
Abstract
As the biological behaviour of even early stage renal cell cancer (RCC) strongly correlates with tumor size, it has been argued that the inclusion of RCC up to a maximum diameter of 7 cm into a common subgroup classified as T1 according to the 5th edition of the TNM system would not adequately represent the different biological aggressiveness of these malignancies. Taking this into account, the TNM classification, which now categorizes T1 RCC as T1a and T1b according to a cutoff size of 4 cm, was recently modified. However, only a few larger investigations, mainly based on univariate statistical analyses, that support the suitability of this cutoff are at present available from the literature. Therefore, it was the aim of the present investigation to determine the tumor size that best separates patients with low responses from those with high risk for tumor progression by univariate (log rank test) and multivariate (Cox regression model) statistical analyses. Between 1981 and 2000, 652 patients (443 males and 209 females) underwent tumor nephrectomy in our clinic for the diagnosis of RCC. Of these, 243 patients revealed primary tumors with a local growth not extending beyond the renal capsula at the time of surgery. For the different cutoff levels (starting from 2 cm in increments of 1 cm up to 8 cm) that were selected to subdivide the patients into groups according to the maximum tumor diameter, the correlation between tumor size and overall survival was determined by univariate and multivariate statistical analyses. It became evident that although during univariate analysis the prognostic value of a cutoff size of 4 cm was confirmed, multivariate analysis identified the highest relative risk for cause-specific death (2.93) for patients having tumors larger than 5 cm in maximum diameter. Therefore, the 5 cm cutoff seems to best determine the clinical prognosis of patients undergoing tumor nephrectomy for early stage RCC. The present study demonstrates the need for multivariate statistical approaches when the latest modification of the TNM classification system is critically evaluated.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Before 1950, a median 5-year survival rate of 30% was reported for patients undergoing radical nephrectomy as treatment for renal cell cancer (RCC). The introduction of new imaging methods such as ultrasonography and computed tomography (CT-scans) into the clinical routine, together with their further refinement during the last few decades, has resulted in the diagnosis of more early stage renal cell tumors. The latter development has not only contributed to an improvement of the patients’ clinical prognosis but has also allowed new insights into the clinical course following surgery for organ-confined RCC classified as T1 or T2 disease according to the TNM classification.
Due to clinical observations, the cutoff size between stage T1 and T2 RCC was changed from 2.5 to 7 cm in the 5th edition of the TNM system published in 1997 [1, 3, 4]. However, it was argued that tumors, although now classified as T1 disease, exceeding a critical maximum diameter of about 4–5 cm reveal a more aggressive biological behaviour and a higher tendency towards metastatic spread than smaller tumors [5, 6, 7, 8]. This results in a deterioration in the patients’ long-term survival. Due to the outcome of subsequently performed studies which evaluated the appropriateness of the aforementioned modification, a further subdivision of stage T1 tumors into a T1a and T1b sugroup was suggested on the basis of a 4 cm size cutoff and introduced into the latest modification of the TNM classification system [2, 5, 6]. Although several authors confirmed that the inclusion of all organ-confined tumors up to a maximum diameter of 7 cm in the T1 group insufficiently reflects the different biological behaviour of organ-confined RCC [5, 6, 7, 8], there was only little consensus on the cutoff size which exhibits the greatest predictive value for the patients’ long-term survival in the past. Therefore, it was the aim of the present investigation to determine the tumor size that best separates patients at low compared to high risk of death from RCC by univariate (log rank test) and multivariate (Cox regression model) statistical analyses in a total of 243 patients with organ-confined RCC.
Patients and methods
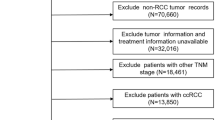
Between 1981 and 2000, 652 patients (443 males and 209 females) underwent tumor nephrectomy in our clinic for the diagnosis of RCC. According to the patient and tumor characteristics recorded by the Clinical Cancer Registry of Hanover University Medical School, 243 patients [152 (63%) males and 91 (37%) females] revealed primary tumors with a local growth not extending beyond the renal capsula at the time of surgery. The median age of the patients at first diagnosis was 59 years(range 33–84 years) and 60 years (range 20–85 years) for male and female patients, respectively. The median postoperative follow-up was 2.4 years (range 2 months–18 years).
