
Abstract
Purpose
Middle fossa arachnoid cysts (MFAC) are a relatively common, benign pathology that pose a therapeutic challenge for both symptomatic and asymptomatic patients. The optimal surgical strategy and indication to treat are still debated by neurosurgeons. We reviewed our experience and results in a group of patients treated with endoscopic fenestration with the aim to assess indications to treat and clinical and neuroradiological results.
Methods
The data on 40 patients operated with endoscopic fenestration for MFAC in two centres, “Anna Meyer” Children’s Hospital, Florence, Italy, and Royal Liverpool Children’s Hospital “Alder Hey”, Liverpool, UK, between 2001 and 2007 were retrospectively reviewed with prospective follow-up. We analysed clinical and neuroradiological presentation, indications to treat, surgical technique, complications, and clinical and neuroradiological follow-up.
Results
There were 30 males and ten females: mean age, 7.8 years; mean follow-up, 21 months. The neuronavigation system was used in 12 patients in the English cohort. Thirty-seven patients (92.5%) had a satisfactory clinical outcome. The cyst was reduced in size or completely disappeared in 29 patients (72.5%). There was no death or significant morbidity associated with the procedure. Four patients required further surgical treatment. Four patients experienced a post-traumatic intracystic bleeding after surgery.
Conclusion
Compared to microsurgical fenestration and cyst shunting, our experience with endoscopic fenestration was as effective and safe but less invasive. Each case must be assessed with its individual characteristics to define the optimal surgical strategy. Successful treatment may not reduce the risk of post-traumatic head injury haemorrhage.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Arachnoid cysts are a relatively common pathology accounting for up to 0.75–1% of non-traumatic intracranial mass lesions as reported in autopsy and neuroradiological studies [1, 15, 26, 33, 34]. The middle fossa is the most common location for arachnoid cysts. In larger series, they account for 34% to 50% of all arachnoid cysts [11, 13, 25, 29]. They pose a therapeutic challenge for both adult and paediatric neurosurgeons alike. Although some may consider it a benign pathology, patients with middle fossa arachnoid cyst (MFAC) may develop a range of signs or symptoms which include headache, focal neurology, macrocrania, and hydrocephalus [2, 6, 10–13, 15, 17, 19–21]. Patients with MFAC experience an increased risk of spontaneous and post-traumatic extradural and subdural haemorrhage and subdural hygromas [1, 13, 24, 26, 28, 35]. Many patients present with “functional” symptoms such as seizures and developmental delay, and although direct clinical correlation of these symptoms to MFAC may be tenuous, reports in the literature suggest efficacy in post-operative seizure control and improvement in development [2–4, 10].
The surgical management strategy for MFAC remains a contentious issue within the neurosurgical fraternity. We present our joint series of 40 patients with MFAC. There were 30 males and ten females with a mean age of 7.8 years treated in two centres (the Department of Neurosurgery of the “Anna Meyer” Children’s Hospital, Florence, Italy, and the Department of Neurosurgery of the Royal Liverpool Children’s Hospital “Alder Hey”, Liverpool, UK). All patients were treated with an endoscopic approach as the first line of treatment. The clinical presentation, indications for surgery, surgical technique, early and late complications, and results are presented. We discuss the advantages and disadvantages of endoscopic fenestration versus cyst shunting and microsurgical fenestration.
Patients and methods
Between 2001 and 2007, 40 patients were treated for MFAC with endoscopic fenestration in two centres of Pediatric Neurosurgery, the Department of Neurosurgery of the “Anna Meyer” Children’s Hospital, Florence, Italy, and the Department of Neurosurgery of the Royal Liverpool Children’s Hospital “Alder Hey”, Liverpool, UK. These 40 patients represent only a small portion of the total neuroendoscopic procedures performed at both centres during the time frame of this study. All case notes and neuroradiological studies were reviewed with prospective follow-up. Clinical presentation, pre-operative cyst size and classification, treatment, clinical evolution, and post-operative cyst size at the most recent neuroradiological investigation were recorded.
Population
There were 30 males and ten females (M:F; 3:1) with a mean age at presentation of 7.8 years (3 months–30 years; median 5.4 years). All patients had a unilateral cyst, on the left side in 28 cases and on the right side in 12 cases (L:R; 2.8:1). Mean follow-up was 21 months (1–73 months).
