
Abstract
Introduction
Anorectal malformations represent a continuing challenge for the paediatric surgeon. Faecal and urinary incontinence can occur even with an excellent anatomic repair. We undertook a prospective evaluation of comorbidity and psychosocial needs in children and adolescents with anorectal malformation to test the hypothesis whether psychosocial workup in concert with an improved continence situation would lead to a better functional outcome in patients suffering from defecating disorders. Treatment of defecating disorder was based on differentiation between overflow pseudo-incontinence and true faecal incontinence.
Materials and methods
Patients who presented with soiling regardless of the type of anomaly were included in the study: 44 patients were investigated, 14 patients did not meet the criteria of the study, 30 patients aged 4–18 were evaluated. The surgical diagnostic program comprised a careful clinical history, physical examination, exact classification of the malformation, evaluation for associated defects, stool protocol.
Results
Patients were grouped in two different management programs according to their continence situation. Patients with pseudo-incontinence were treated with enemas, diet, anal hygiene, behavioural therapy and physiotherapy. Patients with true faecal incontinence were included in a bowel management program: 28 patients were free of symptoms of soiling after 3 days of hospital treatment and remained free of symptoms 6 months and 1 year later at re-evaluation. Two patients did not follow the therapeutic regime and therefore did not show an improved condition concerning soiling in the long run.
Conclusion
Differentiating between overflow pseudo-incontinence and true faecal incontinence is the basis of an effective treatment of defecating disorders. All patients born with anorectal malformation can be kept clean of stool if they are subjected to an adequate treatment. A multidisciplinary approach is a valuable supplement to standard therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anorectal malformations represent a continuing challenge for the paediatric surgeon. The main concerns for the surgeon in correcting these anomalies are bowel control, urinary control, and sexual function. With correct diagnosis, management of associated anomalies and adequate surgical repair, patients have the chance for a good functional outcome. But still defecating disorders can occur even with an excellent anatomic repair, mainly due to associated problems such as a poorly developed sacrum, deficient nerve supply, and spinal cord anomalies. In these patients, an effective management program, including enema, special diet, behavioural therapy, physiotherapy, anal hygiene or bowel management can improve the quality of life.
We undertook a prospective evaluation of defecating disorders and psychosocial needs in children and adolescents with anorectal malformation. Treatment of defecating disorder was based on differentiation between overflow pseudo-incontinence and true faecal incontinence. A multidisciplinary approach involving physiotherapy and behavioural therapy is a valuable supplement to standard medical treatment.
Materials and methods
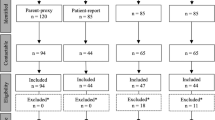
Patients who presented with soiling regardless of the type of anomaly were included in the study; 44 patients were investigated. Nine patients did not participate in the psychological screening and five patients were excluded due to age. Thirty patients aged 4–17 were evaluated: 23 males and 7 females with ARM were investigated. Fifteen patients were 10 years and older. The patients were classified according to fistula localisation [1]. The continence situation was classified referring to the Krickenbeck Conference [2]. The surgical diagnostic program comprised a careful clinical history, physical examination, exact classification of the malformation, evaluation for associated defects and a detailed stool protocol for 2 weeks. Patients and parents were asked to prospectively complete a 2-week defecation protocol detailing the number, amount, consistency and timing of daily bowel movements and soiling accidents, and the use of medication during each assessment. Furthermore, the need to push during evacuation of stool was documented. If involuntary loss of stool, so called “accidents” occurred, patients were asked to detail whether soiling was frequent during active movement such as sport or rather in passive situations such as resting or sleeping. All parameters were evaluated and patients were grouped in two different management programs according to their continence situation (Table 1).
Management program 1
Management program 1 was intended for patients with intact sphincter function and symptoms of overflow pseudo-incontinence. All patients received oral polyethylene glycol for intestinal purgation to evacuate stool impaction. Then an individual program was adjusted with oral laxatives (lactulosis, magnesium oxide) and if necessary sorbit enemas. If we found a dilated rectum and distended colon, the patient received a hydrophobic diet. If the rectum was found to be of regular size, a hydrophilic diet was initiated [3]. All patients were told to meticulously clean the anal region with water after each defecation. Behavioural therapy using child-motivating techniques and teaching the parents to reinforce the child’s efforts was initiated. Patients were told to try to defecate after meals even without feeling of urge. A paediatric physiotherapist assisted in teaching the child how to build up pressure in the right direction and to tense and relax the muscles of the pelvic floor selectively and to combine both to defecate in the correct way. The child had to learn to use the lower part of its body, to exercises voluntary muscle structures and increase motility and sensitivity of the anorectal region. All patients had to continue with the detailed stool protocol to verify therapeutic effects.
