexisting disease. Such signs and symptoms included raised inflammatory markers, leucocytosis, tachycardia and a raised temperature. Two patients (14.3%) had limited resection in addition to strictureplasty to remove fistulae, while one patient (7.1%) underwent laparotomy, strictureplasty and resection for intra-abdominal sepsis. One other patient was operated on both for the presence of complex fistulae and to drain an intra-abdominal abscess. All patients had the standard laboratory tests performed prior to surgery. In addition, all patients received the standard measures to prevent deep-vein thrombosis. Six patients (42.9%) were admitted acutely from the emergency department and stabilised by medical therapy including intravenous hydrocortisone. Surgery was carried out as soon as the patients' condition had been optimised, without necessarily waiting for failure of medical treatment. The remaining patients were admitted electively, and of these, five (35.7%) were on regular oral medication for Crohn's disease.
At laparotomy, strictured sites were identified by palpation. Strictures of 10 cm or less were treated by the Heineke–Mikulicz type of strictureplasty, with the Finney strictureplasty being utilised in strictures over this length. No other form of strictureplasty was utilised. All operations were carried out by the corresponding author at St. George's Hospital, London. A total of 73 strictureplasties were performed of which 15 were of the Finney type and the remaining 58 of the Heineke–Mikulicz type. Two of the strictureplasties were at previous anastomotic sites within the small bowel, while one strictureplasty was at the ileocolic junction. All strictureplasties were hand-sewn using continuous extramucosal single layer 3/0 Vicryl (Ethicon, Edinburgh, UK). Postoperative complications were determined from the records, and details of any further operation required were noted. A summary of patient characteristics is shown in Table 1.
Results
Between 1996 and 2004, 14 patients underwent a total of 73 strictureplasties. The mean number of strictureplasties carried out in one patient at one operation was 5.2 (range 1–14). Figure 1 illustrates the distribution of the maximum number of strictureplasties performed at one operation.

Number of strictureplasties performed per patient
There was no operative mortality. However, one patient died at 33 months from metastatic small bowel adenocarcinoma arising from Crohn's disease (but not a previous site of strictureplasty), which was identified at laparotomy by frozen section of a stricture which was sent for histopathological analysis. The patient subsequently had a computed tomography of the brain and was found to have metastatic deposits. One further patient developed a leak from the strictureplasty suture line at 5 days, which required laparotomy and limited resection of the affected segment. The patient subsequently made a full recovery. All other patients are alive and being followed up at our institution.
Of those patients who had no postoperative complications, two patients (14.3%) required more intensive postoperative care, which was provided in a High Dependency Unit/Intensive Therapy Unit setting. The remainder were nursed on general surgical wards and were discharged home once the usual parameters were met. The median postoperative stay in hospital was 6.9 days (range 4–18).
There were no complications or requirements for further intervention in patients who underwent strictureplasty with concomitant limited resection. In those patients who underwent strictureplasty alone, three patients required further surgery for recrudescent disease, which, for all patients, was a mixture of recurrence at both the original sites of strictureplasty and de novo disease. All of these patients proceeded to have further limited resections combined with strictureplasties.
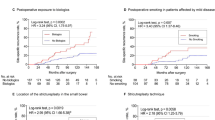
A Kaplan-Meier curve [15] illustrating the proportion of patients remaining intervention-free after first strictureplasty without concomitant resection is shown in Fig. 2, demonstrating that over 70% of patients are intervention-free at our mean follow-up of 41 months.

Kaplan-Meier curve demonstrating the proportion of patients remaining intervention-free after first strictureplasty without concomitant resection
Figure 3 shows the proportion of intervention-free patients after the first operation for recurrent disease. Here, the curve can be seen to fall more steeply and approximately one-third of these patients are intervention-free at 41 months.

Kaplan-Meier curve demonstrating the proportion of patients remaining intervention-free after the first operation for recurrence
Discussion
Strictureplasty has steadily gained favour amongst surgeons as a bowel-sparing alternative to resection in obstructive Crohn's disease, as the risk of subsequent short bowel syndrome is reduced, although one study from Manchester concluded that most cases of short bowel syndrome arose from intra-abdominal complications of Crohn's disease such as sepsis, requiring multiple laparotomies [16]. In their original paper, Lee and Papaioannou put forward the suggestion that strictureplasty should be used in cases of Crohn's disease that are not amenable to surgery [2]. Furthermore, although there was evidence as long-ago as 1988 that early surgery for Crohn's disease may confer long-term benefits with reference to recrudescence rates [17], surgery has still usually been reserved either for complicated cases or in those patients where debilitating side-effects of medication occur [12].