Technique
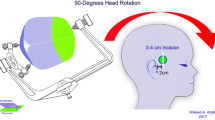
All patients were treated with endoscopic cystocisternal fenestration as first line of surgical treatment. In the UK group, all the procedures were performed freehand with a 3-mm diameter rigid endoscope (Gaab II Karl Storz, B-Braun miniscope or single-use disposable Medtronic scope), whilst the Italian group used a 3.2-mm rigid paediatric neuroendoscope (LG Karl Storz). In the UK group, the image-guided neuronavigation system (StealthStation Medtronic) was used in eight cases and the ‘SureTrak’ electromagnetic neuronavigation in four (StealthStation AxiEM technology Medtronic; Fig. 1).

Intraoperative view using electromagnetic guidance. The target for marsupialisation of a middle fossa arachnoid cyst is indicated
The surgical technique performed in all patients in both groups was similar; after minimal hair shaving, an incision and burr hole is made behind the hairline above the root of the zygoma on the side of the cyst, followed by dissection of the temporalis muscle. Dura mater and the external cyst membrane are opened, and the endoscope is advanced guided by the identification of the anatomical landmarks with or without the frameless image-guided neuronavigation system.
The fenestration target is identified as the membrane between the optic nerve, the internal carotid artery, and the III cranial nerve (Figs. 2 and 3) and is created utilising a Lighttouch balloon catheter (Integra Neuroscience) as the preferred instrument of choice. If ineffective, a rigid electrode without current or blunt forceps (used as a blunt probe) was the next instrument of choice. If the fenestration is still not realised, then the rigid electrode is used with current keeping away from neurovascular structures (used only in one case). Once the fenestration is achieved, it is gently enlarged by inflating the balloon. If the size of the fenestration after repeat balloon inflation is deemed inadequate, it is extended using micro-scissors. The cystocisternal communication is considered satisfactory when it is possible to directly view the basilar artery and cerebrospinal fluid (CSF) pulsation through the fenestration. A cyst wall biopsy specimen was always taken in the Italian group to confirm the diagnosis of arachnoid cyst. The procedure was not abandoned in any case in this series.

Intraoperative view of the anatomic landmarks for fenestration in the prepontine cistern

Intraoperative view. The Lighttouch balloon passes through the medial wall of the cyst
Results
Clinical presentation
Patient signs and symptoms at presentation were divided into five categories (Table 1): (1) neurological deficit, (2) signs and/or symptoms related to intracranial hypertension, (3) skull deformity, (4) functional symptoms, and (5) others signs and/or symptoms. Most patients experienced more than one sign or symptom in combination.
Focal neurology
Eight (20%) patients presented with one or more abnormalities on the neurological examination. Two had VI cranial nerve palsy, nystagmus was present in two, ataxic gait in one, optic nerve atrophy with visual field impairment in one, paraesthesia in one, dysphasia in two, and papilloedema in one.
Signs and/or symptoms related to intracranial hypertension
Fifteen (37.5%) patients presented with headache; two developed a VI cranial nerve palsy; one presented with a reduced level of consciousness; and papilloedema was present in one patient. Ventriculomegaly was present in four (10%) patients. In two of these, there was associated skull deformity.
Skull deformity
In nine (22.5%) patients, macrocrania with or without temporal bone bossing and thinning was present.
Functional symptoms
Eleven (27.5%) patients had functional symptoms on presentation; including head bobbing (one patient) and speech delay (two patients). Epilepsy was noted in eight patients and developmental delay in six (including autism and cerebral palsy). One of the patients in the developmental delay subgroup was also affected by tuberous sclerosis. The indications for surgery in this group are not well established and are open to subjective interpretation. Therefore, surgery was only offered after careful and detailed discussion with the patients parents regarding the perceived potential benefits and the risk of failure to achieve improvement.
Other non-functional signs and/or symptoms
Seven (17.5%) patients presented with different signs and/or symptoms. Dizziness was reported by four patients, two presented with failure to thrive, and one with blackout episodes.
