
Abstract
Purpose
Higher chronological age has been suggested to confer worse prognosis in patients with upper tract urothelial carcinoma (UTUC). The aim of the current study was to test this hypothesis in a large multicenter external validation cohort of patients treated with radical nephroureterectomy (RNU) while controlling for patient performance status.
Materials and methods
We retrospectively reviewed the data from 1,169 patients treated with RNU for UTUC. Age at RNU was analyzed both as a continuous and categorical variable (<50 years, n = 66; 50–59.9 years, n = 185; 60–69.9 years, n = 367; 70–79.9 years, n = 419; ≥80 years, n = 132). Median follow-up was 37 months.
Results
Actuarial recurrence-free, cancer-specific, and all-cause survival estimates at 5 years after RNU were 69, 73, and 61%, respectively. Advanced age was associated with female gender, higher ECOG status, higher ASA score, and a lower probability of receiving adjuvant chemotherapy (all P values ≤ 0.02). In multivariable analyses, advanced age was associated with decreased recurrence-free (P = 0.021), cancer-specific (P = 0.002), and all-cause survival (P < 0.001) after controlling for the effects of gender, tumor location, number of lymph nodes removed, tumor grade, stage, architecture, necrosis, and lymphovascular invasion. After addition of ECOG status, age remained an independent predictor of only all-cause mortality (P > 0.001).
Conclusions
We confirmed that advanced patient age at the time of RNU is associated with worse clinical outcomes after surgery. However, ECOG performance status abrogated the association. Furthermore, a large proportion of elderly patients were cured with RNU. This suggests that chronological age alone is an inadequate indicator criterion to predict response of older UTUC patients to RNU.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Radical nephroureterectomy (RNU) is the gold standard treatment for high-risk upper tract urothelial carcinoma (UTUC) [1]. Improvements in perioperative care and refinements of surgical technique have made this a safe and feasible operation for an increasing number of patients [2]. However, the effectiveness and relative use of RNU in the subgroup of older patients remains controversial. Being older at the time of RNU has been shown to be associated with decreased survival [3]. Potential hypotheses to explain this finding include changes in the biological potential of the tumor, a decrease in the host’s defense mechanisms, or differences in care patterns in elderly patients [3]. As in bladder cancer, older patients might deny the opportunity to receive the most effective treatment for their disease on the basis of chronological age alone [4, 5]. In this context, we evaluated the association of patient age with pathologic and long-term oncologic outcomes in a large international cohort of patients treated with RNU for UTUC while adjusting for the effect of ECOG performance status. Moreover, we estimated the probability of experiencing disease recurrence or dying of UTUC within different age groups.
Materials and methods
Patient selection
This study consists of data collected from 11 participating sites from the Upper Tract Urothelial Carcinoma Collaboration (UTUCC) validation cohort. None of the data from these patients were included in our previous study [3]. All centers provided the necessary institutional data sharing agreements before study initiation. The institutional review board at each site approved this study. The database was comprised of 1,169 patients who underwent RNU with ipsilateral bladder cuff resection by multiple surgeons between 1987 and 2009. RNU that was performed by several surgeons included an extrafascial dissection of the kidney with the entire length of ureter and adjacent segment of the bladder cuff. The hilar and regional lymph nodes adjacent to the ipsilateral great vessel generally were resected along with enlarged lymph nodes if abnormal on preoperative computed tomography scans or palpable intraoperatively. Extended lymphadenectomy was not routinely performed. None of the patients received preoperative chemotherapy or radiation therapy. None of the patients had invasive bladder cancer before their RNU. The Eastern Cooperative Oncology Group (ECOG) performance status was available in 551 patients prior to RNU [6]. Before final analysis, the database was frozen and the final data set was produced for current analysis.
