
Abstract
Purpose
We report a multicenter experience using double dartos flap to protect the neourethra in TIP urethroplasty for distal and midpenile hypospadias.
Methods
A total of 394 patients underwent tubularized incised plate urethroplasty for primary distal and midpenile hypospadias using double dartos flap protection by ten pediatric surgeons and urologists at five different institutions.
Results
Tubularized incised plate urethroplasty protected by a double dartos flap was simple to perform and flaps were easy to obtain. Complications occurred in 23 patients (5.83%): fistulas 1.01% (4 cases), stenosis 0.25% (1 case), mild stenosis 2.53% (10 cases), dehiscence of ventral cutis 0.50% (2 cases) and penile torsion 1.26% (5 cases). All fistulae had a spontaneous resolution.
Conclusion
Double dartos flap to protect tubularized incised plate urethroplasty is safe with a low complication rate. The neourethra is covered entirely with a double layer of vascularized tissue and the double coverage appears a good choice for preventing urethrocutaneous fistula formation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since it was first described by Snodgrass [1] in 1994, tubularized incised plate (TIP) urethroplasty had a worldwide diffusion. The use of a dartos flap covering the neourethra as a barrier to prevent fistula formation was originally described in 1994 by Snodgrass [1] and Retik et al. [2], who obtained the flap from a transverse island of dorsal subcutaneous tissue interposed between the neourethra and the skin. However, urethrocutaneous fistulas represent the most frequent complication [3, 4] and the reported incidence is as high as 2–16% [4–6].
The first author to publish a double dartos flap (DDF) to protect the neourethra was Kamal in 2005 [7], affirming that DDF provides more protection against fistula development rather than a single flap. Since this date, other authors have reported their experience in covering the neourethra with a double layer of dartos tissue in TIP urethroplasty, with very similar techniques and excellent results [8–12].
This multicenter study reports the results of five centers and ten surgeons performing the DDF protection in TIP urethroplasty for distal and midpenile hypospadias.
Materials and methods
From March 2002 to June 2010, ten pediatric surgeons and urologists at five different institutions in Europe and Middle East performed primary TIP urethroplasty protected with DDF on 394 patients affected by distal and midpenile hypospadias. The age of patients ranged from 6 months to 17 years (mean 54 months).
Of these patients, 17 had coronal, 180 sub-coronal, 126 distal penile and 71 midshaft hypospadias. Ventral curvature was present in 42 patients. No patients had previously undergone urethroplasty.
Data were collected via a survey from all authors who had previously published their results [7–10, 13]. Once a TIP urethroplasty is obtained according to Snodgrass, the authors protect the neourethra with a DDF: a vascularized dartos flap is dissected from the dorsal preputial and shaft skin (Fig. 1a). Dissection of the flap from the shaft skin did not go beyond 1–2 cm distal to the root of the penis, depending on the size of the penis. In case of distal hypospadias, dartos was mostly mobilized only from the portion of the preputial tissue that was to be removed. This preserves as much blood supply to the flap as possible. The flap was incised vertically in the midline to form two equal well-vascularized rectangular flaps and the vascular pedicles were preserved (Fig. 1b). Both flaps were then ventrally rotated and transposed over the neourethra, one to the right and the other to the left with symmetric rotation. The left flap was rotated laterally from the left side to cover the neourethra (Figs. 2a, 3) and it was stitched to the periurethral tissue (Figs. 2b, 4). The right flap was then rotated laterally from the right side to overlap the left flap and sutured taking care that the sutures of the two flaps did not overlap (Fig. 5a, b). In the presence of curvature (42 patients), surgical correction was done: in 37 cases by degloving the penis and by dissection of the tissue around the urethral plate; in the other 4 patients, a Nesbitt technique was performed; and in 1 patient, Baskin placation was done.

a The flap is prepared from the foreskin, b a longitudinal incision is effected along the flap to create two hemi-flaps

a The first flap is placed to cover the neourethra in its entirety, b the second flap is superimposed over the first flap

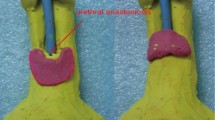
Schematic drawing to show how the first flap is placed to cover the neourethra

Schematic drawing to show the ventral transposition of the second flap

a A double dartos flap is created on the neourethra. The sutures do not overlap, b the result at the end of the surgical procedure
A urethral stent or an open or closed temporary urinary diversion according to the urethra’s diameter and the patient’s age was left in place from 7 to 10 days in all patients. All authors used a compressive penile dressing, which was removed from the second to fifth day postoperatively, and antibiotic prophylaxis was routinely used during the postoperative period.
