
Abstract
Aging plays an essential role in cardiac pathophysiology. Knowledge on the ventricular repolarization in very old individuals is limited. An increase of QT dispersion is associated with higher cardiovascular mortality. The purpose of this study is to investigate whether aging changes the QT dispersion in the very old. Heart rate, P wave duration, PR interval, QRS axis, QRS duration, QT interval, and QTc interval were measured from 12-lead resting ECG. QT dispersion (46 ± 21, 47 ± 17, 69 ± 31 ms, p < 0.005) was significantly increased in the age group ≧85 years (n = 29, 89 ± 4 years) than in the age group 75–84 years (n = 33, 79 ± 3 years) and the age group 65–74 years (n = 32, 68 ± 3 years). Aging modulates dispersion of ventricular repolarization, which may contribute to the cardiac mortality in the very old Asian population.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Aging plays an essential role in cardiac pathophysiology [1]. The incidence of cardiovascular disease, such as coronary artery disease (CAD), heart failure, and valvular diseases, increases with age [2]. Age has been shown to decrease maximal heart rate, beat-to-beat variability, to prolong the PR interval, and to increase the incidence of atrial fibrillation [3–7]. Moreover, aging has also been suggested to prolong the ventricular repolarization measured by QT interval and it may alter the homogeneity of ventricular repolarization [8–10]. QT dispersion reflects nonhomogeneous recovery of excitability or heterogeneity of ventricular repolarization, [11] which is associated with a cardiovascular morbidity and mortality due to electrical instability and ventricular arrhythmogenesis [12–17]. However, knowledge about the effects of aging on QT and QTc dispersions is limited in elderly people. Since the elderly population has increased significantly, it is imperative to evaluate the aging effects of QT dispersion in the very old. The purpose of this study is to investigate the effects of aging on the electrocardiogram in the geriatric population.
Materials and methods
Population selection
This study received institutional review board approval (97038) and enrolled 94 consecutive individuals (46 men and 48 women with a mean age of 78 ± 9 years old) receiving standard 12-lead electrocardiogram (ECG). Twenty-nine (31%) subjects from an outpatient clinic and 65 (69%) subjects from physical checkup were included, whereas the inpatients were excluded to avoid the effects of acute illness. Excluded from the study were subjects without sinus rhythm, those experiencing bundle branch block, those having electrocardiographic evidence of intraventricular conduction abnormalities, those with a QRS interval greater than 100 ms, and those without at least ten evaluable leads with which to measure the QT interval. The subjects were classified into three groups: mild old (65–74 years), moderate old (75–84 years), and very old (≧85 years). Each participant underwent a review of medical history, weight, height, body mass index (BMI, weight in kg/height in m2), blood pressure, and laboratory assessment of fasting sugar, total cholesterol, and triglyceride.
ECG measurements
All patients received a standard 12-lead electrocardiogram recorded at 25 mm/s at outpatient clinic or physical checkup. Heart rate, P wave duration, PR interval, QRS axis, QRS duration, QT interval, and QTc interval were measured. The QT interval was measured in three consecutive cardiac cycles in all leads from the earliest QRS deflection to the end of the T wave and average values are obtained for minimizing error measurements. The QTc was adjusted for heart rate using the Bazett and Fridericia formula [18, 19]. QT dispersion was defined as the maximum interval minus the minimum interval measured on the ECG. T wave end was defined by the threshold method that localizes the T offset as an intercept of the T wave or of its derivative with a threshold above the isoelectric line. Two independent observers were asked to manually analyze the ECG measurements in a blinded fashion. The interobserver reproducibility and intraobserver reproducibility were 91 and 97%, respectively.
Statistical analysis
All data are expressed as mean ± standard deviation. Comparisons among the three groups were analyzed by one-way ANOVA analysis with a post hoc of the Fisher method. Linear regression analysis was used to evaluate the correlation between the age, QT dispersion, and QTc dispersion. A p valve <0.05 was considered statistically significant.
Results
Gender, body weight, height, blood pressure, incidences of hypertension, diabetes, smoking, and dyslipidemia were similar among the three groups (Table 1). Figure 1 shows the ECG examples from the three groups. The age group ≧85 years has a larger QT dispersion and QTc dispersion than the other two age groups (Fig. 2a). In addition, there was a positive relationship between QT dispersion or QTc dispersion and age (Fig. 2b).

