
Abstract
Introduction
Children may be more vulnerable to diagnostic radiation exposure because of the increased dose–volume ratio and the increased lifetime risk per unit dose of radiation from early exposure. Moreover, recent radiological literature suggests that exposure to ionizing radiation from imaging studies may play a role in the later development of malignancies.
Materials and Methods
We review the literature and present two illustrative clinical examples of children (each child developed head and neck malignancies during their late teen years) with hydrocephalus requiring multiple cerebrospinal fluid (CSF) shunt revisions and diagnostic computerized tomography (CT) scans throughout their life.
Discussion
The literature reviewed suggests that children are more prone to diagnostic radiation exposure. Although it is not possible to prove that the multiple diagnostic studies result in malignancies, our review of the literature and illustrative cases describing malignancy risk and radiation exposure should give clinicians pause when considering requesting multiple diagnostic CT studies in children during the evaluation of possible CSF shunt dysfunction. Alternative tests such as “shunt MRI” protocols should be considered for patients and used whenever possible to minimize exposure to ionizing radiation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The recent radiological literature suggests that exposure to ionizing radiation from imaging studies may play a role in the later development of malignancies, particularly in children [2–16, 18, 21, 23, 24, 26, 31, 32, 35, 36–39]. Children are more vulnerable because of the increased dose–volume ratio and the increased lifetime risk per unit dose of radiation from early exposure [5–8, 10, 11, 13, 15, 19, 20, 22, 25, 29, 30, 34]. Although increased recognition of this potential problem has led to the generalized adoption of protocols to minimize radiation exposure while maintaining imaging quality, repetitive diagnostic imaging, particularly with computerized tomography (CT), likely carries cumulative risk of inducing malignancy. We review this literature and present two illustrative examples of shunted hydrocephalic children who developed malignancies of the head and neck later in childhood.
Materials and methods
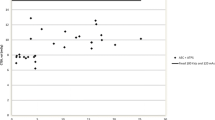
A PubMed online search was performed to try and identify reported cases or reviews in the English language literature using the following search terms: “induced malignancy, induced tumor, pediatric CT, radiation-induced tumor, diagnostic CT, case report, and radiation risk.” Additionally, we present two illustrative cases of patients (one each at Children’s Hospital, St. Louis, MO, USA and Children’s Hospital, Birmingham, AL, USA) with a history of shunted hydrocephalus who presented with newly diagnosed head and neck malignancies. To specify the amount of radiation received, medical records were retrospectively reviewed to ascertain lifetime exposure to diagnostic ionizing radiation (skull films and head CT scans). Cumulative doses of radiation were estimated based on the CT protocols utilized at the time at each institution. Effective doses for each patient were calculated using published factors for pediatric cases, adjusting for the age of the patient at the time of each scan [5–8]. The CT scanners used at both institutions changed over the years for each patient, and the majority of scans obtained preceded our current special techniques for minimizing radiation for pediatric cases. The effective dose calculated for a single scan using those techniques is 160 mrems. The age-adjusted effective dose from each scan was calculated using published factors (Table 1), then summed for a total lifetime effective dose for each patient.
Illustrative cases
Case 1
This was a then 18-year-old Caucasian male diagnosed with cerebral palsy and hydrocephalus as an infant. At 3 weeks of age, a ventriculoperitoneal shunt was inserted. He suffered from frequent severe headaches and has undergone 23 ventriculoperitoneal shunt revisions to date. His headaches were described as dull, non-positional, and not associated with nausea or vomiting. An endoscopic third ventriculostomy had been performed in the past but ultimately failed. There was no family history of migraines. Intracranial pressure monitoring has been performed twice in this boy during the workup of shunt failures. Each revision has been preceded by CT imaging of the head; at the institution where he received most of his neurosurgical care, he has undergone a total of 23 head CTs and 25 plain skull radiographs prior to the age of 17. It is also likely that other studies were performed at other emergency rooms but are not included because that could not be accurately tallied.
Recent physical examination revealed a tall rotund boy in no apparent distress. Extraocular muscles were intact; with visual acuity corrected to 20/20 on the right and 20/25 on the left. Pupils were 4 mm and reactive, no afferent pupillary defect is present. An exotropia of 35 prism diopters was noted. There was a mild spastic right hemiparesis. Sensation and proprioception were within normal limits in all major dermatomes tested. This patient ambulated without assistance, with a mildly hemiparetic gait. There were no birthmarks over the craniosacral axis. Papilledema has not been documented although revision of his shunt has in the majority of cases resulted in temporary relief of headache. At the age of 17, he developed a progressively enlarging neck mass in the high cervical region of his shunt tract. A supraclavicular lymph node biopsy confirmed Hodgkin’s lymphoma, which has responded successfully to treatment.