Patient and tumor characteristics, including the histopathological findings following surgical treatment, were obtained from the H.I.T. program system (Hanover Information System for Tumor Data) of the Clinical Cancer Registry of Hanover University Medical School, and subjected to statistical evaluation. Univariate analysis using a log rank test was employed to determine the possible prognostic importance of different cutoff values for the maximum tumor diameter (starting from 2 cm in increments of 1 cm up to 8 cm), in addition to patient’s age and the presence/absence of regional lymph node or distant metastases, for the long-term survival following tumor nephrectomy. For each of the different cutoff levels that were selected to subdivide the patients into groups according to the maximum tumor diameter, the correlation between tumor size and overall survival was determined. Overall survival was calculated according to the Kaplan-Meier method from the time of tumor nephrectomy and either death from disease or date of last follow-up. Multivariate Cox regression analysis was used to determine whether any of the factors tested—age, tumor size according to different cutoff values, lymph node status and the presence of distant metastases—could be identified as independent parameters of prognostic relevance.
Results
The median size of the RCC specimens included in the present investigation was 4.8 cm. In none of the cases did local tumor growth extending beyond the renal capsula. Regional lymph node or distant metastases were identified in 16 (11 males and five females) and 30 (19 males and 11 females) patients, respectively. In terms of median tumor size and the frequency of regional lymph nodes or distant metastases, the comparison between male and female patients did not reveal any significant differences. After a median follow-up of 28 months (range 2 months–18 years) for the whole group of 243 patients, 41 patients died from progressive disease after surgical treatment.
At 5 and 10 years following initial treatment, overall survival was 78% (78%/76% for males and females) and 69% (72%/66% for males and females) for the whole group of 243 patients included in the present investigation. The 5- and 10-year survival rates for those revealing distant metastases decreased to 39% and 28%, respectively.
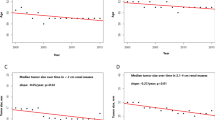
To determine the prognostic value of the maximum diameter of the tumors for the clinical course of the disease, tumor sizes were correlated at 1 cm increments (range 2–8.5 cm) with postoperative long-term survival. During univariate statistical analysis, tumor size revealed a statistically significant impact on the patient’s clinical prognosis at any cutoff value evaluated (Table 1). However, a cutoff size of 5 cm separated best for 5 year patient survival (Figs. 1). Whereas the median long-term survival was 5.8 years (2 months–18 years) for patients whose maximum tumor diameter exceeded the 5 cm cutoff level, a median survival has not yet been determined for patients with smaller tumor sizes at the time of data evaluation. Accordingly, the long-term survival at 5- and 10 years after surgery was 91%/86% (maximum tumor diameter <5 cm) and 55%/45% (maximum tumor diameter ≥5 cm), respectively. Statistically, this difference proved to be highly significant (P<0.01). In contrast to univariate analysis, the classification of the patients into groups with tumors of <3 cm/≥3 cm (P=0.14) or <4 cm/≥4 cm (P=0.11) in maximum diameter did not demonstrate any independent predictive value for long-term survival following surgery using multivariate analysis. In addition to all other cutoff sizes evaluated, the presence of regional lymph node or distant metastases was identified to independently predict the long-term survival of the patients (P<0.01) (Table 2). As in the univariate analysis, a 5 cm cutoff was associated with the highest relative risk (2.93) of dying from tumor progression during the further course of the disease (Table 2).

Long-term survival of patients classified into group A (<5 cm) or group B (>5 cm) according to the maximum diameter of the primary renal cell cancer specimens. Compared with other cutoff values for tumor size, the utilization of a 5 cm cutoff best separated patients with an excellent or less favorable prognosis following tumor nephrectomy (x and y axes: relative overall survival and follow-up in months, respectively)
Discussion
The widespread availability of modern imaging methods such as ultrasonography and computed abdominal tomography have led to the diagnosis of RCC at an earlier stage in the majority of patients. The latter development has not only improved the clinical prognosis of the patients, but has also allowed new insights into the natural course of the disease following surgical treatment. Previously obtained clinical observations have resulted in a modified TNM classification system of renal cancer that has changed the cutoff size between T1 and T2 organ-confined RCC from 2.5 to 7 cm [1]. However, it has been subsequently argued that the classification of all organ-confined tumors up to a maximum diameter of 7 cm as stage T1 disease would not appropriately reflect the interindividually different biological behaviour of RCC that seems to be, at least in part, correlated to tumor size [6, 7, 8, 9, 13, 18, 20]. Consequently, attempts have been made to divide patients classified as stage T1 according to the 1997 TNM classification [1] into subgroups at high and low risk for tumor progression according to different tumor size cutoffs.
In one of the largest series reported so far, Gettman et al. [10] retrospectively analyzed the records of 1,547 surgically treated RCC patients and evaluated the impact of various size cutoffs less than 7 cm on the clinical prognosis following resection of the tumor-bearing kidney. Survival differences according to tumor size were demonstrated for cutoffs of less than 4.5, 4.5–6 and over 6.6 cm.
