
Abstract
The aim of this paper is to study the variations in the percentage of the different types of renal stones with age and sex. Renal calculi were classified according to their composition and structure. Stone formers were divided according to age and sex, and the percentage of each kind of calculi in the different considered age periods for men and women were determined. It was found that calcium oxalate dihydrate calculi decreased with age, but only in men. These calculi were also clearly predominant in men. Hydroxyapatite calculi decreased with age in both men and women, but they were predominant in women. Uric acid calculi increased with age in both men and women, but were predominant in men. Finally, it was found that calcium oxalate monohydrate unattached calculi increased with age in both men and women. As a main novelty, the study here presented demonstrates the importance of distinguishing between calcium oxalate monohydrate papillary stones and calcium oxalate monohydrate unattached stones, since the etiologic factors responsible for their origin must be clearly different.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Urinary tract stone disease is an unfortunately frequent event that affects the population in all countries. Nevertheless, the overall probability of forming stones considerably differs in various parts of the world [1, 2]. Likewise, in Asia it affects between 1 and 5% of the population, 5 and 10% in Europe and 13% in North America. In fact, socio-economical conditions have generated changes in the incidence and type of renal lithiasis (location, composition and structure of the calculi) [3], and this must be attributed to the different lifestyle and dietetic habits. Due to the continuous changes in these last aspects, the relationships between frequency, age, sex and composition can also change with time. Thus, in a study with 15,624 renal stones from 1979 to 1998 in Canada, it was found that from the first (1980–1983) to the last (1995–1998) complete 4-year periods, there was a relative increase in oxalate and decrease in phosphate stones, associated with increasing age from decades 5 to 6 for oxalate and phosphate stones, except that the age peak for phosphate stones in women remained in decade 3 [4]. In a study developed in USA during a period of 14 years (1989–2003), a significant increase of calcium oxalate monohydrate (COM), brushite and uric acid renal calculi was found [5]. This study also found that the percentage occurrence of calcium oxalate stones decreased, while that of calcium phosphate stones increased with each new stone event [5]. A recent study of Daudon et al. [6] analyzes the changes in stone composition according to age and gender of patients in France. This study points out the increasing contribution of uric acid stones with age in both genders and the preponderance of phosphate stones in females. In the present paper, variations in the percentage of each type of stone with age and sex were studied and possible relation with etiologic factors was investigated to explain the observed changes.
Methods
Patients
The study included 2,453 renal calculi produced during the period 1988–2004. The patients were divided according to age and sex in eleven groups that appear in Table 1. As can be observed, five age groups were considered: 10–35, 36–44, 45–53, 54–63 and 64–92 years. The age intervals were chosen to obtain homogeneous size groups. Each lithiasic episode was considered as a new case.
For each renal calculi type, percentage of that kind of calculi in the different considered age groups for men and women and the male/female sex ratio were determined.
Child lithiasis (10–18 years) was not considered as a separate group due to the low number of cases (n = 18, considering all calculi types and both sexes). Struvite calculi were not considered due to their infectious origin. Brushite, cystine and infrequent renal calculi were not included in the study due to the limited number of these types of calculi (n = 182, considering the four types of calculi (see Table 1)).
Urinary calculi studies
The 2,453 renal calculi were collected, dried, stored in sterile containers and studied immediately. The calculus was obtained intact when it came out by spontaneous passage, or fragmented when it was retrieved by ureterorenoscopy, percutaneous nephrolithotomy or shock wave lithotripsy. The procedure used to analyze and study renal calculi involved an appropriate combination of observation by means of macroscopic and microscopic conventional techniques (stereoscopic microscope Optomic) together with physical techniques such as infrared (IR) spectrometry (Brucker IFS 66 infrared spectroscope) and scanning electron microscopy (SEM) (Hitachi S−530) coupled with X ray microanalysis (Oxford Link Isis) [7].