Management program 2
Management program 2 was planned for patients with true faecal incontinence. These patients also received oral polyethylene glycol to evacuate stool impaction. Then patients were started on a bowel management program [4]. The bowel management was initiated with the help of hydrosonography to evaluate bowel motility [5]. Colonic irrigation was adjusted individually so that one bowel management procedure did not last longer than 45 min and kept the patient clean for 48 h. Hygiene of the anal region, physiotherapy and a stool protocol were recommended as in group 1.
In parallel all patients received a complex psychiatric workup for details of this investigation see part two of this article.
All patients were followed up at 6 months and 1 year
Results
The results for the classification according to fistula localisation and defecating disorder are shown in Table 2.
The results for the continence score according to the Krickenbeck Conference are displayed in Table 3. All patients interviewed had somatic symptoms. No patient was assigned to group 1 of the continence score.
All patients in groups 2 and 3 met the criteria for the most severe grade of defecating disorder. They were found in all age groups. One patient could not be classed with the continence score.
Ten patients were grouped in management program 1. These ten patients with grade 3 constipation were also soiling prior to therapy. Twenty patients received management program 2; 30 patients were free of symptoms of soiling after 3 days of hospital treatment. All patients were investigated regularly every 4 weeks for 3 months and the therapeutic regime adjusted if necessary. All 10 patients of management program 1 improved their results for the continence score from group 3, grade 3 to group 1 (Table 3). Eighteen patients of management program 2 improved their continence score from group 2, grade 3 to grade 1. Sixteen patients showed no soiling at all. At follow-up 6 months and 1 year later the therapeutic effect had improved in two patients and remained stable in 26 (Table 4). Two patients did not follow the therapeutic regime and did not show an improved condition concerning soiling.
Discussion
Many patients who undergo repair of an anorectal malformation have some degree of a defecating disorder [6–10]. Faecal continence depends on three main factors: sphincters, sensation and motility. These factors are the major components of the continence organ. Involuntary muscles are important for closure of the anal canal and peristalsis such as the motility of the rectosigmoid. Voluntary muscle structures are used for brief periods prior to defecation when a person feels that it is necessary to use them. For this sensation and for proprioception of a distended rectum, intact sensory mechanism is crucial. Furthermore, the anal skin is specialized to differentiate wind from evacuation of stool [11]. Many patients with anorectal malformation have hypodevelopment of the functional structures of the continence organ with deficient nerve supply [12, 13]. As a consequence of surgery and defecating disorder, the anal skin is often compromised by scaring and chronic dermatitis from soiling.
A multidisciplinary treatment of defecating problems has been promoted before. Children appear to benefit from multidisciplinary behavioural treatment aimed at improving continence and constipation [14].
Our patients belonged to a preselected population because they presented with symptoms of soiling in a specialized consultancy and did not come for routine investigation. Therefore, we were confronted with a severely affected population. According to the literature, treatment is more successful when patients have good continence are clean or only smearing [14].
In children with ARM, the complex process of defecating is disrupted because of the congenital anomaly, surgical procedures, and behavioural factors. In multidisciplinary behavioural treatment, the expertise of three different professions is combined to treat incontinence and constipation to restore the process of defecation as much as possible.
Several randomized, controlled studies concerning the treatment of functional constipation or incontinence in otherwise healthy children show the need and success of behaviour modification combined with laxative treatment [14–18]. Cox [17] also stresses the need for teaching children how to strain adequately without paradoxical constriction of the external anal sphincter, and proved that this can be learned by direct monitoring and demonstration. Both management programs as studied here were based on differentiation between overflow pseudo-incontinence and true faecal incontinence. They combined different aspects of treatment: laxative treatment or bowel management by the paediatric surgeon is combined with behavioural modification by the psychologist, while the paediatric physiotherapist teaches an adequate straining technique. We believe that meticulous anal hygiene had an additive beneficial effect as patients experienced a feeling of cleanliness. The combination of a variety of accompanying measures might explain the relatively high success rate found in both groups of patients.
Baseline scores of young children appear to be significantly poorer than those of older children on most outcome variables, which is consistent with other research [19]. However, we did not find an effect of age on treatment which is consistent with other work groups [14, 18]. Therefore, a multidisciplinary approach seems to be as suitable and effective for younger children as well as for older children.
