
Abstract
Purpose
Trauma is the most important etiology of morbidity and mortality among children. Penetrating injuries to the thorax and abdomen are extremely rare in children. In the present study, we compared the characteristics of patients, management, and outcomes of penetrating thoracic and abdominal trauma in children.
Materials and methods
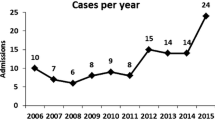
Data from children who were hospitalized for penetrating injuries of the thorax and abdomen from 2006 to 2012 were evaluated retrospectively. These injuries were evaluated with respect to patient details, clinical presentation, circumstances of trauma, management, and outcomes.
Results
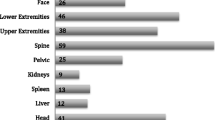
Eighty-four patients were hospitalized for penetrating injuries to the thorax and abdomen. The mean age was 10.3 ± 3.79 years. Patient injuries comprised 26 gunshots injuries and 58 stabbing injuries. Thirty-one patients were wounded in the thorax, 43 were wounded in the abdomen, and 10 were wounded in both the thorax and abdomen. Thirty-one patients had undergone surgical interventions, while the other 53 were managed conservatively. The mean hospital stay was 4.41 ± 6.84 days.
Conclusions
The incidences of penetrating abdominal and thoracic trauma did not differ significantly. Penetrating injuries may be successfully managed by conservative therapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Trauma is a major cause of childhood mortality, morbidity, and disability [1]. The majority of injuries in children are due to blunt trauma (80–90 %), while the incidence of penetrating trauma is relatively low (10–20 %) [1–3]. However, the risk of mortality from penetrating injuries compared with that from blunt injuries is higher among all ages [4]. The incidence of penetrating trauma has been recently increasing, both among all age groups and among children [5–7]. Penetrating injuries in children are associated with a higher mortality and morbidity than those in adults [3]. Because of their thinner body wall and smaller size, children’s internal structures are more susceptible to serious injury [3]. Penetrating abdominal injury is relatively more frequent than penetrating thoracic injury and constitutes 3–6 % of all abdominal injuries [8]. However, the mortality of penetrating thoracic trauma is higher than that of abdominal trauma [1]. The incidence of penetrating thoracic injury is unknown.
Penetrating injury is defined as physical trauma to the skin and tissues with a foreign object such as a gun, knife, or other sharp object by mechanical penetration [3, 5, 8, 9]. The intensity of the penetrating trauma is proportional to the kinetic energy of the object entering the body [9]. Tissue injury is produced by the mechanical force of stab injuries by low pressure applied to a small bodily contact surface. Therefore, the low energy of this pressure does not usually cause trauma to the tissues surrounding the primary site of injury. On the other hand, the pressure is high in gunshot injuries, causing significant harm to the surrounding tissues [9]. As with the rest of the world, possession of guns and stabbing objects by children is also increasing in Turkey. A lower socioeconomic status, widening of the gap between the rich and poor, limited education, exacerbation by the media, and the increased availability of these objects may be responsible for the increasing number of penetrating trauma cases [5, 7].
The purpose of the present study was to evaluate and compare the outcomes of penetrating injuries of the thorax and abdomen.
Materials and methods
The medical charts evaluated retrospectively were of patients hospitalized between 2006 and 2012 with a diagnosis of penetrating thoracic or abdominal trauma. All patients with a penetrating injury from the clavicles to the pubic symphysis were included in the study. Eighty-four patients met the criteria. The study group was further divided into two subgroups comprising patients with either thoracic or abdominal injuries. Demographics, wound characteristics, objects causing the injury, length of hospital stay, management, and clinical results were analyzed.