The study of the calculus begins with direct observation of its external aspect using a stereoscopic microscope. The calculus is then sectioned into two parts along a plane as close as possible to its geometric center in order to establish the internal structure. When the calculus is supplied in a fragmented form, all fragments are observed by stereoscopic microscopy in order to establish its original intact form and, as a consequence, its internal structure. When an insufficient number of fragments of a calculus were supplied, to properly establish its original structure, its classification being impossible, the calculus was not included in the study. If the fragmented calculus consists of several parts with different appearances, it is necessary to perform an IR analysis of each one.
An in-depth study of the fine inner structure of the calculus and the detection and identification of microcomponents (not identifiable using conventional IR spectrometry) require the use of SEM coupled with X-ray microanalysis. In order to determine the importance of a given microcomponent, accurate knowledge of the fine structure of the calculus is fundamental, so that the initial zone of calculus development can be established. This zone is crucial in establishing the origin of the calculus. This study must be developed by experienced personnel.
The study of COM calculi (papillary or unattached) begins with the direct observation of its external aspect using a stereoscopic microscope. Afterwards, each calculus is sectioned into two parts along a plane as near as possible to its geometric center, in order to be able to establish the internal structure and to identify the core of the calculus.
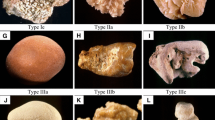
A typical papillary COM stone (see Fig. 1) basically consists of an excentrical core located near the concave region of the stone, where it was attached to the papillae, and a radially striated convex peripheral layer [8, 9]. Scanning electron microscopic study permits to detect microcomponents present in the core and to confirm also the papillary origin of the calculus by observation of the concave external cavity. Thus, the presence of abundant organic matter and tubular apical cells demonstrates the presence of a point of attachment to the renal papillae. A typical unattached COM calculus (see Fig. 2) basically consists of a symmetrically round stone with a central core surrounded by columnar COM crystals emerging from the core and by the absolute absence of a site of stone attachment to the epithelium [8, 9].

Scanning electron microscopy image of a calcium oxalate monohydrate papillary calculus. General view of the section of the calculus in which the excentrical core (in circle) located near the point of attachment (see arrows) to the papillae and a radially striated compact peripheral layer can be seen

Scanning electron microscopy image of a calcium oxalate monohydrate unattached calculus consisting of a central core (in circle) surrounded by compact columnar calcium oxalate monohydrate crystals emerging from it
The methodology used here also permits to distinguish between authentic COM calculi (COM is the initially formed crystalline phase) and COM calculi that come from the crystalline transformation of the initially formed calcium oxalate dihydrate (COD) form. Thus, SEM clearly shows that the latter exhibit a typical disorganized non-compact structure with clearly identifiable COD phantoms [10].
This methodology permits the classification of renal calculi into 11 main types [9]:
-
(1) calcium oxalate monohydrate papillary renal calculi (COM(P));
-
(2) calcium oxalate monohydrate unattached renal calculi (COM(U));
-
(3) calcium oxalate dihydrate renal calculi (COD);
-
(4) calcium oxalate dihydrate / hidroxyapatite mixed renal calculi (COD/HAP);
-
(5) hydroxyapatite renal calculi (HAP);
-
(6) magnesium ammonium phosphate (struvite) renal calculi (STR);
-
(7) calcium hydrogen phosphate dihydrate (brushite) renal calculi (BRU);
-
(8) uric acid renal calculi (UA);
-
(9) calcium oxalate/uric acid mixed renal calculi (CO/UA);
-
(10) cystine renal calculi (CYS);
-
(11) infrequent renal calculi.