All but three patients underwent neuroradiological studies with computed tomography (CT) and magnetic resonance (MR) as part of the investigative work-up resulting from one or more signs and/or symptoms at presentation linked to their MFAC (Table 1). Three previously asymptomatic patients underwent CT head scanning subsequent to a head injury, leading to the incidental discovery of a MFAC. Of these cases, one developed headache, paraesthesia, and dysphasia, which were linked to the MFAC. In one patient, the CT head scan revealed features of increased intracranial pressure (ICP; bossing and thinning of the temporal bone) related to the MFAC. The third patient remained asymptomatic, but neuroradiological follow-up revealed a progressive increase in the size of the MFAC with concomitant mass effect.
The neuroradiological features of the MFAC were graded according to the Galassi classification [8], which divides arachnoid cysts into three types. Type I is small, biconvex, or spindle-shaped and is limited to the anterior middle cranial fossa. Type II involves the proximal, intermediate, and superior segments of the Sylvian fissure with displacement of the temporal lobe. Type III is large, occupies the entire middle cranial fossa with fronto-temporo-parietal displacement, and is associated with bony expansion and bossing of the squamous temporal bone. Type I cysts were present in five patients (12.5%), type II cysts in 17 (42.5%), and type III cysts in 18 (45%; Table 2).
Surgical treatment
Surgical treatment was recommended in MFAC patients with any of the following: focal neurological deficits, skull deformities, and/or signs and/or symptoms related to increased ICP. One patient incidentally diagnosed after a head injury was offered surgical treatment because of a progressive increase in size of a type III MFAC with mass effect and midline shift. MFAC patients with developmental delay alone were excluded from this series, as this was not considered an indication for surgical treatment. Similarly, patients who presented with seizures alone were not considered for surgery in the first instance. They were considered suitable for surgical treatment only if their seizures were refractory to medical treatment and/or other surgical treatment, with concomitant neuroradiological investigation demonstrating MFAC mass effect and/or increase in size. Surgery was performed for this indication in three of the Italian patient cohort. Asymptomatic patients with static MFAC size at two yearly radiological follow-up were not considered for surgical treatment and excluded from this series. Of the four patients with concomitant ventriculomegaly, one required an additional specific treatment with endoscopic third ventriculostomy.
Clinical outcome
A summary of the post-operative results is presented in Table 3. Follow-up for patients from both centres ranged from 6 to 79 months with a mean of 27 months. A satisfactory outcome was obtained in 37 patients (92.5%; Table 3). A complete resolution of the pre-operative signs and/or symptoms was obtained in 25 patients (62.5%) and a significant improvement in 12 patients (30%). Clinically, the most likely symptom to improve was headache, with complete relief or a significant improvement in 14 patients (93.3%). Improvement in skull deformities was obtained in all the nine cases (100%). Among the patients with abnormalities on neurological examination, six (75%) recovered completely or improved. Nystagmus, VI cranial nerve palsy, and papilloedema recovered completely in all cases (five patients). In the patient with optic nerve atrophy, progressive visual field impairment was halted post-operatively, whilst the patient suffering blackouts had no repeat post-operative episodes. Dizziness resolved completely in two patients and improved in one.
Among the eight patients with seizures at presentation, seven improved after surgery. Six of them had a better control or were seizure-free on medical therapy and one was seizure-free with no medication at last follow-up. No improvement was reported in one patient. None of the patients with developmental delay improved after surgery.
Neuroradiological outcome
A summary of the post-operative imaging is presented in Table 3. All patients underwent a CT head scan the day after surgery and MR at 3, 6, and 12 months and then on a yearly basis. At the last MR scan, 24 patients (60%) showed a reduction in size of the cyst. Of this group, their corresponding Galassi classification at diagnosis was a type I cyst in one case, type II in nine cases, and type III in 14 cases. In five patients (12.5%), the cyst disappeared completely; these were type I cysts in two cases, type II in one case, and type III in two cases at diagnosis (Figs. 4 and 5). Cysts were unchanged in nine patients (22.5%); these were a type I cyst in one case, type II cyst in six, and type III in two at diagnosis. Two patients (5%), one with a type I and one with a type II cyst demonstrated a small post-operative increase in size but did not receive any further treatment because they were completely asymptomatic, with the cyst not demonstrating radiological mass effect (Table 4). Of the four patients with concomitant hydrocephalus, only one required specific treatment (endoscopic third ventriculostomy) while the ventricular size reduced in the remaining three after endoscopic cystocisternostomy.