Pathological evaluation
All surgical specimens were processed according to standard pathological procedures, and all slides were reviewed by genitourinary pathologists blinded to clinical outcomes. Tumors were staged according to the TNM classification by the American Joint Committee on Cancer/International Union Against Cancer. Tumor grading was assessed according to the 1998 WHO/International Society of Urologic Pathology consensus classification [7]. Tumor architecture was defined as papillary or sessile. Tumor location was defined as pelvic/caliceal or ureteral. In tumors involving both sites, the location was attributed according to the index cancer. LVI was defined as the unequivocal presence of tumor cells within an endothelium-lined space, with no underlying muscular walls [8].
Follow-up regimen
Patients were generally evaluated every 3–4 months for the first year after surgery, every 6 months from the second through fifth years, and annually thereafter. Follow-up consisted of a history and physical examination, serum chemistry studies, urinary cytology, chest radiography, cystoscopy, and radiographic evaluation of the contralateral upper urinary tract.
Disease recurrence was defined as local failure in the operative site, regional lymph nodes, or distant metastasis. A recurrence in the bladder was not calculated in the recurrence-free survival analysis. The cause of death was determined by retrospective chart review and corroborated by death certificates. A patient with widely disseminated metastases at the time of death was categorized as having died of UTUC. Patients who died within 30 days of surgery were censored at the time of death for UTUC-specific survival analysis.
Statistical analysis
Fisher’s exact and chi-square (χ2) tests were used to evaluate the association between categorical variables. Differences in continuous variables across categorical variables were analyzed using the Mann–Whitney U or Kruskal–Wallis test, respectively. Univariate and multivariable Cox regression models were used to evaluate time to recurrence, cancer-specific, and all-cause mortality outcomes. Statistical significance was defined as P ≤ 0.05. All reported P values were two-sided. Analyses were performed with SPSS® 17 (SPSS, Inc., Chicago, IL).
Results
Association of age as continuous and categorical variables with clinical and pathologic characteristics
The median patient age was 69 years. At the time of RNU, 66 (5.6%), 185 (15.8%), 367 (31.4%), 419 (35.8%), and 132 (11.3%) patients were younger than 50, between 50 and 59.9, between 60 and 69.9, between 70 and 79.9, and older than 80 years old, respectively. The association of age at RNU with clinicopathologic characteristics is shown in Table 1. Higher age was significantly associated with a history of previous bladder cancer (P < 0.017), tumor location (P = 0.035), worse ECOG performance status (P < 0.0001), higher American Society of Anesthesiologists (ASA) Score (P = 0.001), and female gender (P < 0.001). Adjuvant chemotherapy was given more commonly to younger patients (P ≤ 0.018).
Association of age as continuous and categorical variables with disease outcomes
The mean follow-up was 38 months (median: 37 months; range: 1–195 months, interquartile range: 39) for patients alive at last follow-up. Actuarial recurrence-free estimates at 2, 5, and 10 years after RNU were 75% (standard error [SE] ± 1), 69% (±2), and 65% (±2), respectively. Actuarial cancer-specific survival estimates at 2, 5, and 10 years after RNU were 82% (±1), 73% (±2), and 65% (±3), respectively. Actuarial all-cause survival estimates at 2, 5, and 10 years after RNU were 77% (±1), 61% (±2), and 34% (±3), respectively. In univariate analyses, age coded as either a continuous or categorical variable was significantly associated with disease recurrence (P values ≤ 0.05), cancer-specific mortality (P values < 0.009), and all-cause mortality (P values < 0.0001).
In multivariable analyses (Table 2), age coded as a categorical variable was an independent predictor of disease recurrence (P = 0.018), cancer-specific mortality (P = 0.001), and all-cause mortality (P < 0.001). Patients 70 years and older were at increased risk for disease recurrence and patients 60 years and older were at increased risk for cancer-specific and all-cause mortality. The same was true for age when analyzed as continuous variable (P = 0.021, P = 0.002, and P < 0.001, respectively). Subgroup analyses in patients who did not undergo adjuvant chemotherapy did not change the statistical significance of these associations.
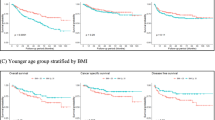
Figure 1a shows the proportion of patients who experienced disease recurrence at 3 years after RNU, stratified by age in decades. Patients who were censored before 2 years were excluded from the analysis to prevent underestimation of the recurrence probability. The proportion of patients who experienced disease recurrence by 3 years increased incrementally with advancing age. The probability of disease recurrence at 3 years following RNU was 22.4% for patients under 50 years of age compared to 40.2% for patients over 80 years of age.