Analysis of urine samples
All subjects were on free diet at the time of urine collection and none of the stone formers were undergoing pharmacological treatment of any kind. Serum analysis of these patients was performed (creatinine, calcium, magnesium, phosphorous, uric acid) mainly to evaluate the renal function. Patients with renal failure were excluded from this study. Subjects with infected urine were also excluded from the study. In sterile flasks containing thymol as a preservative, 24 h urines were collected and immediately refrigerated. After collection, the volume was recorded and the samples stored at −20°C until they were assayed. After overnight fasting, 2 h urine collection was performed and the pH was immediately measured with a glass electrode (Crison pH-meter). This urine was only used for pH evaluation, since such measurements avoid pH changes due to precipitation processes (calcium salts) that can happen during 24 h storage. On the other hand, this pH measurement better represents the urinary basal pH since it is less affected by dietary factors. Urine was collected in duplicate 1–2 months after stone passage/removal. Calcium, magnesium and phosphorus were determined by inductively coupled plasma atomic spectroscopy. Uric acid and creatinine were determined by means of a Roche Modular Analytics with 11875426216 and 11875663216 reagents, respectively, and citrate and oxalate were determined by means of the R-Biopharm enzymatic test kits No. 10139076035 and 10755699035, respectively. The urinary biochemical parameters were considered as potential lithogenic factors in abnormal conditions. Abnormal values for these parameters in accordance with our experience and literature are defined in Table 2.
Statistics
Student’s t test was used to determine the significance of changes in the calculi percentages with age and sex.
Results
The number of stone formers in each group according to age and sex, and considering the kind of calculi formed are shown in Table 1. Male/female sex ratio in the different age intervals and for the different kinds of calculi are indicated in Table 3. The percentages of each type of calculus in the considered age intervals and for men and women as well as statistical significances are shown in Fig. 3. As can be observed, the most significant aspects were:
-
COM unattached calculi increased with age in both men and women.
-
COD calculi decreased with age, but only in men. Male/female sex ratio was 3.83/1; likewise, men were much more affected by this kind of calculi than women.
-
COD/hydroxyapatite mixed calculi decreased with age in both men and women.
-
Hydroxyapatite calculi decreased with age in both men and women. Women were much more affected by this kind of calculi than men (male/female sex ratio was 0.67/1).
-
Uric acid calculi increased with age for both men and women. Male/female sex ratio was 3.85/1, that is, men were much more affected by this kind of calculi than women.
-
Calcium oxalate/uric acid mixed calculi increased with age especially for men. Male/female sex ratio was 3.47/1, that is, men were much more affected by this kind of calculi than women.
Urinary biochemical data corresponding to stone formers of each particular type of renal calculus and for each age interval and sex were obtained. Few changes, although not statistically significant, with age were observed for the mean value of urinary biochemical data:
-
An increase in urinary oxalate concentration with age for men and women for the COM unattached calculi group was seen (Fig. 4a).
-
A decrease in calcium urinary concentration with age for men for the COD calculi (Fig. 4b) as well as for the COD/hydroxyapatite mixed calculi (Fig. 4c) groups was observed.
-
A decrease in urinary phosphate with age for men and women for the hydroxyapatite calculi group was found (Fig. 4d).
-
A decrease in urinary calcium with age for women for the hydroxyapatite calculi group was also observed (Fig. 4e).

Percentages for different types of calculi in the considered age intervals and for men and women. Statistical significance of the observed changes with age is indicated for each type of renal calculus and for men and women. COM calcium oxalate monohydrate, COD calcium oxalate dihydrate, HAP hydroxyapatite, N.S. not significative

Mean values for urinary biochemical data corresponding to stone formers of different types of renal calculi and for each age interval and sex. a Oxalate urinary mean concentration for COM unattached stone formers, b calcium urinary mean concentration for COD stone formers, c calcium urinary mean concentration for COD/HAP stone formers, d phosphorus urinary mean concentration for HAP stone formers, e calcium urinary mean concentration for HAP stone formers. COM calcium oxalate monohydrate, COD calcium oxalate dihydrate, HAP hydroxyapatite
Discussion
The obtained results clearly show that COM unattached calculi increased with age. Consequently, considering the formation mechanism of this type of renal calculi [9], this increment could be attributed to the increase in urinary oxalate concentration observed for this group of stone formers (Fig. 4) and to the increase of retained heterogeneous nucleants like organic matter (for example due to hypertension [11]) or uric acid crystals with age. Also, the different behavior with age of COM papillary calculi when compared with COM unattached calculi suggests distinct pathogenic factors between them.