An investigation by Krejci et al. [11] included 289 patients subjected to nephron-sparing surgery for T1 disease as determined according to the 1997 TNM classification. After a follow-up of 5 years, the metastasis-free and cause-specific survival was 94%/97% and 74%/86% for tumors revealing a maximum diameter of < and >5 cm, respectively. In the present investigation, patients with organ-confined tumors of >5 cm in maximum diameter had a significantly decreased long-term survival at 5 years following surgery (55%) when compared with the results reported by Krejci et al. However, this might to due to the inclusion of RCCs exceeding a diameter of 8 cm (n=21).
In addition to several patient and tumor characteristics (tumor stage according to the TNM classification system, histological grade, histological growth pattern, ECOG performance status, symptoms and application of immunotherapy for metastatic disease), Zisman et al. [12] determined the predictive value of 11 tumor size cutoffs between 1 and 10 cm for the metastasis free and long-term survival following surgical treatment for RCC. Whereas a size cutoff of 4.5 cm revealed the greatest predictive value for metastasis free survival, the long-term survival of patients with organ-confined tumors of 4.5–7 cm was equal to that of patients harbouring T2 disease according to the 1997 TNM classification. Therefore, it was proposed not to classify all tumors up to 7 cm uniformly as stage T1 but to better distinguish two subgroups at low and high risk for tumor progression, respectively.
Delahunt et al. [14] investigated the impact of tumor size on the clinical prognosis of 116 patients with organ-confined RCC. They demonstrated that the risk of death as a result of RCC at 2 and 5 years after surgery was strongly correlated with the maximum diameter of the primary tumors. During multivariate statistical analysis, tumor size correlated well with survival, whereas Fuhrman grade and proliferative activity as determined by Ki-67 expression did not [14]. Accordingly, the independent prognostic value of tumor size for the clinical prognosis of the patients was confirmed by multivariate statistical analysis in the present investigation.
In a recently reported investigation [15] that included 196 patients with one of four heritable forms of RCC (clear cell in Von Hippel-Lindau disease, hereditary basophilic papillary, hereditary renal oncocytoma, and Birt-Hogg Dube oncocytic/chromophobe), metastases could not be identified if the maximum diameter of the tumors was less than 3 cm. In accordance with this observation, our own group demonstrated a strong correlation between tumor size and the risk for an intra-adrenal metastatic spread originating from a primary renal tumor. Whereas the risk for adrenal metastases was significantly lowered when the primary tumor had a maximum diameter of <5 cm, in none of the tumors ≤2.5 cm in size were adrenal metastases detected [21].
Elmore et al. [19] reviewed 544 patients who underwent radical nephrectomy for the treatment of organ-confined RCCs. The long-term survival was correlated to tumor size at 0.5 cm increments for tumor diameters ranging from 2.5 up to 7 cm. A 5 cm cutoff not only best separated for 5 year survival, but also predicted the likelihood of the primary tumor developing non-organ-confined growth. Although the risk of the presence of both nodal and distant metastases correlated well with tumor size, the level of significance for the prediction of the presence of regional lymph node or distant metastases was not reached for tumors in the 2.5–7 cm range at any size cutoff analyzed.
A 5 cm cutoff for the maximum diameter of RCC specimens separated patients at high and low risk of death from tumor progression most appropriately in our study. During univariate analysis, the long-term survival was 91%/86% and 55%/45% at 5 and 10 years following surgery. However, the present investigation is one of the very few evaluating the prognostic value of tumor size for patients diagnosed with RCC by a multivariate analysis that included different patient and tumor characteristics such as age, regional lymph node status and the presence of distant metastases, in addition to maximum tumor diameter. Although an independent prognostic value was also demonstrated for cutoffs at 6.7 and 8 cm, patients whose tumors exceeded the critical size of 5 cm were characterized by the highest relative risk for cause-specific death when compared with those having a tumor diameter of ≤5 cm. Therefore, the 5 cm cutoff seems to best distinguish between organ-confined RCCs at high and low risk for the development of tumor progression during the further course of the disease. Recognizing the outcome of our univariate analysis that identified a significant predictive value for any cutoff size evaluated, the present study clearly demonstrates that the determination of a cutoff value that most appropriately subdivides RCC patients not harbouring extrarenal tumor growth into groups at low and high risk for disease progression requires multivariate statistical evaluations. Taking this point into consideration, the latest modification of the TNM classification system [2] should be critically evaluated.