Examples of QT dispersion and QTc dispersion from different age subjects. a Age between 65 and 74 years, QT dispersion (50 ms), and QTc dispersion (54 ms). b Age between 75 and 84 years, QT dispersion (40 ms), and QTc dispersion of (43 ms). c Age more than 85 years, QT dispersion (60 ms), and QTc dispersion (61 ms)

Distributions of QT and QTc dispersion in different age groups. a QT and QTc dispersion increased in the very old age group. b Linear regression shows a good relationship between QT dispersion or QTc dispersion and age
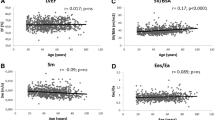
Figure 3 shows the heart rate, PR interval, QRS axis, QRS duration, QT, and QTc interval in the three groups. The QRS axis, QRS duration, QT interval, and QTc interval were similar among these patients. However, the age group 75–84 years or ≧85 years has a longer PR interval than the age group 65–74 years. In contrast, resting heart rate was faster in the age group ≧85 years than in the other two age groups. Figure 4 shows the correlations between heart rate or PR interval and age.

Distribution of heart rate, PR interval, QRS axis, QRS duration, QT interval, and QTc interval in different age groups. Resting heart rate was faster and PR interval was longer in the very old age group

Linear regression shows a relationship between resting heart rate or PR interval and age
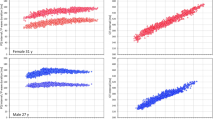
Among female individuals, the female age group ≧85 years has a larger QT dispersion and QTc dispersion than the other two female groups (Fig. 5). In contrast, the QT dispersion and QTc dispersion were similar among the three male age groups. Figure 5b shows a good correlation between QT dispersions or QTc dispersions and age in female population. Moreover, the QT interval was similar among female age groups 65–74 years, 75–84 years, and ≧85 years (420 ± 38, 417 ± 39, 429 ± 68 ms, p > 0.05) and male age groups (401 ± 30, 394 ± 27, 399 ± 31 ms, p > 0.05).

Gender differences in aging effects. a QT dispersion and QTc dispersion in male and female individuals from different age groups. b Linear regression showed a good relationship between QT dispersion or QTc dispersion and age in male and female groups
Table 2 shows the baseline characteristics and ventricular repolarization in hypertensive and non-hypertensive patients. The hypertensive patients have a high incidence of dyslipidemia and use of aspirin. In the patients with hypertension, the age group ≧85 years has a larger QT dispersion and QTc dispersion than the other two hypertensive groups (Fig. 6). In contrast, the QT dispersion and QTc dispersion were similar among the three non-hypertensive groups. Figure 6b shows a good correlation between QT dispersion or QTc dispersion and age in patients with hypertension. Moreover, the QT interval was similar among the hypertensive age groups 65–74 years, 75–84 years, and ≧85 years (419 ± 47, 406 ± 37, 408 ± 54 ms, p > 0.05) and non-hypertensive groups (410 ± 25, 405 ± 33, 413 ± 44 ms, p > 0.05).

Differences of hypertension in aging effects. a QT dispersion and QTc dispersion in hypertensive and non-hypertensive individuals from different age groups. b Linear regression showed a good relationship between QT dispersion or QTc dispersion and age in hypertension and non-hypertension groups
Discussion
The main finding of this study is that QT dispersion and QTc dispersion are significantly increased in the very old (≧85 years) population. In addition, hypertension and female gender appear to play important roles in aging-related increases of QT dispersions.
QT interval dispersion, defined as the difference between the longest and the shortest QT interval as measured by 12-lead electrocardiogram, was proposed as an electric instability index to represent the expression of regional physiological variation of myocardial excitability recovery [20]. QT dispersion has been proposed to identify those patients who are at risk of developing ventricular arrhythmias and reported to be associated with sudden cardiac death [12–16]. Previous study from Reardon et al. [8] has shown that QT dispersion was similar between subjects younger and older than 75 years of age. This study also shows a similar QT dispersion and QTc dispersion between age groups 65–74 years and 75–84 years. However, for the first time, this study shows that QT dispersion and QTc dispersion are significantly increased in the very old (≧85 years) population. These findings may have a role in the cardiac mortality in the very old individuals. Although previous study has revealed that QT interval was increased with age [8, 9], we have found a similar QT interval among the patients. Since the use of diuretics may induce hypokalemia to interfere with QT interval, we also compared the QT interval without including the data from the patients using diuretics. The QT interval was still similar among different age groups. The conflicting results may be due to racial differences, since all the subjects in this study were Asians. In addition, the included patients were older and the gender was balanced. Hansen et al. [21] has shown that sex may not affect the QT dispersion. However, there was increased QT dispersion in the very old female group in this study, which suggests a gender difference of aging effects on ventricular repolarizations. Moreover, heart failure has been shown to increase QT dispersion [22]. In this study, each age group contains one patient with chronic heart failure. We further evaluated the QT dispersion among the patients without heart failure and found that QT dispersion was still significantly different among the three age groups.