a Proportion of patients with disease recurrence at 3 years after radical nephroureterectomy (standard error bars shown). b Proportion of patients with cancer-specific mortality at 5 years after radical nephroureterectomy (standard error bars shown)
Figure 1b shows the proportion of patients who died from UTUC at 5 years after RNU, stratified by age in decades. Patients who were censored before 2 years were excluded from the analysis to prevent underestimation of the survival probability. The proportion of patients who died from UTUC by 5 years increased incrementally with advancing age. The probability of cancer-specific death at 5 years following RNU was 14.3% for patients under 50 years of age compared to 32.2% for patients over 80 years of age.
Overall, 551 patients had ECOG performance status available. These patients were more likely to be of male gender (P < 0.001), have tumor located in the renal pelvis (P = 0.04), undergo laparoscopic RNU (P < 0.001), receive adjuvant chemotherapy (P = 0.03), have papillary tumor architecture (P < 0.001), and less likely to have previous bladder cancer (P = 0.01).
When ECOG performance status was added to the multivariable models (Table 3; n = 551), age was only associated with all-cause death (P < 0.0001), but not with disease recurrence (P = 0.766) or cancer-specific death (P = 0.357). ECOG performance status was independently associated with all-cause death (HR 1.58, P = 0.005), but not with disease recurrence (HR 1.38, P = 0.101) or cancer-specific death (HR 1.27, P = 0.287).
Discussion
In the present study, we confirmed that chronological age coded either as a continuous or a categorical variable was significantly associated with post-RNU clinical outcomes [3] after adjusting for the effect of standard clinical and pathologic covariates. However, when adjusted for the effects of ECOG performance status, age was not associated with clinical outcomes. Moreover, the large majority of oldest elderly (defined as age over 80 years) patients did not experience disease recurrence and death. We confirmed that higher chronological age was associated with increased risk of disease recurrence and mortality after RNU [3]. Similarly, mortality from urothelial carcinoma of the bladder has been shown to be higher in the elderly [9]. The ratio of cancer-specific mortality to incidence for patients in the USA aged 65–69 years is 14 and 18%, respectively, whereas for patients aged 80–84 years, it is 30 and 37%, respectively [10]. The higher mortality in the elderly has several possible explanations. In patients aged <40 years, bladder cancer tends to be well differentiated and therefore behaves in a more indolent fashion [11–13]. While some researchers have observed lower rates of disease recurrence and progression with better survival in younger patients [9, 11–17], others have reported that the natural history of bladder cancer in younger patients resembles that of older patients [18–22]. Differences in outcomes between the elderly and their younger counterparts might be due to a combination of relatively more advanced stage at diagnosis (due to social and/or biological reasons [4]) and the administration of less aggressive and potentially more effective therapies in the elderly.
We found that elderly patients were less likely to undergo lymphadenectomy, receive adjuvant chemotherapy, and were more likely to have previous bladder cancer. One reason for this tendency may be decreased renal function among elderly patients. In general, elderly patients with multiple comorbidities are less likely to be candidates for the most aggressive chemotherapy combinations because of a high risk of significant treatment-related morbidity [4]. We and others have previously shown that lymphadenectomy is potentially curative in patients with tumor burden and that nodal status is a significant predictor of cancer-specific survival in UTUC [23]. Therefore, even elderly patients expected to have pT2–4 disease should undergo lymphadenectomy to improve staging and having the chance of cure.
Another reason for worse outcomes in patients with advanced age compared with their younger counterparts may be the reluctance to perform radical surgery in older patients with comorbidities [9, 24]. Delay of radical treatment has been shown to result in stage progression and worse survival in patients with UTUC and bladder cancer [25, 26]. Timely consideration of definitive treatment for patients with high-risk UTUC seems to be of high importance, especially in elderly patients [27].