The decrease in COD calculi with age and only for men can be explained considering the respective decrease in urinary calcium concentration with age observed for this group of stone formers (Fig. 4b). It is interesting to point out that this decrease in such a type of calculus was not observed in women and this could be assigned to the changes in calcium metabolism during menopause, due to the consumption of calcium supplements or Vitamin D. In fact, the association between COD calculi and hypercalciuria is a well-established fact [12–16, 17] and decrease in urinary calcium excretion with age has also been reported [18, 19]. Previous papers also demonstrated that COD calculi clearly declined with age only in males, suggesting that the calcium and vitamin D supplements prescribed to menopausal women could contribute to COD stone formation [6].
The decrease in hydroxyapatite calculi with age can be attributed to the decrease in urinary phosphorus (Fig. 4d) and calcium concentration (Fig. 4e) with age, observed for this group of stone formers, as was also found by other authors [6]. The decrease in urinary phosphorus excretion with age can be attributed to a decrease in phosphorus intestinal absorption due to the tendency for Vitamin D deficit [20]. Moreover, as in previous studies [6, 21, 22], the present study found a clearly higher proportion of hydroxyapatite stones in females than in males in all ages; this type of renal calculus being the only one that is clearly more frequently found in females.
As it was found by other authors [6, 22], the data presented here demonstrated a clear increase of uric acid stones with age in both genders, and a male predominance of uric acid lithiasis. Such increase can be explained considering that the prevalence of the metabolic syndrome (reduced ammoniagenesis and insulin resistance) increases with age in both genders [23]. Thus, this metabolic syndrome could be a factor in acidic urine and uric acid nephrolithiasis in older patients [24].
As a conclusion, like in previous studies, we found that COD calculi decreased with age, but only in men. These calculi were also clearly predominant in men. Hydroxyapatite calculi decreased with age in both men and women, but they were predominant in women. Uric acid calculi increased with age in both, men and women, but were predominant in men. Finally, the study presented here found that COM unattached calculi increased with age in both men and women. As a main novelty, the study presented here demonstrates the importance of distinguishing between COM papillary stones and COM unattached stones, since the etiologic factors responsible for their origin must be clearly different.
References
Trinchieri A (1996) Epidemiology of urolithiasis. Arch Ital Urol Androl 68:203–249
Ramello A, Vitale C, Marangella M (2000) Epidemiology of nephrolithiasis. J Nephrol (13 suppl) 3:S45–S50
el-Reshaid K, Mughal H, Kapoor M (1997) Epidemiological profile, mineral metabolic pattern and crystallografic analysis of urolithiasis in Kuwait. Eur J Epidemiol 13:229–234
Gault MH, Chafe L (2000) Relationship of frequency, age, sex, stone weight and composition in 15,624 stones: comparison of results for 1980 to 1983 and 1995 to 1998. J Urol 164:302–307
Mandel N, Mandel I, Fryjoff K, Rejniak T, Mandel G (2003) Conversion of calcium oxalate to calcium phosphate with recurrent stone episodes. J Urol 169:2026–2029
Daudon M, Doré J-C, Jungers P, Lacour B (2004) Changes in stone composition according to age and gender of patients: a multivariate epidemiological approach. Urol Res 32:241–247