It is important to differentiate between an active disease stricture and the one caused by fibrosis as a result of healing. Although some inflammatory tissue will be present in fibrotic strictures, our study looked at patients whose strictures were composed entirely of inflammatory tissue, with other components of ongoing active disease such as pus, abscesses, fistulae and extravasation of red blood cells in the subserosal tissue. We obtained histology of the strictures in 9 of 14 patients (the other 5 patients were initially treated at another hospital and referred to the senior author as a tertiary referral). All the histology reports obtained confirm the presence of important features associated with active Crohn's disease.
In a study of 181 patients undergoing ileocaecal resection for Crohn's disease over a 23-year period, Kim et al. [13] reported that 69.1% of patients who underwent ileocaecal resection for a single focus of disease, subsequently, had no further recurrence. In another study from Germany [18], 56 patients who were operated on for the first time for Crohn's disease were followed up for 3.5 years, a time-scale comparable with our results. The majority of patients had limited terminal ileal resection. Three patients (5.3%) subsequently required re-operation for recrudescent disease. The authors of both studies concluded that early intervention by limited resection resulted in low re-operation rates. This may be due to a number of factors: early surgery before the patient has become debilitated, and possibly immunosuppressed is likely to result in better wound healing and recovery. Additionally, if terminal ileal disease progresses despite medical therapy being continued, the absorptive capacity diminishes, and the patient's capability to absorb essential nutrients is substantially reduced, leading to poor wound healing and slower recovery time.
In a meta-analysis of 1,825 strictureplasties performed for the first time in more than 500 patients, Tichansky et al. [19] found that the mean rate of re-operation was 18.9% (mean 0–44%). Although few of these studies were utilising strictureplasty alone, most used strictureplasty in conjunction with limited resection. Of the 14 patients that we report on, 3 (21.4%) subsequently needed further surgery for recrudescent disease. However, few published studies on strictureplasty give statistics on intervention-free intervals. Our results show that in patients undergoing strictureplasty alone for the first time in active disease, more than 70% will remain intervention-free at 41 months. Furthermore, if the follow-up period were to be extended, the same proportion of patients would remain intervention-free at 70 months or more. This would suggest that while the safety and efficacy of strictureplasty in complicated Crohn's disease has been well proven, the procedure could also be used early in the treatment on those patients in whom there are no established complications and who would otherwise undergo limited resection for a single focus of inflammation. The intervention-free results obtained are certainly comparable to those obtained with limited resection, and our complication rate is similarly acceptable (3.8%). The first account of strictureplasty for active disease strictures by Kendall et al. in 1986 [14] reported on nine patients, aged between 14 and 36, who underwent 13 operations for mostly diffuse active disease. A total of 45 strictureplasties were performed, mostly in conjunction with limited resections of up to 50 cm in length. Of the nine patients, three (33%) required further surgery for recurrence, while a further three developed recurrence that was managed conservatively. Two patients (22%) developed complications requiring further laparotomy. Overall, only two patients had an uncomplicated postoperative recovery, with no recurrence. The authors concluded that the poor results obtained were probably a reflection of the severity of disease, and that further refinement of the technique would give better results.
Figure 3 shows a Kaplan-Meier curve indicating the disease-free state in patients who underwent surgery for recurrence. It demonstrates that approximately one-third of patients are intervention-free at 30 months. All patients with recrudescent disease underwent more than one subsequent procedure, which suggests that in those patients where recurrence occurred, the disease was of a severe nature. This agrees with the conclusion by Kendall et al. that severe and diffuse disease is less likely to be successful by strictureplasty alone. However, such patients may well benefit from strictureplasty once the disease has become quiescent.
There are several types of strictureplasty in use; we have utilised only the two most common varieties, suitable for strictures up to 25–30 cm in length. It would have been useful to compare the results obtained separately from both types; however, this was not possible for two reasons: firstly, there were far more Heineke–Mikulicz strictureplasties performed than Finney, and, in a small series, direct comparisons would not be valid. Secondly, several patients who had a Finney strictureplasty also underwent concurrent Heineke–Mikulicz strictureplasty; therefore, it would be difficult to perform meaningful comparison of one procedure against the other.
There are newer types of strictureplasty such as the Michelassi strictureplasty [20], which are suitable for strictures that are much longer than this. There is no current published data to confirm whether strictureplasty on active disease strictures of 30 cm or more in length could be safely carried out using similar novel techniques, with acceptable complication and recrudescence rates. We suggest that patient selection is the most important prognostic factor, and that patients with severe jejunoileal disease on maximal medical treatment may not be good candidates for such surgery, as they may already have a poor nutritional state, which does not bode well for postoperative recovery. In contrast, young patients with discrete foci of disease, who have not been subjected to prolonged maintenance of medical therapy, should fare better.