Pre-operative cranial computed tomography scan

Post-fenestration cranial computed tomography scan in the same patient 6 months after surgery demonstrating significant reduction in cyst volume
Complications
There was no mortality or additional post-operative neurological deficit in this series. The main complication was subdural hygroma, developed by five patients of whom four required subdural-peritoneal shunting. Other post-operative complications treated conservatively were rhinoliquorrhea (one patient) and subcutaneous collection (one patient). One patient developed post-operative bacterial meningitis and recovered completely with antibiotics.
Post-operative traumatic subdural haemorrhage was a long-term complication in four patients 3 to 60 months after surgery (Fig. 6). At the last follow-up before head injury, all four patients were completely asymptomatic, and the cyst had disappeared in two, was reduced in one, and was unchanged in one patient. They all required specific surgical treatment for the subdural haemorrhage resulting in complete recovery.

Subdural haematoma ipsilateral to the cyst. The haemorrhage occurred 60 months post-fenestration subsequent to a relatively trivial head injury
Endoscopic fenestration failure occurred in four patients (10%) necessitating repeat surgical treatment. One patient was treated with cysto-peritoneal shunting, while three were treated with a redo-endoscopic fenestration: in all of them, the previous cystocisternostomy had closed over. Redo-endoscopic fenestration had a good outcome in one but failed in two patients. Of the two that failed on redo, one improved transiently after mini-craniotomy fenestration and cyst marsupialisation but deteriorated again 3 months later; whereas, the other patient refused any further surgical treatment.
Discussion
The debate on the indications and best surgical treatment for primary MFAC still continues. Their pathophysiological relationship with other intracranial structures is incompletely understood. Studies with water-soluble contrast CT cisternogram [8, 15] reveal a communication between the cyst and the subarachnoid space. The closure of this communication, a one-way pulsatile mechanism at the point of the communication [5], an increased osmotic gradient, e.g., after a minor intracystic bleeding [1], and an increased production of fluid from the cyst wall [29] are all postulated to explain an increase in size of the cyst/ICP and/or compression on the surrounding structures. This in turn would then potentially induce the onset of signs and/or symptoms, as described by Wester and Moen [37]. Nevertheless, it is not unusual for a patient with a type III MFAC to remain completely asymptomatic over a lengthy follow-up period; whereas, a type I MFAC may produce neurological signs and/or symptoms attributable to raised ICP.
It is worth noting that a previous study on prolonged ICP monitoring in MFAC [7] ruled out the indication for surgery in children with type I cysts for raised ICP and confirmed the almost constant increase of the ICP in children with type III cysts. Indeterminate results were obtained in children with type II cysts. Other studies suggest that intracystic pressure in all types of cyst appears to be within the normal range of ICP, raising the possibility that symptomatic patients and patients with type III MFAC could have normal ICP [12].
The relationship between MFAC and functional symptoms, seizures, and developmental delay is poorly understood. Studies with single photon emission computed tomography suggest a reduction of cerebral perfusion not only to the brain surrounding the cyst but also to the contralateral hemisphere [22, 30], offering a possible explanation for focal neurology and functional symptoms [22, 30]. However, cerebral blood flow has been shown to increase after surgery as well as in patients treated conservatively [30]. Cognitive tests administered before and after surgery demonstrate an improvement in performance after treatment [4]. Functional MR imaging investigations indicate that MFACs do not interfere with the normal structure of the cortex [14]. Although seizures are reported in up to 25–33.7% of patients with MFACs [2, 21], the incidence of arachnoid cysts in a population of epileptic patients is very low, around 0.02% according to Arroyo and Santamaria [3].
Most within the neurosurgical fraternity would agree on prompt treatment for MFAC patients presenting with symptoms of raised ICP or objective acute onset neurological deficit resulting from cyst mass effect [3, 5, 21]. Far less certain is the indication to treat asymptomatic patients and patients with vague and subtle functional signs or symptoms. Some authors have proposed that asymptomatic patients should be offered surgery [26, 35] because of the recognised increased risk of bleeding and rupture of arachnoid cysts after minor head injury. MFAC haemorrhage and rupture has also previously been linked to consequent MFAC growth [1, 19, 20, 24, 26, 27, 35, 37].