The details are shown in Table 1.
The authors report their results analyzing all the complications that occurred: fistulas, dehiscence of glans and ventral cutis, penile torsion, stenosis and mild stenosis. The difference between stenosis and mild stenosis has been defined by the authors: at the first control after catheter removal, if dilatation of the neomeatus was possible with the same catheter size as that used during surgery, stenosis was defined as “mild”; it was defined as stenosis when a smaller catheter size was necessary.
Results
Postoperative follow-up ranged from 6 to 106 months. In 371 patients (94.17%), good cosmetic results were obtained without any complication.
Complications occurred in 23 patients (5.83%): fistulas 1.01% (4 cases), stenosis 0.25% (1 patients), mild stenosis 2.53% (10 cases), dehiscence of ventral cutis 0.50% (2 cases) and penile torsion 1.26% (5 cases).
All fistulae occurred at the level of the native hypospadic meatus and were very narrow with a leak of only a few drops of urine through micturition. All fistulae were completely healed and closed spontaneously 2–5 weeks after catheter removal. None was associated with meatal stenosis.
A unique stenosis occurred, and it was corrected by urethral dilation of the external meatus by 6 Fr feeding catheter at an interval of up to 2 months. The ten cases of mild stenosis were managed by simple daily meatal dilation for 3 months in seven patients; in three patients, it was treated and resolved with dilatations at home for 15–20 days using a self-lubricating catheter for 15 min twice daily. None of the stenotic or mild stenotic cases required meatotomy. In two cases, dehiscence limited to the ventral skin healed spontaneously with epithelization.
Penile torsion occurred in five cases: in two cases, at 5° to the right; in two other cases at 5° to the left; and in one patient at 10° to the right. Penile torsion degrees were estimated to be very low and so nothing was applied.
Discussion
In the past decade, TIP urethroplasty has rapidly gained popularity for correcting hypospadias because such repair is easily performed and can have good cosmetic results, with a vertically oriented meatus [14–16]. However, urethrocutaneous fistulas are still reported as the most frequent complication [3, 4]. One of the most important factors to avoid the occurrence of fistulas is the application of a protective intermediate layer between the neourethra and the skin [17]. In fact, flapless urethroplasties have a higher risk of fistula development: a 13 and 15% incidence of fistulas was reported in two studies after TIP urethroplasty without a dartos flap [18, 19].
Other protective intermediate layers such as external spermatic fascia flaps, tunica vaginalis and scrotal and ventral dartos flaps have been described as alternatives to the dorsal ones, especially in circumcised boys or those undergoing reoperation [17, 20–22].
When TIP urethroplasty was originally described, a transverse island of dorsal subcutaneous tissue was used as a flap [1]. Later on, Snodgrass transposed it ventrally in a buttonhole fashion to cover the neourethra [23]. Although this technique has achieved a 100% fistula-free outcome with Djordjevic et al. [15, 24], fistula occurrence was as high as 3% for others [25] and not infrequent in various reported studies [3, 26].
It is not clear how urethrocutaneous fistulas develop in the presence of an interposed dartos flap. Moreover, when a single dartos flap is used, a fistula track can develop through the suture line next to the flap edge. The fistulas can find the way through a small perforation due to injury during dissection, focal ischemic injury or infection.
The first author reporting a DDF to protect the neourethra was Kamal in 2005 [7], who reported that covering the neourethra with DDF was superior to single dartos flap to prevent fistula development. Recently, other authors have reported the effectiveness of DDF protection, comparing flapless TIP urethroplasty, and TIP urethroplasty protected by single dartos flap and by DDF [10, 13]. Erol et al. [11] in a prospective randomized study analyze the single versus double dartos interposition flaps in preventing urethrocutaneous fistulas, affirming that double symmetrical dartos flap to protect the neourethra decreases the fistula rate virtually down to 0%. In the case of double dartos flaps, two pedicles are rotated from both sides and fixed across the neourethra. This seals the neourethra from the glans and skin on the front, as well as on both sides, and provides more protection against fistula development. When double dartos flaps are used, a perforation in one flap, which may cause a urethrocutaneous fistula, would be protected by the second layer of the dartos flap.