Previous study has shown that hypertension plays a role in QT dispersions [23]. Recent studies have evaluated the significance of QT dispersion in elderly hypertensive and normotensive patients and found a significant prognostic value in these patients [24, 25]. In this study, we found that very old patients with hypertension had larger QT dispersion as compared to other hypertensive groups. In contrast, the QT dispersion was similar among the different groups of non-hypertensive individuals. These findings suggest the important role of hypertension in QT dispersion and also indicate the potential role of cardiac mortality of hypertension with aging. In this study, PR interval prolongs with aging and this finding corresponds with previous study [6]. The prolongation of the PR interval indicates delayed conduction of AV node.
Aging has been shown to decrease maximum heart rates [5]. Interestingly, we have found that resting heart rates were increased in the very old age group, which was evident in total patients or in the male or female population. The resting heart rates were still higher in the very old group after excluding the patients with heart failure. These findings suggest the possibility that parasympathetic tone in very old people is significantly reduced. Reduced parasympathetic tone is associated with increased cardiac mortality [26–28]. This phenomenon may play a role in cardiac death in the elderly.
Study limitations
The data should be interpreted with caution due to the potential limitations. Although there was no statistical difference regarding QT-dispersion and QTc-dispersion among the three male groups or among three non-hypertensive groups, there was a trend for the group ≧85 years to have higher values. This can be explained by the small number of patients included in each group. However, the significant differences among these age groups suggest the importance of age on ventricular repolarization. Additionally, the possible comorbidities in our patients may interfere with our findings. It is well known that the prevalence of heart failure increases with age [29]. Nonetheless, the very old age group only contains one patient with heart failure in this study. It is possible that the use of diuretics in this group of patients may indicate the presence of heart failure.
Conclusions
Our results show that aging modulates the dispersion of ventricular repolarization, which may contribute to the cardiac mortality in the very elderly population in Asian population.
References
Centers for Disease Control, Prevention (CDC) (2003) Trends in aging––United States and worldwide. MMWR Morb Mortal Wkly Rep 52:101–104 (see also pp 106)
Lakatta EG, Levy D (2003) Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “Set Up” for vascular disease. Circulation 107:139–146
Wolf PA, Mitchell JB, Baker CS, Kannel WB, D’Agostino RB (1998) Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med 158:229–234
Psaty BM, Manolio TA, Kuller LH, Kronmal RA, Cushman M, Fried LP, White R, Furberg CD, Rautaharju PM (1997) Incidence of and risk factors for atrial fibrillation in older adults. Circulation 96:2455–2461
Fleg JL, O`Connor F, Gerstenblith G, Becker LC, Clulow J, Schulman SP, Lakatta EG (1995) Impact of age on the cardiovascular response to dynamic upright exercise in healthy men and women. J Appl Physiol 78:890–900
Fleg JL, Das DN, Wright J, Lakatta EG (1990) Age-associated changes in the components of atrioventricular conduction in apparently healthy volunteers. J Gerontol 45:M95–M100
Taneja T, Mahnert BW, Passman R, Goldberger J, Kadish A (2001) Effects of sex and age on electrocardiographic and cardiac electrophysiological properties in adults. Pacing Clin Electrophysiol 24:16–21
Reardon M, Malik M (1996) QT interval change with age in an overtly healthy older population. Clin Cardiol 19:949–952
Esen AM, Barutcu I, Melek M, Kaya D, Onrat E, Batukan Esen O (2004) Comparison of QT interval duration and dispersion in elderly population versus healthy young subjects. Clin Auton Res 4:408–411
Su HM, Chiu HC, Lin TH, Voon WC, Liu HW, Lai WT (2006) Longitudinal study of the ageing trends QT interval and dispersion in healthy elderly subjects. Age Ageing 35:636–638