Effect of treatment in children with constipation and intact sphincter function was expected to be better than that of children with incontinence because of their somatic differences. In our patients the outcome concerning soiling was better in management group 2 which comprised patients with functional incontinence. This effect might be due to the fact that these patients received bowel management to serve as basis of therapy. In contrast to other work groups [18], we did not expect patients with compromised continence organ to benefit from behaviour modification alone.
The positive results of the management programs remained stable in all our patients who continued treatment after a mean follow-up period of 12 months.
Considering the continence score (Table 4), 93% of all patients in this study can be considered to be improved at 12 months after treatment.
Therefore, we can conclude that differentiating between overflow pseudo-incontinence and true faecal incontinence is a helpful instrument to implement an effective treatment of the symptom soiling. A multidisciplinary approach is an important and valuable supplement to the standard medical treatment of children with congenital ARM suffering from chronic defecating problems.
Conclusion
Patients born with anorectal malformation can be kept clean of stool if they are subjected to an adequate treatment.
References
Pena A (1995) Anorectal malformations. Semin Pediatr Surg 4(1):35–47
Holschneider A, Hutson J, Pena A, Bekhit E, Georgeson K, Iwai N et al (2005) Preliminary report on the international conference for the development of standards for the treatment of anorectal malformations. J Pediatr Surg 40:1521–1526
Kasper H (1985) Ernährungsmedizin und Diätetik. Urban and Schwarzenberg, Munich
Pena A, Guardino K, Tovilla JM et al (1998) Bowel management for fecal incontinence in patients with anorectal malformations. J Pediatr Surg 33:133–137
Koltai JL, Pistor G (1985) Anorektale Inkontinenz. Urban and Schwarzenberg, Munich
Levitt M, Pena A (2005) Outcomes from the correction of anorectal malformations. Curr Opin Pediatr 17(3):394–401
Rintala R, Mildh L, Lindahl H (1992) Fecal continence and quality of life in adult patients with an operated low anorectal malformation. J Pediatr Surg 27(7):902–905
Rintala R, Mildh L, Lindahl H (1994) Fecal continence and quality of life in adult patients with an operated high or intermediate anorectal malformation. J Pediatr Surg 29(6):770–780
Holschneider A (1983) Treatment and functional results of anorectal continence in children with imperforate anus. Acta Chir Belg 82(3):191–204
Holschneider A (1990) Diagnosis and primary surgical therapy of anorectal abnormalities with regard to postoperative incontinence. Zentralbl Chir 115(22):1409–1422
Stelzner F (2001) Anatomie und Entwicklungsgeschichte des anorektalen Kontinenzorgans. Chir Gastroenterol 17:194–201
Holschneider A, Koebke J, Meier-Ruge W, Land N, Jesch NK (2001) Pathophysiology of chronic constipation in anorectal malformations. Eur J Pediatr Surg 11:305–310
Pena A, Levitt MA (2002) Colonic inertia disorders. Curr Probl Surg 39:666–730
van Kuyk EM, Wissink-Essink M, Brugman-Boezeman AT, Oerlemans HM, Nijhuis-van der Sanden MW, Severijnen RS et al (2001) Multidisciplinary behavioral treatment of defecation problems: a controlled study in children with anorectal malformations. J Pediatr Surg 36:1350–1356
van-Kuyk EM, Brugman-Boezeman AT, Wissink-Essink M et al (2000) A biopsychosocial treatment of defecation problems in children with anal atresia: a retrospective study. Pediatr Surg Int 16:317–321
Van-der-Plas RN, Benninga MA, Redekop WK et al (1996) Randomised trial of biofeedback training for encopresis. Arch Dis Child 75:367–374
Cox DJ, Sutphen J, Borowitz S et al (1998) Contribution of behavior therapy and biofeedback to laxative therapy in the treatment of pediatric encopresis. Ann Behav Med 20:70–76
Schmiedecke E, Busch M, Stamatopoulos E, Lorenz C (2008) Multidisciplinary behavioural treatment of fecal incontinence and constipation after correction of anorectal malformation. World J Pediatr 4(3):206–210
Langemeijer RA, Molenaar JC (1991) Continence after posterior sagittal anorectoplasty. J Pediatr Surg 26:587–590
Conflict of interest statement
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maerzheuser, S., Schmidt, D., Mau, H. et al. Prospective evaluation of comorbidity and psychosocial need in children and adolescents with anorectal malformation. Part one: paediatric surgical evaluation and treatment of defecating disorder. Pediatr Surg Int 25, 889–893 (2009). https://doi.org/10.1007/s00383-009-2440-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-009-2440-9