Data on physical examination findings, blood tests results, and/or radiologic study results during the initial management were obtained. The hepatic transaminase levels were evaluated to predict the presence of liver injury. Hemogram results were studied to determine occult blood loss. Posterior–anterior and lateral X-rays of both the thorax and abdomen were obtained to detect perforation, pneumothorax, and additional visceral injury. When tissue injury was suspected, computed tomography (CT) of the thorax and ultrasonography (US) of the abdomen were performed to detect further injury. If patients had an open wound, antibiotics and tetanus, prophylaxis were administered during the initial management. If patients had skin defects without visceral injury, the defects were repaired. If the patient was considered to be hemodynamically unstable and/or hollow viscus perforation was detected or suspected, surgical intervention was initiated. In patients with penetrating trauma to the abdomen, surgical intervention was initiated if signs of peritonitis or evisceration through the abdominal defect were present. Tube thoracostomy was performed if the patient had pneumothorax or hemothorax that caused or could cause respiratory distress. Open thoracotomy was reserved for ongoing bleeding and removal of foreign objects.
The criteria were being nonoperative treatment which was on physical examination and radiologic studies. Hemogram was studied for determining occult blood loss. All patients underwent X-ray. When there were positive findings on X-ray and physical examination, patients had undergone USG and/or CT for confirmation or exclusion of diagnosis.
All patients were followed up at intensive care unit initially. If the finding of patient was regressed or lost, patients were discharged after 24–48 h close follow-up based on stable serial hemograms and normal X-ray and US results. If the findings increase on X-ray and physical examination, patients underwent appropriate interventions.
Surgical intervention was considered to be unnecessary if visceral injury did not require repair or drainage, no peritoneal penetration was present, or penetration was present without visceral injury. In cases of subcutaneous emphysema, the torso was wrapped circumferentially with an elastic bandage. Patients with pneumothorax or hemothorax without compromising physical findings were closely monitored with serial roentgenograms. Abdominal US examination and plain roentgenograms were utilized for routine follow-up. Occasionally, CT and/or magnetic resonance (MR) imaging were utilized, if needed.
Statistical analyses
Data analysis was performed using the SPSS ver. 11.5 statistical software. Preliminary analyses involved sample frequency tables. Data on injuries were collected, and a descriptive statistical analysis of demographic characteristics (age and gender), circumstances of the injury, clinical presentation, management, and outcomes was performed. The data were expressed as mean ± SD with a 95 % confidence interval. Data were analyzed using the t test, Chi square test. Probability (P) values of <0.05 were considered to indicate statistical significance.
Results
Data from 84 patients were gathered and analyzed in the present study (Table 1).
Age and gender
The majority of the patients were male (86 % male, 14 % female), who were affected sixfold more frequently than females. The mean age of all patients was 10.30 ± 3.79 (1–16) years. The mean ages of the groups were as follows: 9.77 ± 4.20 (1–16) years for patients with thoracic injury, 10.38 ± 3.71 (3–16) years for patients with abdominal injury, and 12 ± 2.26 (9–15) years for patients with both abdominal and thoracic injuries. There were no statistically significant differences between children with thoracic and abdominal injuries in terms of age or gender (P > 0.05). The majority (67.9 %) of patients were accidentally injured. Except for one patient, all other gunshot injuries were accidental; however, stabbing injuries by knife were accidental in 5 of the 26 patients who were injured.
Cause of injury
In 11 of the 31 patients with thorax injuries, the trauma was caused by gunshots, while the trauma in the remaining 20 patients was caused by stabbing (11 knife injuries, 5 penetrating sharp device injuries, and 4 cases of falling on a sharp object). The penetrating thoracic injuries were accidental in (n = 24) majority of the patients. With the exception of seven patients, all thoracic injuries were located in the anterior thoracic wall. Nine patients underwent surgery for thoracic injuries. Six of these underwent tube thoracostomy for hemothorax and/or pneumothorax. The remaining three patients underwent open thoracotomy; two underwent thoracotomy for ongoing bleeding, while one patient underwent an operation for removal of the foreign object. Of the 22 patients with thoracic injuries who underwent no surgical procedures, three underwent application of a compressing circumferential elastic bandage for subcutaneous emphysema. No intervention was required in 11 patients with minimal hemothorax or pneumothorax and/or rib fracture. The remaining eight patients had no abnormal findings on imaging studies despite the presence of penetrating trauma. Complications among patients with thoracic injuries included hemothorax, pneumothorax, rib fracture, vertebral fracture, spinal cord injury. One patient with thoracic injury due to a gunshot wound underwent tube thoracostomy for pneumothorax and hemothorax followed by immediate neurosurgery for paraplegia due to vertebral fracture. This patient had a diaphragmatic rupture found on surgical exploration during the late period.
