
Abstract
Introduction
Cystic lesions in and around the third ventricle have been known to cause intermittent and acute obstruction of the foramen of Monroe with rapid onset symptoms. Most of these lesions are seen on routine investigations, whereas some are not so obvious resulting in mistaken diagnosis. Symptomatic choroids plexus cysts have only been infrequently reported, predominantly in the lateral ventricle.
Case report
A 3-year-old female child presented with rapid loss of consciousness for the first time. Computed tomography and magnetic resonance imaging scans only showed triventriculomegaly. Endoscopy revealed a cyst of the third ventricle, which was excised, leading to good recovery. Biopsy of the wall revealed a choroid plexus cyst.
Conclusion
Choroid plexus cysts are rare causes for symptomatic obstruction of the third ventricle and may be difficult to detect on routine investigations and may lead to the wrong choice of treatment. Endoscopic fenestration or excision is a good option to manage such lesions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cysts of the third ventricle can present with acute hydrocephalus. When presenting for the first time, the only obvious feature in routine imaging may be triventriculomegaly, which may sometimes lead to error in management.
Case report
A previously healthy 3-year-old female child of nonconsanguineous parents presented to another hospital with the history of rapidly deteriorating sensorium associated with vomiting that was preceded by a low-grade fever.
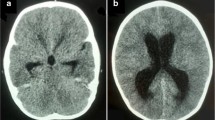
When first seen by the pediatric services, the child was lethargic with signs of meningeal irritation. With a suspicion of meningo-encephalitis, she had a lumbar cerebrospinal fluid (CSF) study, which was normal. A toxicology screen was also done to rule out poisoning, which was negative. A computed tomography (CT) scan showed triventriculomegaly (Fig. 1) The child recovered over the next 12 h and, when first seen by the neurosurgical services, was alert but still bedridden with no focal deficits and normal fundus.

Nonenhanced CT scan showing triventriculomegaly
A magnetic resonance imaging (MRI) of the brain (Fig. 2) showed moderate triventriculomegaly with minimal asymmetry of the foramen of Monroe. With a diagnosis of aqueduct stenosis, she was taken up for an endoscopic third ventriculostomy. At surgery, which was performed through a right precoronal burrhole, a cyst wall was seen occluding the foramen of Monroe from within the third ventricle. The choroid plexus was seen adherent to it. The translucent wall was coagulated and fenestrated to release clear fluid. Most of the thin wall was then excised, and the rest coagulated and shrunk till the third ventricle and both foramen were free (Fig. 3).

Contrast-enhanced MRI scan showing a mild asymmetry of ventricles and narrow foramen of Monroe but no obvious cyst

Endoscopic view before and after cyst excision
The wall biopsy showed a cyst wall attached to the choroids plexus lined by cuboidal epithelium suggestive of a choroid plexus cyst (Fig. 4). The child recovered rapidly, and a CT scan at 3 months showed normal ventricles (Fig. 5).

Photomicrograph of cyst wall (hematoxylin and eosin) showing cuboidal epithelium lining

Contrast-enhanced CT scan 3 months after surgery showing normal ventricles
Discussion
Third ventricular cysts, especially colloid cysts, are known to cause acute or intermittent obstruction of the ventricular system resulting in drop attacks, sudden loss of consciousness, and even sudden death [1].
Choroid plexus cysts have been thought to be a variant of normal development and can be seen in up to 2.3% of normal fetuses during sonography and most disappear by 24 weeks of gestation [2]. Even those that persist remain asymptomatic. Larger cysts, especially in the region of the foramen of Monroe, can, however, become symptomatic. Most of those reported are primarily in the lateral ventricle [3]. Third ventricular choroid plexus cysts are rarer still [2, 4, 5]. Moreover, these cysts, unlike colloid cysts, are difficult to detect on routine CT and MRI, due to the thin nonenhancing walls and CSF-like fluid content. They mimic an aqueductal stenosis except for mild asymmetry of the lateral ventricles, asymmetry of position of the foramen of Monroe, or shape of the third ventricle, as was evident in this case too, on close observation. Neurosonography is extremely useful when the fontanel is open [2] and can even demonstrate the intermittent obstruction [5]. CT ventriculography has also been used when the diagnosis was strongly suspected [2, 3] but is invasive in nature. Special magnetic resonance sequences like constructive interference in steady state (CISS) have also been described to be useful in picking up these cysts but are again not performed routinely [6].
Other than being a curiosity, the significance of this case lies in the fact that with intermittent obstruction, the ventriculomegaly might not be significant during the recovery phase after an acute event, and the cyst itself may not be obvious especially if it is floppy [5].
The arrival at a proper preoperative diagnosis is even more important in deciding the correct procedure. A shunt in this situation will only result in draining one side if the septum pellucidum is competent. Endoscopic fenestration, on the other hand, is a simple solution and is probably an enduring one, even if a partial excision is done [6]. Total excision of the cyst through a craniotomy can also be done, if a preoperative diagnosis is achieved, but is obviously a more extensive procedure.
Conclusion
The conclusions of the study are as follows:
-
1.
Choroid plexus cysts are rare causes for symptomatic obstruction of the third ventricle with atypical presentations that may be mistaken for other conditions.
-
2.
Triventriculomegaly, when presenting acutely, should be viewed with caution.
-
3.
An MRI often gives clues to the presence of a third ventricular cyst, though not obvious at first glance.
-
4.
Endoscopic procedures are ideally suited for the management of such cysts.
References
Kava MP, Tullu MS, Deshmukh CT, Shenoy A (2003) Colloid cyst of the third ventricle: a cause of sudden death in a child. Indian J Cancer 40:31–33
Lam AH, Villanueva AC (1992) Symptomatic third ventricular choroid plexus cysts. Pediatr Radiol 22:413–416
Parizek J, Jakubec J, Hobza V, Nemeckova J, Cernoh Z, Sercl M, Zizka J, Spacek J, Nemecek S, Suba P (1998) Choroid plexus cyst of the lateral ventricle with intermittent blockage of the foramen of Monroe, and initial invagination into the III ventricle in a child. Child’s Nerv Syst 14:700–708
Radaideh MM, Leeds NE, Kumar AJ, Bruner JM, Sawaya R (2002) Unusual small choroid plexus cyst obstructing the foramen of Monroe: case report. Am J Neuroradiol 23:841–843
van Baalen A, Stephani U (2007) Flexible and floating choroid plexus cyst of the third ventricle: an ultrasonographic video documentation. Childs Nerv Syst 23:259–261
Vlaho S, Gebhardt B, Gerlach R, Weidauer S, Kieslich M (2003) Cyst of the third ventricle as an unusual cause of acquired hydrocephalus. Pediatr Neurol 28:225–227
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kariyattil, R., Panikar, D. Choroid plexus cyst of the third ventricle presenting as acute triventriculomegaly. Childs Nerv Syst 24, 875–877 (2008). https://doi.org/10.1007/s00381-008-0622-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-008-0622-8