Another argument for surgery in asymptomatic patients is the hazardous effect of chronic compression and persistent reduction of cerebral blood flow on the developing brain [22, 30, 36]. Our opinion is that it is not possible to estimate these risks because the incidence and natural history of MFACs is undetermined. Therefore, our practise is to preferably manage asymptomatic patients conservatively unless neuroradiological investigations reveal a progressive increase in size and/or a significant mass effect. Moreover, our experience with late post-traumatic haemorrhages in four apparently successfully decompressed post-operative MFAC cases reinforces our position.
Our treatment of choice in all cases was endoscopic cystocisternal fenestration. The rationale for this choice was based on the principles of employing the least invasive surgical technique without the use of implant devices to reduce the related risks of infection and malfunction. Incorporating the electromagnetic guidance system latterly conferred the potential benefit of accuracy and safety within the context of a minimally invasive procedure.
Compared to open craniotomy, endoscopic fenestration is performed through a single burr hole and allows for a quicker procedure in expert hands. Frameless neuronavigation allows us to determine the optimal entry point, allows us to plan the trajectory, provides real-time control of the endoscope position, and allows for tracking of the fenestration probe tip. This provides increased accuracy and safety with the caveat being the danger of neglecting intra-procedural brain shift. Compared to cyst shunting, endoscopic cystocisternostomy obviates the requirement for an implant device with its well-documented inherent risks. The main complication we encountered was subdural hygroma (five patients, 12.5%) requiring surgical treatment with subduro-peritoneal shunt in four. It is worth noting that this complication rate is also well recognised in patients undergoing treatment with craniotomy and wide marsupialisation of the cystic membrane, although in one large series, the post-operative incidence of subdural hygroma was only 5.8% [31]. Other surgical-related complications were a subcutaneous collection in one patient (2.5%), CSF rhinoliquorrhea in one patient (2.5%), and CSF infection in one patient (2.5%).
We obtained a good clinical outcome with complete recovery or significant improvement with endoscopic fenestration in 37 patients (92.5%). Headache was the most likely symptom to improve, with a completely recovery or significant improvement in 14 patients (93.3%), while abnormalities on neurological examination and the other non-functional signs and/or symptoms resolved or improved in 11 (78.4%). This result compares favourably with other reported series. Levy et al. [20] had an improvement or a complete recovery in 95% of patients in a series of 50 patients who underwent craniotomy and microsurgical fenestration. Two patients in their series required a cysto-peritoneal shunt, and 16 experienced a complication: pseudomeningocele in five (with one patient requiring further surgery), CSF leak in three, transient third cranial nerve palsy in three, post-operative seizure in one, CSF infection in two, and subdural hygroma in two patients.
Arai et al. [2] performed cysto-peritoneal shunts in 77 patients with MFAC, reporting complete resolution in all cases of headache, hemiparesis, chocked disc, diplopia, and macrocrania (35 patients); eight patients in their series required further surgical treatment for shunt malfunction with a total of 12 operative procedures with one shunt infection, one transient oculomotor palsy, and one extradural haematoma. Similar results are obtained by smaller studies treated with craniotomy or shunt CSF diversion [9, 11, 13, 23].
The surgical treatment of patients with functional symptoms is possibly supported by the empirical observation of improvement in seizure control reported by several authors [2, 16, 18, 20]. Those with seizures and developmental delay are potentially the most challenging to manage/advise on. Indications for treatment remain blurred with parents often hoping for a ‘miracle cure’ after discovery of a cyst as part of an investigative work-up for other clinical indications. The focus then shifts towards the surgical option and it may become very difficult to persuade parents that the symptoms are unlikely to improve with surgery. In our series, patients with seizures were treated only if presenting with headache and/or macrocrania and/or focal neurology and/or progressive increase in size of the cyst with mass effect on neuroradiological imaging.