References
Sobin LH, Wittekind CH (1997) TNM classification of malignant tumours, 5th edn. Wiley-Liss, New York
Wittekind C, Meyer H.-J., Bootz F (2002) TNM-Klassifikation maligner Tumoren, 6th edn. Springer, Berlin Heidelberg
Javidan J, Stricker HJ, Tamboli P, Amin MB, Peabody JO, Deshpande A, Menon M, Amin MB (1999) Prognostic significance of the 1997 TNM classification of renal carcinoma. J Urol 162: 1277
Minervini R, Minervini A, Fontana N, Traversi C, Cristofani R (2000) Evaluation of the 1997 tumour, nodes and metastases classification of renal cell carcinoma: experience in 172 patients. Br Urol 86: 19
Guinan P, Sobin LH, Algaba F, Badellino F, Kameyama S, MacLennan G, Novick A (1997) TNM staging of renal cell carcinoma. Workgroup no 3. Cancer 80: 992
Hafez KS, Fergany AF, Novick AC (1999) Nephron sparing surgery for localized renal cell carcinoma: impact of tumor size on patient survival, tumor recurrence and TNM staging. J Urol 162: 1930
Licht M, Novick AC, Goormastic M (1994) Nephron sparing surgery in incidental vs suspected renal cell carcinoma. J Urol 152: 39
Lerner SE, Hawkins CA, Blute ML, Grabner A, Wollan PC, Eickholt JT, Zincke H (1996) Disease outcome in patients with low stage renal cell carcinoma treated with nephron sparing or radical surgery. J Urol 155: 1868
Shinohara N, Harabayashi J, Koyanagi T (2001) Stage-specific follow-up protocol after radical nephrectomy for renal cell carcinoma: could we follow the T1B patients by a same follow-up protocol of T1A patients? J Urol 165 [Suppl]: 161
Gettman MT, Blute ML, Spotts B, Bryant SC, Zincke H (2001) Pathologic staging of renal cell carcinoma. Significance of tumor classification with the 1997 staging system. Cancer 91: 354
Krejci KG, Frank I, Blute ML. Grade-and size-specific outcomes for stage T1 renal cell carcinoma (RCC) after nephron sparing surgery (NSS). J Urol [Suppl]: 158
Zisman A, Pantuck AJ, Chao D, Dorey F, Said JW, Gitlitz BJ, De Kernion JB, Figlin RA, Belldegrun AS (2001) Reevaluation of the 1997 TNM classification for renal cell carcinoma: T1 and T2 cutoff point at 4.5 cm rather than 7 cm better correlates with clinical outcome. J Urol 166: 54
Slaton JW, Levy DA, Perrotte P et al. (2001) Practical application of renal cell carcinoma prognostic factors to a risk factor driven approach to tumor surveillance after radical nephrectomy. J Urol 165 [Suppl]: 160
Delahunt B, Kittelson JM, McCredie MR, Reeve AE, Stewart JH, Bilous AM (2002) Prognostic importance of tumor size for localized conventional (clear cell) renal cell carcinoma. Cancer : 658
Walker JR, Choyke PL, Glenn G et al. (2001) Association of renal tumor size and metastasis in four different hereditary renal tumor syndromes. J Urol [Suppl]: 160
Delahunt B, Eble JN (1997) Papillary adenoma of the kidney: an evolving concept. J Pathol 7: 99
Baltaci S, Orhan D, Soyupek S et al. (2000) Influence of tumor stage, size, grade, vascular involvement, histological cell type and histological pattern on multifocality of renal cell carcinoma. J Urol 164: 36
Turner KJ, Huson SM, Moore N, Britton BJ, Cranston D (2001) Von Hippel-Lindau disease: renal tumors less than 3 cm can metastasize. J Urol 165: 1207
Elmore JM, Kadesky KT, Koeneman KS, Sagalowsky AL(2002) Reassessing the 1997 TNM classification system for renal cell carcinoma: a 5.0 cm T1/T2 cut-off better stratifies clinical outcome. J Urol 167 [Suppl]: 194
Miller J, Fischer C, Freese R, Altmannsberger M, Weidner W (1999) Nephron-sparing surgery for renal cell carcinoma: is tumor size a suitable parameter for indication. Urology 54: 988
Kuczyk M, Münch T, Machtens S, Bokemeyer C, Wefer A, Hartmann J, Kollmannsberger C, Kondo M, Jonas U (2002) The need for routine adrenalectomy during surgical treatment for renal cell cancer: the Hanover experience. BJU Int 89: 517
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kuczyk, M., Wegener, G., Merseburger, A.S. et al. Impact of tumor size on the long-term survival of patients with early stage renal cell cancer. World J Urol 23, 50–54 (2005). https://doi.org/10.1007/s00345-004-0483-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-004-0483-z