The main limitation of our study is that it is a small series, involving 14 patients undergoing a total of 73 strictureplasties. Although most strictureplasty series involve longer follow-up periods with much larger series of patients, our results need to be compared to those reported by Kendall et al., which involved nine patients. Our results confirm that surgical experience has widened the indications for the use of strictureplasty, from the original use in patients with multiple previous resections in whom further resectional surgery would not be tolerated, to patients in whom there is a single focus of disease where early and judicious use of strictureplasty can bring about long-term intervention-free states. Additionally, we have shown that strictureplasty can safely be carried out in active disease strictures, as well as strictures caused by the formation of fibrotic tissue associated with healing. The population of patients who can thus benefit from strictureplasty is greater, hopefully leading to still fewer incidences of short bowel syndrome. There are, of course, instances where limited resection will still be preferable to strictureplasty, but this will be due to either severity of disease determined clinically, radiologically and biochemically or the length of affected bowel. The latter limitation may become more relative if surgical experience with long-length strictureplasty increases, and good teamworking between physician and surgeon ensures that appropriate patients are operated on early. Overall, our experience suggests that the use of strictureplasty in Crohn's disease should not just be used as a last resort in severely affected individuals but can be a proactive choice by the surgeon in preference to resection, to treat relatively uncomplicated cases that may result in satisfactory long-term remission rates.
References
Katariya RN, Sood S, Rao PG, Rao PL (1977) Stricture-plasty for tubercular strictures of the gastro-intestinal tract. Br J Surg 64:496–498
Lee EC, Papaioannou N (1982) Minimal surgery for chronic obstruction in patients with extensive or universal Crohn's disease. Ann R Coll Surg Engl 64:229–233
Cristaldi M et al (2000) Long-term results and multivariate analysis of prognostic factors in 138 consecutive patients operated on for Crohn's disease using “bowel-sparing” techniques. Am J Surg 179:266–270
Dietz DW et al (2001) Safety and longterm efficacy of strictureplasty in 314 patients with obstructing small bowel Crohn's disease. J Am Coll Surg 192:330–337
Fazio VW, Tjandra JJ (1993) Strictureplasty for Crohn's disease with multiple long strictures. Dis Colon Rectum 36:71–72
Hurst RD, Michelassi F (1998) Strictureplasty for Crohn's disease: techniques and long-term results. World J Surg 22:359–363
Spencer MP, Nelson H, Wolff BG, Dozois RR (1994) Strictureplasty for obstructive Crohn's disease: the Mayo experience. Mayo Clin Proc 69:33–36
Stebbing JF, Jewell DP, Kettlewell MG, Mortensen NJ (1995) Recurrence and reoperation after strictureplasty for obstructive Crohn's disease: long-term results [corrected]. Br J Surg 82:1471–1474
Borley NR et al (2002) Recurrence after abdominal surgery for Crohn's disease: relationship to disease site and surgical procedure. Dis Colon Rectum 45:377–383
Cooper JC, Williams NS (1986) The influence of microscopic disease at the margin of resection on recurrence rates in Crohn's disease. Ann R Coll Surg Engl 68:23–26
Ellis L, Calhoun P, Kaiser DL, Rudolf LE, Hanks JB (1984) Postoperative recurrence in Crohn's disease. The effect of the initial length of bowel resection and operative procedure. Ann Surg 199:340–347
Laureti S, Fazio VW (2000) Obstruction in Crohn's disease: strictureplasty versus resection. Curr Treat Options Gastroenterol 3:191–202
Kim NK et al (1997) Long-term outcome after ileocaecal resection for Crohn's disease. Am Surg 63:627–633
Kendall GP, Hawley PR, Nicholls RJ, Lennard-Jones JE (1986) Strictureplasty. A good operation for small bowel Crohn's disease? Dis Colon Rectum 29:312–316
Kaplan EM, Meier P (1958) Nonparametric observation from incomplete observations. J Am Stat Assoc 53:457–481
Agwunobi AO, Carlson GL, Anderson ID, Irving MH, Scott NA (2001) Mechanisms of intestinal failure in Crohn's disease. Dis Colon Rectum 44:1834–1837
Hulten L (1988) Surgical treatment of Crohn's disease of the small bowel or ileocecum. World J Surg 12:180–185
Lauschke H, Kaminski M, Wiedwald C, Tolba R, Hirner A (2002) Long-term results after surgical therapy of Crohn's disease. Zentralbl Chir 127:706–711
Tichansky D, Cagir B, Yoo E, Marcus SM, Fry RD (2000) Strictureplasty for Crohn's disease: meta-analysis. Dis Colon Rectum 43:911–919
Michelassi F (1996) Side-to-side isoperistaltic strictureplasty for multiple Crohn's strictures. Dis Colon Rectum 39:345–349
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Roy, P., Kumar, D. Strictureplasty for active Crohn's disease. Int J Colorectal Dis 21, 427–432 (2006). https://doi.org/10.1007/s00384-005-0029-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-005-0029-x