The association of age with worse outcomes is likely due to worse performance status and higher comorbidities in elderly patients. Adjustment for the effect of ECOG mitigated the prognostic value of age. This, together with the finding that many elderly patients did well after RNU, suggests that it is not chronological age but biological age that determines outcomes after RNU.
There are several limitations in this study. First and foremost are the limitations inherent to retrospective analyses. We are unable to comment on the extent to which patient age factored into the selection of RNU and/or perioperative chemotherapy among available treatment options for patients. The impact of an age-based selection bias on treatment outcomes for UTUC is probably substantial, particularly given the suspected relative underuse of RNU for elderly patients. The relative underuse of chemotherapy in older patients in the present series suggests a bias against adjuvant treatment in our older patients; however, the individual reasons for this were not available. A careful analysis of other factors not addressed in the present study, such as the time from invasive UTUC diagnosis to RNU and the impact of comorbidities, is needed to have a better understanding of the effect of age on tumor biology and patient survival. We did not adjust for comorbidities, which would have been a better measure of patient health than ECOG performance status. Such data have not been systematically examined and may add to the perspective of quality-of-life-adjusted relative survival benefits.
Another limitation is the inherent difficulty in determining the presence of LVI at the morphological level, with significant differences between local pathologists and central pathology review [28, 29]. For example, retraction artefacts of the surrounding stromal tissue can mimic vascular invasion [30, 31]. Therefore, experts have recommended reporting LVI only in unequivocal cases and to make use of immunohistochemistry if necessary [30, 31]. However, the use of immunohistochemical staining to identify the vessels remains controversial (e.g., heterogeneity in the expression of immunohistochemical markers by different capillary structures) and not practical for everyday clinical use [32, 33].
Conclusions
While age was associated with disease recurrence and decreased survival after RNU, advanced age should not be an exclusion criterion for the aggressive treatment of potentially curable UTUC. Reluctance to perform radical treatment, decreased performance of lymphadenectomy, and underuse of adjuvant chemotherapy are potentially modifiable risk factors that could lead to improvement of outcomes in elderly patients. Further research on the epigenetic and genetic changes that occur with aging may shed light on the association of age with biologic behavior.
Abbreviations
- ASA:
-
American Society of Anesthesiologists Physical Status Classification System
- ECOG:
-
Eastern Cooperative Oncology Group
- RNU:
-
Radical nephroureterectomy
- UTUC:
-
Upper tract urothelial carcinoma
- UTUCC:
-
Upper Tract Urothelial Carcinoma Collaboration
References
Scher H et al. (1998) NCCN urothelial cancer practice guidelines. National Comprehensive Cancer Network. Oncology (Williston Park) 12(7A):225–271
Sun M et al (2010) Management of upper urinary tract urothelial carcinoma. Expert Rev Anticancer Ther 10(12):1955–1965
Shariat S et al (2010) Advanced patient age is associated with inferior cancer-specific survival after radical nephroureterectomy. BJU Int 105(12):1672–1677
Shariat SF, Milowsky M, Droller MJ (2009) Bladder cancer in the elderly. Urol Oncol 27(6):653–667
Nielsen M et al. (2007) Advanced age is associated with poorer bladder cancer-specific survival in patients treated with radical cystectomy. Eur Urol 51(3):699–706 (discussion 706–708)
Oken MM et al (1982) Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 5(6):649–655
Epstein JI (1998) The World Health Organization/International society of urological pathology consensus classification of urothelial (transitional cell) neoplasms of the urinary bladder. Bladder consensus conference committee. Am J Surg Pathol 22(12):1435–1448