Case 2
This patient initially presented as an infant with intraventricular hemorrhage and had a ventriculoperitoneal shunt placed at 2 months of age. He subsequently underwent 13 ventriculoperitoneal and ventriculoatrial shunt revisions, culminating in a complex bilateral shunt system. A review of his radiology records disclosed a minimum of 14 head CT scans performed prior to the age of 15. He presented to neurosurgery clinic at the age of 19 after a 3 year hiatus from his last shunt revision complaining of morning headaches. His neurologic examination revealed an ambulatory, interactive young man. His cranial nerve examination and fundoscopic examination were normal. He had a partial right homonymous hemianopsia and a subtle right hemiparesis. A CT scan demonstrated a new mass in the left parieto-occipital region, which was subtotally resected. Despite aggressive resection and fractionated cranial irradiation, the gliosarcoma recurred rapidly and the patient expired in home hospice care.
Radiation exposure to cases
Both patients presented in infancy with intraventricular hemorrhage of prematurity and underwent multiple cerebrospinal fluid shunt revisions. Throughout their lives, both patients were plagued with multiple shunt malfunctions necessitating frequent diagnostic imaging and shunt revisions. The first patient underwent a minimum of 23 CT scans of the head, with a cumulative radiation dose estimated at 3,800 mrems. In the first case, Hodgkin’s lymphoma was identified in the soft tissues of the neck surrounding the distally tunneled shunt catheter as an incidental finding. A supraclavicular lymph node biopsy was performed, confirming the diagnosis of Hodgkin’s lymphoma. In the second case, the patient presented to the clinic with headaches and nausea suggestive of shunt malfunction. A head CT, obtained to assess the ventricular system, demonstrated an unexpected mass in the left lateral ventricle and deep parietal lobe. This mass was not present on prior CT images. The mass was subtotally resected. The biopsy demonstrated a highly malignant, poorly differentiated gliosarcoma. Three years prior to the diagnosis of the new mass, this patient had undergone a minimum of 14 CT scans of the head, with a cumulative effective radiation dose estimated at 4,100 mrems. Both patients underwent routine CT imaging of the brain for their shunted hydrocephalus from the time of shunt placement (perinatally) until the present time at routine intervals for clinic visits (approximately every 6 months until age of 5 years then every 1 year). Additionally, each patient underwent CT imaging and radiographs of their shunt systems each time shunt malfunction was evaluated.
Discussion
Calculating the lifetime effective radiation dose that each child received from diagnostic CT imaging is fraught with methodological difficulty due to the long time span (1983–2003) during which the patients underwent imaging, the different CT scanners in use over time (even at the same institutions), and variability in the techniques employed. Furthermore, records from other health care facilities where both of the patients also undoubtedly underwent diagnostic radiological imaging were not available for dose estimation. For the purposes of this study, we have only calculated an estimated effective lifetime dose based on the number of CT scans confirmed to have been performed, assuming the technique used (kmV, etc) was similar to that employed at both institutions in typical adult head CT scans from the 1980s and early 1990s. Newer, age-adjusted techniques are currently employed at the radiology departments at both institutions for diagnostic imaging in all pediatric patients.
While we cannot prove that childhood exposure to CT imaging induced the malignancies in these two cases, it is not unreasonable to suspect a causative role. Both malignancies occurred within the fields exposed to ionizing radiation, and each patient received a cumulative dose of radiation (>4 rem) approximating that seen in the cohort of Hiroshima atomic bomb survivors (5–20 rem) with documented elevated background cancer risks [7, 17, 26, 32, 35]. Many reports exist of malignancies induced in adults from high-dose therapeutic irradiation [3, 9, 16, 18, 24], and it stands to reason that frequent lower doses of ionizing radiation delivered during childhood may also lead to neoplastic transformation. Lifetime cancer mortality risks attributable to pediatric diagnostic radiation exposure are estimated to be considerably higher than in adults. One recent study used population-based estimates of the relative risk of developing a neoplasm from a single diagnostic CT examination to put the odds at 1 in 1,500 per head CT (0.07%) and 1 in 550 per abdominal CT (0.18%) in 1 year olds [3]. By this estimate, the lifetime risk of developing a malignancy increases to 1% after 15 head CT scans early in life.
Physicians and other pediatric health care providers, CT technicians, CT manufacturers, and medical and governmental organizations share the responsibility to minimize radiation exposure to children. Improved communication between radiologists and clinical health care providers regarding the need for CT examination and the techniques used can help minimize radiation exposure. Exposure parameters for pediatric CT should be adjusted based on patient size, the smallest necessary region scanned, and scan resolution (e.g., lower quality scans at lower mA can still be diagnostic). Cranial ultrasound should be used whenever possible in younger patients with open fontanelles. The current medicolegal environment in the US applies pressure to physicians to order tests even when the pretest probability of a positive finding is quite low. When faced with the frequent clinical situation of “rule out shunt failure” in pediatric hydrocephalus patients, emergency room physicians and neurosurgeons should be aware of the potential risks of ionizing radiation from diagnostic imaging. Instead of reflexively ordering the “CT and shunt series,” physicians managing children with hydrocephalus should carefully weigh the real need for imaging data in the clinical decision-making process, tempered against the reality of practicing “defensive medicine.”