Grases F, García-Ferragut L, Costa-Bauzá A (1998) Analytical study of renal calculi. a new insight. Recent Res Devel Pure Appl Anal Chem 1:187–206
Grases F, Costa-Bauzá A, García-Ferragut L (1998) Biopathological crystallization: a general view about the mechanisms of renal stone formation. Adv Colloid Interface Sci 74:169–194
Grases F, Costa-Bauzá A, Ramis M, Montesinos V, Conte A (2002) Simple classification of renal calculi closely related to their micromorphology and etiology. Clin Chim Acta 322:29–36
Iwata H, Iio S, Nishio S, Takeuchi M (1992) Architecture of mixed calcium oxalate dihydrate and monohydrate stones. Scanning Microsc 6:231–238
Palatini P (2003) Microalbuminuria in hypertension. Curr Hypertens Rep 5:208–214
Asplin JR, Lingeman J, Kahnoski R, Mardis H, Parks JH, Coe FL (1998) Metabolic urinary correlates of calcium oxalate dihydrate in renal stones. J Urol 159:664–668
Curhan GC, Willet WC, Speizer FE, Stampfer MJ (2001) Twenty-four-hour urine chemistries and the risk of kidney stones among women and men. Kidney Int 59:2290–2298
Daudon M, Bader CA, Jungers P (1993) Urinary calculi: review of classification methods and correlations with etiology. Scaning Microsc 7:1081–1104
Daudon M, Labrunie M, Hennequin C, Lacour B, Jungers P (1997) Relative influence of calcium and oxalate urine concentration on the risk of calcium oxalate crystallization. In: Jungers P, Daudon M (eds) Renal stone disease. Crystallization process, pathophysiology, metabolic disorders and prevention. Elsevier, Paris, p 72
Daudon M, Reveillaud RJ (1984) Whewellite and weddellite, toward a different etiopathogenesis: the significance of morphological typing of calculi. Nephrologie 5:195–201
Pierratos AE, Khalaff H, Cheng PT, Psihramis K, Jewett MAS (1994) Clinical and biochemical differences in patients with pure calcium oxalate monohydrate and calcium oxalate dihydrate kidney stones. J Urol 151:571–574
Halloran BP, Lonergan ET, Portale AA (1996) Aging and renal responsiveness to parathyroid hormone in healthy men. J Clin Endocrinol Metab 81:2192–2197
Kotowicz MA, Melton LJIII, Cedel SL, O’Fallon WM, Riggs BL (1990) Effect of age on variables relating to calcium and phosphorus metabolism in women. J Bone Miner Res 5:345–352
Baylink DJ, Jennings JC, Mohan S (1998) Calcium and bone homeostasis and changes with aging. In: Hazzard W, Blass J, Ettinger W, Halter J, Ouslander J, (eds) Principles of geriatric medicine and gerontology, 4th edn. Mc Graw-Hill, pp 1041–56
Robertson WG (2001) The changing pattern of urolithiasis in the UK and its causes. In: Kok DJ, Romijn HC, Verhagen PCMS, Verkoelen CF (eds) Eurolithiasis. Shaker, Maastricht, p 9
Robertson WG, Peacock M, Heyburn PJ (1980) Clinical and metabolic aspects of urinary stone disease in Leeds. Scand J Urol Nephrol Suppl 53:199–206
Ford ES, Giles WH, Dietz WH (2002) Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA 287:356–359
Abate N, Chandalia M, Cabo-Chan AV Jr, Moe OW, Sakhaee K (2004) The metabolic syndrome and uric acid nephrolithiasis: novel features of renal manifestation of insulin resistance. Kidney Int 65:386–392
Acknowledgments
We gratefully acknowledge the financial support of Conselleria de Innovacio i Energia of Govern Balear (Grant PCTIB-2005GC4-06) and Dirección General de Investigación, Ministerio de Educació y Ciencia (Grant CTQ2006-05640).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Costa-Bauzá, A., Ramis, M., Montesinos, V. et al. Type of renal calculi: variation with age and sex. World J Urol 25, 415–421 (2007). https://doi.org/10.1007/s00345-007-0177-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-007-0177-4