In 12 of the 43 patients with abdominal injuries, the trauma was caused by gunshots, while the trauma in the remaining 31 patients was caused by stabbing (15 knife injuries, five penetrating sharp device injuries, and 11 cases of falling on a sharp object). The penetrating abdominal injuries were accidental in (n = 32) majority of the patients. There were no statistically significant differences between thoracic and abdominal injury in terms of the cause of the event. All abdominal injuries were located in the anterior abdominal wall. Eighteen patients underwent surgical intervention for abdominal injury. There were detected intestinal perforation in six patients, a gallbladder perforation, and hemobilia in one patient. One patient had liver injury and bleeding due to the presence of gunshot shell fragments. The other 11 patients had no abnormal findings on diagnostic laparotomy. The remaining 25 patients were managed conservatively. Additional problems among patients with abdominal injuries included intestinal perforation, gall bladder perforation, hemobilia, liver injury, and abdominal evisceration.
Among the ten patients who were injured in both the thorax and abdomen, seven were due to gunshots and three were due to falling on a sharp object. Ten patients were injured in both the thorax and abdomen, six were wounded in the anterior wall of the body, and the remaining four were wounded in the back (Table 2). Five patients among those who were injured in both the thorax and abdomen underwent surgical intervention. Three of these patients underwent tube thoracostomy for hemopnuemothorax. The remaining two patients underwent laparotomy; one had a diaphragmatic rupture on surgical exploration, and the other underwent diagnostic laparotomy with no abnormal findings (Table 2).
Radiologic studies on admission
All patients underwent conventional X-ray imaging and hemogram measurement on admission. CT imaging results were obtained from 64 % of patients among the whole study group, 65 % of patients with thoracic injuries, 62 % of patients with abdominal injuries, and 70 % of patients with both abdominal and thoracic injuries. US imaging results were obtained from 54 % of patients in the whole study group, 35 % of patients with thoracic injuries, 55 % of patients with abdominal injuries, and 50 % of patients with both abdominal and thoracic injuries (Table 2).
Hospitalization and outcomes
The mean hospital stay was 4.41 ± 6.84 (1–60) days for the whole study group, 3.70 ± 3.21 (1–14) days for patients with thoracic injuries, 5.11 ± 8.99 (1–60) days for patients with abdominal injuries, and 3.60 ± 3.92 (1–14) days for patients with both thoracic and abdominal injuries. When surgical and conservative management were compared, patients who were managed conservatively had a mean 2.58 ± 2.34 days of hospitalization, and patients who were managed surgically had a mean 7.54 ± 10.20 days of hospitalization. The difference was statistically significant (P = 0.000). The operative group had a longer-duration hospital stay than the nonoperative group.
Complications
There were no encountered secondary complications and death in the present study.
Discussion
Penetrating thoracic and abdominal injuries are rare, and their exact incidence is unknown. The incidence of these injuries is related to the rate of violence in the society [1]. Nevertheless, due to alterations in the social structure, the incidence of these events has been recently increasing [7]. Regardless of age, penetrating trauma may occur among all ages of children [5]. It is less prevalent in preschool ages and usually happens accidentally (e.g., contact with sharp broken glass or metal objects). Penetrating trauma is usually seen among adolescents and teenagers and is usually intentional (e.g., knife or gunshot wounds) [1, 8–10]. Therefore, adolescent males living in low socioeconomic environments are at particular risk of penetrating injuries [7]. In the present study, the results of age distribution were in accordance with those in the English-language literature. Most of the injuries were accidental. The incidence of penetrating trauma in males was found to be sixfold greater than that in females. This finding suggests that males of this age group are more prone to involvement in violence and hazardous acts compared with their female peers.