Recent reports of the utility of fast-sequence magnetic resonance imaging (MRI) scans to assess the ventricular system for shunt function are encouraging [1, 27, 28]. Advantages of fast-sequence MRI include the lack of ionizing radiation, high resolution imaging of the ventricular system, and usually do not require sedation. The main disadvantages are the difficulty in visualizing the shunt catheters and the availability of time in the MRI unit. Many radiology departments, including our institutions, have made steps to accommodate requests for “rapid sequence shunt MRI” scans by inserting the add-on cases in between longer scheduled studies. Because of the potential risks of pediatric diagnostic CT, “shunt MRI” protocols should be considered for these patients and used whenever possible to minimize exposure to ionizing radiation. Radiation-induced carcinogenesis is most likely due to gene mutations that lead to errors in DNA repair and synthesis [33]. Minimizing patient exposure to radiation with routine radiological tests is desirable with the potential for tissue damage at the molecular level and subsequent risk of cancer.
Conclusions
The clinician should be aware of potential risks while ordering “routine” CT imaging for the evaluation of shunted hydrocephalus. Our hopes are that these case reports enhance the awareness of the readership to this potential problem.
References
Ashley W, Leonard JR, Smyth MD, Ojemann JG, Park TS (2003) Rapid MRI in the evaluation of shunted hydrocephalus. AANS/CNS Joint Section on Pediatric Neurological Surgery, Salt Lake City
Bance M, Guha A (2001) Radiation-induced malignant tumors after stereotactic radiosurgery. Otol Neurotol 22:124–125
Berrington de Gonzalez A, Darby S (2004) Risk of cancer from diagnostic X-rays: estimates for the UK and 14 other countries. Lancet 363:345–351
Boone JM, Geraghty EM, Seibert JA, Wootton-Gorges SL (2003) Dose reduction in pediatric CT: a rational approach. Radiology 228:352–360
Brenner DJ, Elliston CD, Hall EJ, Berdon WE (2001) Estimates of the cancer risks from pediatric CT radiation are not merely theoretical: comment on “point/counterpoint: in x-ray computed tomography, technique factors should be selected appropriate to patient size. against the proposition. Med Phys 28:2387–2388
Brenner D, Elliston C, Hall E, Berdon W (2001) Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol 176:289–296
Brenner DJ (2002) Estimating cancer risks from pediatric CT: going from the qualitative to the quantitative. Pediatr Radiol 32:228–223discussion 242–244
Chan CY, Wong YC, Chau LF, Yu SK, Lau PC (1999) Radiation dose reduction in paediatric cranial CT. Pediatr Radiol 29:770–775
Chang SM, Barker FG 2nd, Larson DA, Bollen AW, Prados MD (1995) Sarcomas subsequent to cranial irradiation. Neurosurgery 36:685–690
Donnelly LF, Emery KH, Brody AS, Laor T, Gylys-Morin VM, Anton CG, Thomas SR, Frush DP (2001) Minimizing radiation dose for pediatric body applications of single-detector helical CT: strategies at a large children's hospital. AJR Am J Roentgenol 176:303–306
Feigal DW Jr (2002) FDA public health notification: reducing radiation risk from computed tomography for pediatric and small adult patients. Int J Trauma Nurs 8:1–2
Frush DP (2003) Responsible use of CT. Radiology 229:289–291
Frush DP (2002) Introduction: the role of the pediatric radiologist in dose reduction. Pediatr Radiol 32:285–286
Ganz JC (2002) Gamma knife radiosurgery and its possible relationship to malignancy: a review. J Neurosurg 97:644–652
Hall EJ (2002) Lessons we have learned from our children: cancer risks from diagnostic radiology. Pediatr Radiol 32:700–706
Hanabusa K, Morikawa A, Murata T, Taki W (2001) Acoustic neuroma with malignant transformation. Case report. J Neurosurg 95:518–521
Hoshi M, Matsuura M, Hayakawa N, Ito C, Kamada N (1996) Estimation of radiation doses for atomic-bomb survivors in the Hiroshima University Registry. Health Phys 70:735–740
Kaido T, Hoshida T, Uranishi R, Akita N, Kotani A, Nishi N, Sakaki T (2001) Radiosurgery-induced brain tumor. Case report. J Neurosurg 95:710–713