Franz MR, Zabel M (2000) Electrophysiological basis of QT dispersion measurements. Prog Cardiovasc Dis 42:311–324
Day CP, McComb JM, Campbell RW (1990) QT dispersion: an indication of arrhythmia risk in patients with long QT intervals. Br Heart J 63:342–344
Elming H, Holm E, Jun L, Torp-Pedersen C, Køber L, Kircshoff M, Malik M, Camm J (1998) The prognostic value of the QT interval and QT interval dispersion in all-cause and cardiac mortality and morbidity in a population in all-cause and cardiac mortality and morbidity in a population of Danish citizens. Eur Heart J 19:1391–1400
Zareba W, Moss AJ, le Cessie S (1994) Dispersion of ventricular repolarization and arrhythmic cardiac death in coronary artery disease. Am J Cardiol 74:550–553
de Bruyne MC, Hoes AW, Kors JA, Hofman A, van Bemmel JH, Grobbee DE (1998) QTc dispersion predicts cardiac mortality in the elderly: the Rotterdam Study. Circulation 98:467–472
Barr CS, Naas A, Freeman M, Lang CC, Struthers AD (1994) QT dispersion and sudden unexpected death in chronic heart failure. Lancet 343:327–329
Hina K, Kawamura H, Murakami T, Yamamoto K, Yamaji H, Murakami M, Hirohata S, Ogawa H, Sakane K, Kusachi S (2008) Association of corrected QT dispersion with symptoms improvement in patients receiving cardiac resynchronization therapy. Heart Vessels 23:325–333
Malik M, Batchvarov VN (2000) Measurement, interpretation and clinical potential of QT dispersion. J Am Coll Cardiol 36:1749–1766
Pan NH, Yang HY, Hsieh MH, Chen YJ (2008) Coronary calcium score from multislice computed tomography correlates with QT dispersion and left ventricular wall thickness. Heart Vessels 23:155–160
Merri M, Benhorin J, Alberti M, Locati E, Moss AJ (1989) Electrocardiographic quantitation of ventricular repolarization. Circulation 80:1301–1308
Hansen S, Rasmussen V, Larsen K, Torp-Pedersen C, Jensen GB (2007) Circadian variation in QT dispersion determined from a 12-lead Holter recording: a methodological study of an age- and sex-stratified group of healthy subjects. Ann Noninvasive Electrocardiol 12:185–196
Kuch M, Janiszewski M, Mamcarz A, Cudnoch-Jedrzejewska A, Dłuzniewski M (2009) Major adverse cardiac event predictors in survivors of myocardial infarction with asymptomatic left ventricular dysfunction or chronic heart failure. Med Sci Monit 15:40–48
Clarkson PB, Naas AA, McMahon A, MacLeod C, Struthers AD, MacDonald TM (1995) QT dispersion in essential hypertension. QJM 88:327–332 (See also pp 322)
Dimopoulos S, Nicosia F, Donati P, Prometti P, De Vecchi M, Zulli R, Grassi V (2008) QT-dispersion and left ventricular hypertrophy in elderly hypertensive and normotensive patients. Angiology 59:605–612
Dimopoulos S, Nicosia F, Turini D, Zulli R (2009) Prognostic evaluation of QT-dispersion in elderly hypertensive and normotensive patients. Pacing Clin Electrophysiol 32:1381–1387
Hull SS Jr, Evans AR, Vanoli E, Adamson PB, Stramba-Badiale M, Albert DE, Foreman RD, Schwartz PJ (1990) Heart rate variability before and after myocardial infarction in conscious dogs at high and low risk of sudden death. J Am Coll Cardiol 16:978–985
Kleiger RE, Miller JP, Bigger JT Jr, Moss AJ (1987) Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol 59:256–262
Ishida S, Nakagawa M, Fujino T, Yonemochi H, Saikawa T, Ito M (1997) Circadian variation of QT interval dispersion: correlation with heart rate variability. J Electrocardiol 30:205–210
Ho KK, Pinsky JL, Kannel WB, Levy D (1993) The epidemiology of heart failure: the Framingham Study. J Am Coll Cardiol 22:6A–13A
Acknowledgments
This work was supported by the Center of Excellence for Clinical Trial and Research in Neuroscience (DOH99-TD-B-111-003) and grants NSC 96-2628-B-038-012-MY3, NSC 96-2314-B-010-006, NSC 97-2314-B-038-030-MY3.
Conflict of interest
The authors have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Huang, JH., Lin, YQ., Pan, NH. et al. Aging modulates dispersion of ventricular repolarization in the very old of the geriatric population. Heart Vessels 25, 500–508 (2010). https://doi.org/10.1007/s00380-010-0026-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-010-0026-z