In this multicentric experience, fistulas occurred only in four cases (1.01%). These fistulas were very narrow, and completely healed and closed spontaneously after few weeks. It is well known that fistulas appear in areas of least resistance of the reconstructed urethra because of an inadequate cicatrization process and/or due to infective processes that are often related to poor blood supply. To preserve as much blood supply as possible to the flap, its dissection from the shaft skin did not go beyond 1–2 cm distal to the root of the penis. We think that the double well-vascularized flap interposed between the neourethra and the skin may add to the spontaneous healing of fistulas in this multicentric experience (100%), because fistulas may have very good blood supply for spontaneous cicatrization from the two interposed layers of dartos tissue.
Meatal stenosis is another complication that may be observed after TIP procedure. Published data indicate the occurrence of metal stenosis to be between 0.7 and 17% after TIP repair [27, 28]. Snodgrass reported that the dorsal midline incision wound healed without cicatricial evidence and did not cause meatal and urethral stenosis [27, 29]. However, tight closing of the distal neourethra could cause a narrow meatus [28]. In our series, we had one patient (0.25%) with stenosis and the other ten cases with mild stenosis (2.53%), with a total stenosis rate of 2.78%, similar to those reported in the literature. In all cases, stenoses were limited to the meatus and were managed by simple meatal dilation.
None of the stenotic or mild stenotic cases required meatotomy
Glans dehiscence in the presence of the dartos flap is a rare complication [23], but Elbakry [19] affirms that the dartos flap should not be used because it hinders tension-free closure of the glans flaps and increases the risk of glans dehiscence. Therefore, the presence of a double dartos layer to protect the neourethra could have a greater risk of glans dehiscence. In the present study, glans dehiscence was not seen. Glans closure was achieved comfortably by the deep dissection of the glans wings, obtaining good mobility for later closure. Nevertheless, dehiscence limited to the ventral skin occurred in two cases of mediopenile hypospadias repair (0.50%) which healed spontaneously with epithelization. Another possible complication after TIP urethroplasty using a single flap carried out with a transverse island of dorsal subcutaneous tissue to protect the neourethra is penile torsion. Yiğiter et al. [13] in a comparative retrospective study report a significant decrease (from 43.5 to 3.8%) of penile torsion in patients submitted to TIP urethroplasty protected by DDF compared to those protected by single dartos flap. In this multicentric experience, penile torsion occurred in five cases (1.26%); the degrees (5° in four cases and 10° in one case) were estimated to be very low and so nothing was applied.
Conclusion
This multicentric experience shows that TIP urethroplasty, entirely protected with a double layer of well-vascularized tissue such as dartos, has a very low complication rate, especially concerning fistula occurrence. Ten surgeons of five different institutions participated in the study with similar results, demonstrating the reliability of the protection with DDF in TIP urethroplasty and indicating that the procedure probably was not significantly affected by the surgeon’s skill. Therefore, this experience suggests that the coverage of neourethra by DDF is a safe procedure with minimal complication rate, and it may be a recommended choice for protecting the neourethra in TIP urethroplasty in distal and midpenile hypospadias.