Kamel IR, Hernandez RJ, Martin JE, Schlesinger AE, Niklason LT, Guire KE (1994) Radiation dose reduction in CT of the pediatric pelvis. Radiology 190:683–687
Khursheed A, Hillier MC, Shrimpton PC, Wall BF (2002) Influence of patient age on normalized effective doses calculated for CT examinations. Br J Radiol 75:819–830
Land CE (1995) Studies of cancer and radiation dose among atomic bomb survivors. The example of breast cancer. JAMA 274:402–407
Linton OW, Mettler FA Jr (2003) National conference on dose reduction in CT, with an emphasis on pediatric patients. AJR Am J Roentgenol 181:321–329
Little MP, Charles MW (1997) The risk of non-melanoma skin cancer incidence in the Japanese atomic bomb survivors. Int J Radiat Biol 71:589–602
Loeffler JS, Niemierko A, Chapman PH (2003) Second tumors after radiosurgery: tip of the iceberg or a bump in the road? Neurosurgery 52:1436–1440, discussion 1440–1442
Lucaya J, Piqueras J, Garcia-Pena P, Enriquez G, Garcia-Macias M, Sotil J (2000) Low-dose high-resolution CT of the chest in children and young adults: dose, cooperation, artifact incidence, and image quality. AJR Am J Roentgenol 175:985–992
Mabuchi K, Soda M, Ron E, Tokunaga M, Ochikubo S, Sugimoto S, Ikeda T, Terasaki M, Preston DL, Thompson DE (1994) Cancer incidence in atomic bomb survivors. Part I: use of the tumor registries in Hiroshima and Nagasaki for incidence studies. Radiat Res 137:S1–S16
Mannudeep K, Kalra M, Maher T, Toth L, Hamberg M, Blake J, Saini S (2004) Strategies for CT radiation dose optimization. Radiology 230:619–628
Medow JE, Iskandar BJ (2002) “Quick brain” MRI versus CT scan for evaluating shunted hydrocephalus. AANS/CNS Joint Section on Pediatric Neurological Surgery, Scottsdale
Morgan HT (2002) Dose reduction for CT pediatric imaging. Pediatr Radiol 32:724–728, discussion 751–754
Paterson A, Frush DP, Donnelly LF (2001) Helical CT of the body: are settings adjusted for pediatric patients? AJR Am J Roentgenol 176:297–301
Pierce DA, Mendelsohn ML (1999) A model for radiation-related cancer suggested by atomic bomb survivor data. Radiat Res 152:642–654
Preston DL, Ron E, Yonehara S, Kobuke T, Fujii H, Kishikawa M, Tokunaga M, Tokuoka S, Mabuchi K (2002) Tumors of the nervous system and pituitary gland associated with atomic bomb radiation exposure. J Natl Cancer Inst 94:1555–1563
Preston RJ (2004) Radiation biology: concepts for radiation protection. Heatlh Phys 87:3–14
Robinson AE, Hill EP, Harpen MD (1986) Radiation dose reduction in pediatric CT. Pediatr Radiol 16:53–54
Ron E, Preston DL, Kishikawa M, Kobuke T, Iseki M, Tokuoka S, Tokunaga M, Mabuchi K (1998) Skin tumor risk among atomic-bomb survivors in Japan. Cancer Causes Control 9:393–401
Salvati M, Frati A, Russo N, Caroli E, Polli FM, Minniti G, Delfini R (2003) Radiation-induced gliomas: report of 10 cases and review of the literature. Surg Neurol 60:60–67 discussion 67
Shamisa A, Bance M, Nag S, Tator C, Wong S, Noren G, Guha A (2001) Glioblastoma multiforme occurring in a patient treated with gamma knife surgery. Case report and review of the literature. J Neurosurg 94:816–821
Shin M, Ueki K, Kurita H, Kirino T (2002) Malignant transformation of a vestibular schwannoma after gamma knife radiosurgery. Lancet 360:309–310
Yu JS, Yong WH, Wilson D, Black KL (2000) Glioblastoma induction after radiosurgery for meningioma. Lancet 356:1576–1577
Acknowledgements
The authors express their sincere appreciation for the contributions to this manuscript from Drs. Arie Perry (Department of Pathology, Washington University) and Glenn Fletcher (Department of Physics, Washington University).
Author information
Authors and Affiliations
Corresponding author
Additional information
Commentaries on this paper are available at http://dx.doi.org/10.1007/s00381-007-0561-9, http://dx.doi.org/10.1007/s00381-007-0562-8, and http://dx.doi.org/10.1007/s00381-007-0563-7.
Rights and permissions
About this article
Cite this article
Smyth, M.D., Narayan, P., Tubbs, R.S. et al. Cumulative diagnostic radiation exposure in children with ventriculoperitoneal shunts: a review. Childs Nerv Syst 24, 493–497 (2008). https://doi.org/10.1007/s00381-007-0560-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-007-0560-x