We observed a surprisingly good outcome in patients with seizures associated with focal neurology and/or signs of increased ICP. Of the eight patients (20%) who presented with seizures and were surgically treated, six had better seizure control with medication, and one was seizure-free off medication at the last follow-up. We had no cases of increased seizures post-operatively; however, this complication has been previously described [2, 20]. This echoes the findings and opinions of several other authors who recommend epilepsy as a potential indication for surgery in some cases with other concomitant signs or symptoms [2] or in cases where the seizures are refractory to medication [9]. Levy et al. [21] reported an improvement in seizure control in their series in 50% of cases; in the series by Arai et al. [2], 21 patients out of 26 with seizures continued to require antiepileptic medication after surgery, while one was seizure-free off medication; three of them developed medication resistance after surgery, and one died from status epilepticus. Patients with developmental delays did not improve in any of our cases, and similar results are reported by other authors after microsurgical fenestration and cysto-peritoneal shunting [2, 21]. It is of note that one study demonstrated post-surgical neuropsychological improvement in cognitive function [4].
One of the classic indications for treatment often quoted at neurosurgical meetings and in the literature even in asymptomatic patients is the risk of haemorrhage, either spontaneously or from minimal trauma [32]. Our group has not recommended prophylactic surgery for asymptomatic MFACs; however, we have had a similar experience with the inherently higher risk of haemorrhage in these patients.
Four patients in our series suffered a head injury 3 to 60 months after successful surgery resulting in chronic subdural haematoma in three and acute subdural haematoma in one directly subsequent to the trauma. In all of them, the haemorrhage was ipsilateral to the cyst and required surgical treatment. An important finding in this subgroup was that the cysts in those patients had reduced in size in two of them, disappeared in one, and remained unchanged in one; and they were all asymptomatic at the last follow-up (3 to 60 months) before the trauma. Intracystic haemorrhage is a well-known complication associated with MFAC [1, 24, 26], and some authors advocate the risk of spontaneous or post-traumatic bleeding as an indication for surgery even in asymptomatic patients [26, 35]. The experience from our series suggests that surgery for symptomatic MFAC did not result in reducing the risk of traumatic haemorrhage after head injury. It is difficult to explain this result; however, it may be due to the persistence of the cyst membrane, which has abundant small vessels, or it could result from an intrinsic increased risk of haemorrhage after a recent neurosurgical procedure.
MFACs have been associated with high post-operative recurrence rates (due to membrane thickness and vascularity) [5] potentially facilitated by a higher risk of early fenestration closure. Consequently, some authors have proposed that performing a mini-craniotomy marsupialisation may reduce such a risk. The results from our series have not demonstrated a higher risk of early fenestration closure resulting from endoscopic cystocisternostomy. Although we would still advocate the use of neuroendoscopy in a repeat procedure if required, we maintain that certain difficult cases presenting with further clinical deterioration, may require mini-craniotomy marsupialisation or CSF shunting as second or third line management options. Conversely, in asymptomatic patients, the option of conservative follow-up with interval neuroradiology imaging would be reasonable and appropriate.
Complications
Our series complication rate compares favourably to the existing literature; however, the post-operative subdural hygroma rate remains significant. It should, however, be clarified that the potential to cause harm, particularly to the internal carotid artery, should not be underestimated due to the close anatomical proximity of this structure to the fenestration. The technique of MFAC endoscopic fenestration should therefore preferably be performed by experienced neurosurgeons.
Conclusion
The endoscopic approach, as a first line management to these cysts when clinically indicated, offers comparable results to shunts and craniotomy in terms of symptom control. However, the rate of complete radiological resolution of the cyst is probably lower than in these alternative techniques.
Nevertheless, the main advantage is avoidance of implant in the case of shunt (and its longer-term complications) and avoidance of a larger scar in the case of open craniotomy. The complications remain not insignificant—particularly in terms of post-operative hygromas and some late haemorrhages. Fortunately, significant neurological sequelae remain few, although the potential for harm in this area must still be recognised as being potentially high.
One important finding in our series is the incidence of post-traumatic chronic/acute subdural hematomas in children despite long-term neuroradiological confirmation of MFAC size reduction and symptom resolution. This may have implications against the recommendation for surgically treating asymptomatic MFAC patients as a preventative measure against post-traumatic haemorrhages [32].