Shariat SF et al (2010) International validation of the prognostic value of lymphovascular invasion in patients treated with radical cystectomy. BJU Int 105(10):1402–1412
Nielsen ME et al. (2007) Advanced age is associated with poorer bladder cancer-specific survival in patients treated with radical cystectomy. Eur Urol 51(3):699–706(discussion 706–708)
EM M (2008) Urothelial tumors of the bladder. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA (eds) Campbell-Walsh urology. Saunders-Elsevier, Philadeiphia, Amsterdam, pp 2407–2446
Benson RJ, Tomera K, Kelalis P (1983) Transitional cell carcinoma of the bladder in children and adolescents. J Urol 130(1):54–55
Fitzpatrick J, Reda M (1986) Bladder carcinoma in patients 40 years old or less. J Urol 135(1):53–54
Linn J et al (1998) The molecular characteristics of bladder cancer in young patients. J Urol 159(5):1493–1496
Madgar I et al (1988) Long-term followup of patients less than 30 years old with transitional cell carcinoma of bladder. J Urol 139(5):933–934
Witjes J, Debruyne F (1989) Bladder carcinoma in patients less than 40 years of age. Urol Int 44(2):81–83
Resorlu B et al (2009) The prognostic significance of advanced age in patients with bladder cancer treated with radical cystectomy. BJU Int 103(4):480–483
Shi B et al (2008) Relationship between patient age and superficial transitional cell carcinoma characteristics. Urology 71(6):1186–1190
Johnson D, Hillis S (1978) Carcinoma of the bladder in patients less than 40 years old. J Urol 120(2):172–173
Kurz K, Pitts W, Vaughan EJ (1987) The natural history of patients less than 40 years old with bladder tumors. J Urol 137(3):395–397
Kutarski P, Padwell A (1993) Transitional cell carcinoma of the bladder in young adults. Br J Urol 72(5 Pt 2):749–755
Wan J, Grossman H (1989) Bladder carcinoma in patients age 40 years or younger. Cancer 64(1):178–181
Yossepowitch O, Dalbagni G (2002) Transitional cell carcinoma of the bladder in young adults: presentation, natural history and outcome. J Urol 168(1):61–66
Roscigno M et al (2009) Impact of lymph node dissection on cancer specific survival in patients with upper tract urothelial carcinoma treated with radical nephroureterectomy. J Urol 181(6):2482–2489
Prout GR Jr (2005) Age and comorbidity impact surgical therapy in older bladder carcinoma patients: a population-based study. Cancer 104(8):1638–1647
Nielsen M et al (2007) A delay in radical cystectomy of >3 months is not associated with a worse clinical outcome. BJU Int 100(5):1015–1020
Gore J et al (2009) Mortality increases when radical cystectomy is delayed more than 12 weeks: results from a surveillance, epidemiology, and end results-medicare analysis. Cancer 115(5):988–996
Waldert M et al (2010) A delay in radical nephroureterectomy can lead to upstaging. BJU Int 105(6):812–817
Sesterhenn IA et al (1992) Prognosis and other clinical correlates of pathologic review in stage I and II testicular carcinoma: a report from the Testicular Cancer Intergroup Study. J Clin Oncol 10(1):69–78
Cheng L et al (2005) Lymphovascular invasion is an independent prognostic factor in prostatic adenocarcinoma. J Urol 174(6):2181–2185
Lapham RL, Grignon D, Ro JY (1997) Pathologic prognostic parameters in bladder urothelial biopsy, transurethral resection, and cystectomy specimens. Semin Diagn Pathol 14(2):109–122
Larsen MP et al (1990) Use of Ulex europaeus agglutinin I (UEAI) to distinguish vascular and “pseudovascular” invasion in transitional cell carcinoma of bladder with lamina propria invasion. Mod Pathol 3(1):83–88
Miyata Y et al (2006) Tumor lymphangiogenesis in transitional cell carcinoma of the upper urinary tract: association with clinicopathological features and prognosis. J Urol 176(1):348–353
Straume O, Jackson DG, Akslen LA (2003) Independent prognostic impact of lymphatic vessel density and presence of low-grade lymphangiogenesis in cutaneous melanoma. Clin Cancer Res 9(1):250–256
Conflicts of Interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chromecki, T.F., Ehdaie, B., Novara, G. et al. Chronological age is not an independent predictor of clinical outcomes after radical nephroureterectomy. World J Urol 29, 473–480 (2011). https://doi.org/10.1007/s00345-011-0677-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-011-0677-0