In previous studies, penetrating trauma to the thorax and abdomen was a more frequent cause of mortality and morbidity in children than in adults. This may be attributed to body structure [1, 2]. In addition, penetrating injuries to the thorax are reportedly associated with a higher mortality than are penetrating abdominal injuries [1, 4]. In the present study, there was no mortality; however, there were various severe visceral injuries. The low mortality in the present study may be explained by the nature of the local social and geographic conditions; patients with serious injuries may die before reaching a medical care facility due to a number of factors, such as distance between the hospital and the town and limited resources in this developing rural province. Thus, patients with mortal injuries may be lost at the scene of the event or during transportation to the hospital. This was a limitation of our study, and thus it does not reflect the true mortality rates of penetrating thoracic and abdominal trauma. To overcome this limitation, the records of the emergency departments of hospitals and the records of emergency call services may be included in future studies.
Penetrating trauma to the abdomen and thorax are frequently minor injuries. Thoracic injuries involve less morbidity and mortality. Therefore, most penetrating abdominal and thoracic injuries can be managed successfully by conservative measures [7, 11]. The morbidity rate of abdominal injuries in the present study was greater than that of thoracic injuries, and the hospital stay was longer. The most common cause of morbidity in patients with penetrating thoracic injuries is atelectasis [12]. In the present study, pneumothorax was the most common cause of morbidity. Rib fractures are less common in adults because of the comparatively higher elasticity of the chest wall than in children [12]. In the present study, rib fractures were diagnosed in five patients, and diaphragmatic rupture was diagnosed during late surgical exploration in one patient. Diaphragm rupture is usually diagnosed in the late phase unless the patient has undergone surgical exploration [13]. It may be the consequence of the selective group of patients who arrived in the hospital, only.
Advances in diagnostic tools have lowered the negative exploration rates [11]. The most commonly utilized assay is a plain roentgenogram. US, CT, and MR imaging are the other preferred imaging modalities. CT is very helpful in deciding between surgical and conservative management [13, 14]. US is most commonly preferred for ease of serial monitoring and detecting additional visceral injury. When these measures do not suffice to rule out visceral injury, minimally invasive surgical procedures may be utilized. In the present study, laparoscopy was not used for diagnostic purposes in abdominal trauma patients, because we do not have appropriate tools of laparoscopy. In the present study, all patients underwent physical examination and X-ray at the time of the initial admission. When there were positive findings on X-ray and physical examination, the patients also underwent CT and/or US examinations.
There is no standard management of patients with penetrating trauma. The purpose of management is to treat patients while avoiding unnecessary surgical interventions. Conventional surgical teaching dictates urgent surgical exploration if the hemodynamic parameters are unstable in cases of penetrating trauma. Until recently, the standard management of penetrating trauma was immediate surgical exploration. When this approach was found to be associated with higher negative exploration rates, higher morbidity, and longer hospital stays, conservative measures gained popularity to prevent these complications [15, 16]. Unnecessary surgery for trauma is reportedly associated with complication rates of 2.5–41 % [14]. After the first report by Shaftan in 1960 showing the increased morbidity of urgent exploration for penetrating trauma, urgent surgical exploration rates dropped, and negative exploration rates more recently dropped to as low as 10 % [15, 16]. Previous reports support the notion that patients with penetrating trauma can be managed conservatively whether or not visceral injury is present because one-third of these injuries are non-significant and do not require surgical intervention [15, 17]. If surgery is planned, laparoscopy may be considered first for exploration [14]. Laparoscopic exploration may reduce the morbidity associated with open surgery [18]. Patients with abdominal injuries underwent surgery more often than did patients with thoracic injuries in our series, possibly due to the protective effect of the bony structures of the thoracic wall. Previous studies have reported that penetrating thoracic injuries usually require surgical intervention [1]. In our experience, patients with hemodynamically stable hemothorax, pneumothorax, and subcutaneous emphysema that did not cause respiratory distress were safely managed with conservative measures. In the present study, the negative laparotomy rate was much higher than anticipated. This higher rate could be attributed to the insufficient resources for close monitoring of patients in our setting. In the present study, explorations in the early years of the study were more often negative than those in the later years, at which time the negative exploration rate dropped to 13.6 %.