In experienced hands, the endoscopic technique, as a first line treatment, is a reasonable technique to offer in these patients with few neurological sequelae. The families must be warned that with this technique, the cyst may never fully disappear in a significant portion of patients and of the potential for the complications described. A second line of repeat endoscopy, craniotomy, or shunt may have to be considered in failures or complications with subdural collections.
It is recognised that this retrospective review of our particular management approach to these cysts may not necessarily indicate which of the common or alternative techniques used is the best choice in all cases of MFAC. In the absence of a randomised trial, this discussion is likely to continue. Nevertheless, we have demonstrated that the minimally invasive neuroendoscopic approach is safe in our hands and offers good symptom control.
References
Albuquerque FC, Giannotta SL (1997) Arachnoid cyst rupture producing subdural hygroma and intracranial hypertension: case report. Neurosurgery 41:951–956
Arai H, Sato K, Wachi A, Okuda O, Takeda N (1996) Arachnoid cysts of the middle cranial fossa: experience with 77 patients who were treated with cystoperitoneal shunting. Neurosurgery 39:1108–1113
Arroyo S, Santamaria J (1997) What is the relationship between arachnoid cysts and seizure foci? Epilepsia 38(10):1098–1102
Baroey Raeder M, Helland CA, Hugdahl K, Wester K (2005) Arachnoid cysts cause cognitive deficits that improve after surgery. Neurology 64:160–162
Choi JU, Kim DS, Huh R (1999) Endoscopic approach to arachnoid cyst. Childs Nerv Syst 15:285–291
Di Rocco C, Caldarelli M, Ceddia A (1993) Incidence, anatomical distribution and classification of arachnoidal cysts. In: Raimondi A, Choux M, Di Rocco C (eds) Intracranial cysts lesions. New York, Springer Verlag, pp 101–111
Di Rocco C, Tamburrini G, Caldarelli M, Velardi F, Santini P (2003) Prolonged ICP monitoring in Sylvian arachnoid cysts. Surg Neurol 60:211–218
Galassi E, Tognetti F, Gaist G, Fagioli L, Frank F, Frank G (1982) CT scan and medtrizamide CT cisternography in arachnoid cysts of the middle cranial fossa: classification and pathophysiological aspects. Surg Neurol 17:363–369
Hamid NA, Sgouros S (2005) The use of an adjustable valve to treat over-drainage of a cyst-peritoneal shunt in a child with a large sylvian fissure arachnoid cyst. Childs Nerv Syst 21:991–994
Harsh GR, Edwards MSB, Wilson CB (1986) Intracranial arachnoid cysts in children. J Neurosurg 64:835–842
Helland CA, Wester K (2006) A population based study of intracranial arachnoid cysts: clinical and neuroimaging outcomes following surgical cyst decompression in children. J Neurosurg (Pediatrics) 105:385–390
Helland CA, Wester K (2007) Intracystic pressure in patients with temporal arachnoid cysts: a prospective study of preoperative complaints and postoperative outcome. J Neurol Neurosurg Psychiatry 78:620–623
Helland CA, Wester K (2007) A population based study of intracranial arachnoid cysts: clinical and radiological outcome following surgical cyst decompression in adults. J Neurol Neurosurg Psychiatry 78:1129–1135
Hund-Georgiadis M, von Cramon Y, Kruggel F, Preul C (2002) Do quiescent arachnoid cysts alter CNS functional organization? AfMRI and morphometric study. Neurology 59:1935–1939
Kanev PM (2004) Arachnoid cysts. In: Winn HR (ed) Youmans neurological surgery, 5th edn. Philadelphia, Saunders, pp 3289–3299
Kang JK, Lee KS, Lee IW, Jeun SS, Son BC, Jung CK, Park YS, Lee SW (2000) Shunt-independent surgical treatment of middle fossa arachnoid cysts in children. Childs Nerv Syst 16:111–116