References
Snodgrass W (1994) Tubularized, incised plate urethroplasty for distal hypospadias. J Urol 151:464–465
Retik AB, Mandell J, Bauer SB et al (1994) Meatal based hypospadias repair with the use of a dorsal subcutaneous flap to prevent urethrocutaneous fistula. J Urol 152:1229–1231
Sozubir S, Snodgrass W (2003) A new algorithm for primary hypospadias repair based on tip urethroplasty. J Pediatr Surg 38:1157–1161
Snodgrass WT (2005) Snodgrass technique for hypospadias repair. BJU Int 95:683–693
Sugarman ID, Trevett J, Malone PS (1999) Tubularization of the incised urethral plate (Snodgrass procedure) for primary hypospadias surgery. BJU Int 83:88–90
Guralnick ML, al-Shammari A, Williot PE et al (2000) Outcome of hypospadias repair using the tubularized, incised plate urethroplasty. Can J Urol 7:986–991
Kamal BA (2005) Double dartos flaps in tubularized incised plate hypospadias repair. Urology 66:1095–1098
Bakan V, Yildiz A (2007) Dorsal double-layer dartos flap for preventing fistulae formation in the Snodgrass technique. Urol Int 78:241–244
Mustafa M, Wadie BS, Abol-Enein H (2008) Standard Snodgrass technique in conjunction with double-layer covering of the neourethra with dorsal dartos flap is the therapy of first choice for hypospadias. Int Urol Nephrol 40:573–576
Appignani A, Prestipino M, Bertozzi M et al (2009) Double-cross flap protection: new technique for coverage of neourethra in hypospadias repair. J Urol 182:1521–1527
Erol A, Kayikci A, Memik O et al (2009) Single vs double dartos interposition flaps in preventing urethrocutaneous fistula after tubularized incised plate urethroplasty in primary distal hypospadias: a prospective randomized study. Urol Int 83:354–358
Abolyosr A (2010) Snodgrass hypospadias repair with onlay overlapping double layered dorsal dartos flap without urethrocutaneous fistula: experience of 156 cases. J Pediatr Urol 6:403–407
Yiğiter M, Yildiz A, Oral A et al (2010) A comparative study to evaluate the effect of double dartos flaps in primary hypospadias repair: no fistula anymore. Int Urol Nephrol 42:985–990
El-Sherbiny MT, Hafez AT, Dawaba MS et al (2004) Comprehensive analysis of tubularized incised-plate urethroplasty in primary and re-operative hypospadias. BJU Int 93:1057–1061
Djordjevic ML, Perovic SV, Slavkovic Z et al (2006) Longitudinal dorsal dartos flap for prevention of fistula after a Snodgrass hypospadias procedure. Eur Urol 50:53–57
Baccala AA Jr, Ross J, Detore N et al (2005) Modified tubularized incised plate urethroplasty (Snodgrass) procedure for hypospadias repair. Urology 66:1305–1306
Hayashi Y, Kojima Y, Kurokawa S et al (2005) Scrotal dartos flap for the prevention of the urethrocutaneous fistula on hypospadias urethroplasty. Int J Urol 12:280–283
Holland AJA, Smith GHH (2000) Effect of the depth and width of the urethral plate on tubularized incised plate urethroplasty. J Urol 164:489–491
Elbakry A (1999) Tubularized-incised urethral plate urethroplasty: is regular dilatation necessary for success? BJU Int 84:683–688
Chatterjee US, Mandal MK, Basu S et al (2004) Comparative study of dartos fascia and tunica vaginalis pedicle wrap for the tubularized incised plate in primary hypospadias repair. BJU Int 94:1102–1104
Soygur T, Arikan N, Zumrutbas AE et al (2005) Snodgrass hypospadias repair with ventral based dartos flap in combination with mucosal collars. Eur Urol 47:879–884
Yamataka A, Ando K, Lane GJ et al (1998) Pedicled external spermatic fascia flap for urethroplasty in hypospadias and closure of urethrocutaneous fistula. J Pediatr Surg 33:1788–1789
Snodgrass WT (2002) Tubularized incised plate (TIP) hypospadias repair. Urol Clin North Am 29:285–290
Djordjevic ML, Perovic SV, Vukadinovic VM (2005) Dorsal dartos flap for preventing fistula in the Snodgrass hypospadias repair. BJU Int 95:1303–1309
Baskin LS, Duckett JW (1994) Dorsal tunica albuginea plication for hypospadias curvature. J Urol 151:1668–1671
Snodgrass W, Yucel S (2007) Tubularized incised plate for mid shaft and proximal hypospadias repair. J Urol 177:698–702
Lorenzo AJ, Snodgrass WT (2002) Regular dilatation is unnecessary after tubularized incised-plate hypospadias repair. BJU Int 89:94–97
Stehr M, Lehner M, Schuster T et al (2005) Tubularized incised plate (TIP) urethroplasty (Snodgrass) in primary hypospadias repair. Eur J Pediatr Surg 15:420–424
Snodgrass W (1999) Does tubularized incised plate hypospadias repair create neourethral strictures? J Urol 162:1159–1161
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bertozzi, M., Yıldız, A., Kamal, B. et al. Multicentric experience on double dartos flap protection in tubularized incised plate urethroplasty for distal and midpenile hypospadias. Pediatr Surg Int 27, 1331–1336 (2011). https://doi.org/10.1007/s00383-011-2978-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-011-2978-1