Several limitations should be considered when evaluating the results of this study. The data collected were from those hospitalized at pediatric surgery ward with related penetrating injuries. Also, the study was retrospective, only the information in the records was available and not all data could be evaluated. Therefore, we had no data regarding the mechanism and outcomes of all penetrating injuries. We did not have equipment of laparoscopy; therefore, we did not have experience with laparoscopy in the present study. The sample size of the present study was small, therefore, it may not be representative for general statement.
In conclusion, in the present study, abdominal injuries are more frequent than thoracic injuries, and negative exploration rates are higher in abdominal injuries. Conservative management of penetrating thoracic and abdominal injuries is considered to be safe. Development of management strategies should be accompanied by preventive measures such as social projects and educational programs to prevent violence and its consequences.
References
Wessen DE, Stylianos S, Pearl RH (2006) Thoracic injuries, abdominal trauma. In: Grosfeld JL, O’neill JA (eds) Pediatric surgery, 6th edn. Mosby Inc, Philadelpia, pp 275–316
Cotton BA, Nance ML (2004) Penetrating trauma in children. Semin Pediatr Surg 13(2):87–97
Sandler G, Leishman S, Branson H et al (2010) Body wall thickness in adults and children–relevance to penetrating trauma. Injury 41(5):506–509
Ottochian M, Salim A, DuBose J et al (2009) Does age matter? The relationship between age and mortality in penetrating trauma. Injury 40(4):354–357
Schecter SC, Betts J, Schecter WP et al (2012) Pediatric penetrating trauma: the epidemic continues. J Trauma Acute Care Surg 73(3):721–725
Adesanya AA, da Rocha-Afodu JT, Ekanem EE et al (2000) Factors affecting mortality and morbidity in patients with abdominal gunshot wounds. Injury 31(6):397–404
Melling L, Lansdale N, Mullassery D et al (2012) Penetrating assaults in children: often non-fatal near-miss events with opportunities for prevention in the UK. Injury 43(12):2088–2093
Adorisio O, Elia A, Pinzauti E et al (2008) The importance of a multidisciplinary approach in a child with major abdominal penetrating trauma. Pediatr Emerg Care 24(1):34–36
Moore K (2012) The knife and gun club just adjourned: managing penetrating injuries in the emergency department. J Emerg Nurs 38(1):102–103
Holland AJ, Kirby R, Browne GJ et al (2002) Penetrating injuries in children: is there a message? J Paediatr Child Health 38(5):487–491
Morrison JJ, Clasper JC, Gibb I et al (2011) Management of penetrating abdominal trauma in the conflict environment: the role of computed tomography scanning. World J Surg 35(1):27–33
Cobanoğlu U, Yalçinkaya I (2010) Thoracic injuries. Ulus Travma Acil Cerrahi Derg 16(1):77–83
Madiba TE, Thomson SR, Mdlalose N (2001) Penetrating chest injuries in the firearm era. Injury 32(1):13–16
Como JJ, Bokhari F, Chiu WC et al (2010) Practice management guidelines for selective nonoperative management of penetrating abdominal trauma. J Trauma 68(3):721–733
Salim A, Velmahos GC (2002) When to operate on abdominal gunshot wounds. Scand J Surg 91(1):62–66
Shaftan GW (1960) Indications for operation in abdominal trauma. Am J Surg 99:657–664
Cigdem MK, Onen A, Siga M et al (2009) Selective nonoperative management of penetrating abdominal injuries in children. J Trauma 67(6):1284–1286
Gaines BA, Rutkoski JD (2010) The role of laparoscopy in pediatric trauma. Semin Pediatr Surg 19(4):300–303
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boleken, M.E., Cevik, M., Yagiz, B. et al. The characteristics and outcomes of penetrating thoracic and abdominal trauma among children. Pediatr Surg Int 29, 795–800 (2013). https://doi.org/10.1007/s00383-013-3339-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-013-3339-z