Karabatsou K, Hayhurst C, Buxton N, O’Brien DF, Mallucci CL (2007) Endoscopic management of arachnoid cysts: an advancing technique. J Neurosurg (Pediatrics) 106:455–462
Koch CA, Voth D, Kraemer G, Schwarz M (1995) Arachnoid cysts: does surgery improve epileptic seizures and headaches? Neurosurg Rev 18:173–181
Lena G, Erdincler P, Van Calenberg F, Genitori L, Choux M (1996) Arachnoid cysts of the middle cranial fossa in children. A review of 75 cases, 47 of which have been operated in a comparative study between membranectomy with opening of cisterns and cystoperitoneal shunt. Neurochirurgie 42:29–34
Levy ML, Meltzer HS, Hughes S, Aryan HE, Yoo K, Amar AP (2004) Hydrocephalus in children with middle fossa arachnoid cysts. J Neurosurg (Pediatrics) 101:25–31
Levy ML, Wang M, Aryan HE, Yoo K, Meltzer H (2003) Microsurgical keyhole approach for middle fossa arachnoid cyst fenestration. Neurosurgery 53:1138–1145
Martinez-Lage JF, Valenti JA, Piqueras C, Ruiz-Espejo AM, Roman F, Nuno de la Rosa JA (2006) Functional assessment of intracranial arachnoid cysts with TC99 m-HMPAO SPECT: a preliminary report. Childs Nerv Syst 22:1091–1097
McBride LA, Winston KR, Freeman JE (2003) Cystoventricular shunting of intracranial arachnoid cysts. Pediatr Neurosurg 39:323–329
Mori T, Kujimoto M, Sakae K, Sakakibara T, Shin H, Yamaki T, Ueda S (1995) Disappearance of arachnoid cysts after head injury. Neurosurgery 36:938–942
Oberbauer RW, Haasa J, Pucher R (1992) Arachnoid cysts in children: a European co-operative study. Childs Nerv Syst 8:281–286
Parsch CS, Krauss J, Hofmann E, Meixensberger J, Roosen K (1997) Arachnoid cysts associated with subdural hematomas and hygromas: analysis of 16 cases, long term follow up, and review of the literature. Neurosurgery 40:483–490
Peter JC, Fieggen G (1999) Congenital malformations of the brain—a neurosurgical perspective at the close of the twentieth century. Childs Nerv Syst 15:635–645
Rakier A, Feinnsod M (1995) Gradual resolution of an arachnoid cyst after spontaneous rupture into subdural space. J Neurosurg 83:1085–1086
Rengachary S, Watanabe I, Brackett C (1978) Pathogenesis of intracranial arachnoid cysts. Surg Neurol 9:139–144
Sgouros S, Chapman S (2001) Congenital middle fossa arachnoid cysts may cause global brain ischaemia: a study with 99Tc-Hexamethylpropyleneamineoxime single photon emission computerised tomography scans. Pediatr Neurosurg 35:188–194
Tamburrini G, Caldarelli M, Massimi L, Santini P, Di Rocco C (2003) Subdural hygroma: an unwanted result of Sylvian arachnoid cyst marsupialization. Childs Nerv Syst 19:159–165
Tamburrini G, Del Fabro M, Di Rocco C (2008) Sylvian fissure cysts: a survey on their diagnostic workout and practical management. Childs Nerv Syst 24:593–604
Van Burken MMG, Sarioglu AC, O’Donnell HD (1992) Supratentorial arachnoidal cyst with intracystic bleeding and subdural hematoma. Neurochirurgia 35:199–203
Von Wild K (1992) Arachnoid cysts of the middle cranial fossa. Neurochirurgia 35:177–182
Wester K, Helland CA (2008) How often do chronic extra-cerebral haematomas occur in patients with intracranial arachnoid cysts? J Neurol Neurosurg Psychiatry 79:72–75
Wester K, Hugdahl K (2003) Verbal laterality and handedness in patients with intracranial arachnoid cysts. J Neurol 250:36–41
Wester K, Moen G (2000) Documented growth of a temporal arachnoid cyst. J Neurol Neurosurg Psychiatry 69:699–700
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Spacca, B., Kandasamy, J., Mallucci, C.L. et al. Endoscopic treatment of middle fossa arachnoid cysts: a series of 40 patients treated endoscopically in two centres. Childs Nerv Syst 26, 163–172 (2010). https://doi.org/10.1007/s00381-009-0952-1
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-009-0952-1