
Abstract
Objectives
To establish inter-reader reliability of CT Liver Imaging Reporting and Data System (LI-RADS) and explore factors that affect it.
Methods
MEDLINE and EMBASE databases were searched from January 2014 to March 2020 to identify original articles reporting the inter-reader reliability of CT LI-RADS. The imaging analysis methodology of each study was identified, and pooled intraclass correlation coefficient (ICC) or kappa values (κ) were calculated for lesion size, major features (arterial-phase hyperenhancement [APHE], nonperipheral washout [WO], and enhancing capsule [EC]), and LI-RADS categorization (LR) using random-effects models. Subgroup analyses of pooled κ were performed for the number of readers, average reader experience, differences in reader experience, and LI-RADS version.
Results
In the 12 included studies, the pooled ICC or κ of lesion size, APHE, WO, EC, and LR were 0.99 (0.96−1.00), 0.69 (0.58–0.81), 0.67 (0.53–0.82), 0.65 (0.54–0.76), and 0.70 (0.59–0.82), respectively. The experience and number of readers varied: studies using readers with ≥ 10 years of experience showed significantly higher κ for LR (0.82 vs. 0.45, p = 0.01) than those with < 10 years of reader experience. Studies with multiple readers including inexperienced readers showed significantly lower κ for APHE (0.55 vs. 0.76, p = 0.04) and LR (0.45 vs. 0.79, p = 0.02) than those with all experienced readers.
Conclusions
CT LI-RADS showed substantial inter-reader reliability for major features and LR. Inter-reader reliability differed significantly according to average reader experience and differences in reader experience. Reported results for inter-reader reliability of CT LI-RADS should be understood with consideration of the imaging analysis methodology.
Key Points
• The CT Liver Imaging Reporting and Data System (LI-RADS) provides substantial inter-reader reliability for three major features and category assignment.
• The imaging analysis methodology varied across studies.
• The inter-reader reliability of CT LI-RADS differed significantly according to the average reader experience and the difference in reader experience.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The Liver Imaging Reporting and Data System (LI-RADS) was introduced in 2011 [1] and recently updated in 2018 to standardize the performance of liver imaging in patients at risk for hepatocellular carcinoma (HCC) [2, 3]. LI-RADS provides a standardized lexicon for imaging features of HCC, as well as criteria for ordinal categories (i.e., LR-1 to LR-5, according to the likelihood of benignity or HCC). Unlike other malignant tumors, HCC in patients at risk can be diagnosed noninvasively on the basis of imaging features on dynamic CT or MRI, without mandatory pathologic confirmation [4]. It is therefore very important to standardize the imaging diagnosis of HCC [5].
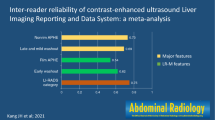
Given the wide adoption of LI-RADS in research and clinical practice, extensive evaluation of the diagnostic accuracy of LI-RADS has been reported [6,7,8], but variable imaging protocols and the lack of using standardized lexicon may challenge the synthesis of solid evidence [9]. A recent multi-center, multi-reader study found that CT LI-RADS demonstrated substantial to almost perfect inter-reader reliability, with intraclass correlation coefficients (ICCs) of 0.67 for LI-RADS category assignment and 0.79 to 0.86 for major features [9]. In addition, this previous study showed that the inter-reader reliability of LI-RADS was not significantly affected by LI-RADS familiarity or years of experience [9]. Although this multi-center, multi-reader study determined the inter-reader reliability for CT LI-RADS, variable results for inter-reader reliability of CT LI-RADS have been reported after this study [10,11,12,13], with kappa values (κ) for LI-RADS category assignment ranging from 0.44 to 0.90.
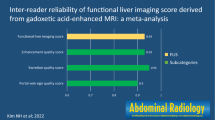
Recently, a meta-analysis of inter-reader reliability of MRI LI-RADS has been published, reporting overall substantial agreement [14]. However, that of CT LI-RADS has not yet been done. Considering the fact that discrepancy rates in imaging tests can be influenced by various imaging analysis factors, as well as reader characteristics [15, 16], we hypothesized that differences in imaging analysis methodology between each study might be partly responsible for these heterogeneous results for the inter-reader reliability of CT LI-RADS. Therefore, we aimed to establish inter-reader reliability of CT LI-RADS and explore factors that affect it.
Materials and methods
This study was conducted and reported according to the guidelines for Meta-analysis of Observational Studies in Epidemiology [17] and Preferred Reporting Items for Systematic Reviews and Meta-Analyses [18, 19].
Literature search
A systematic search was performed in MEDLINE and EMBASE databases to find original studies reporting the inter-reader reliability of LI-RADS categorizations and major imaging features of LI-RADS for the diagnosis of HCC using CT. The search query was developed to provide a sensitive search of potentially eligible articles (Supplementary Table 1). The search was performed for articles published from January 2014, to include original studies using LI-RADS v2014 or later versions of LI-RADS. The literature search was updated until March 2020. The search was limited to studies published in English and those involving human subjects. The bibliographies of the included articles were also screened to expand the scope of the search and to prevent other potentially relevant studies from being omitted.
Eligibility criteria
Studies were included when all of the following criteria were met: (a) population—patients at risk for HCC with a focal observation, i.e., adult patients with cirrhosis or chronic viral hepatitis [20]; (b) index test—dynamic contrast-enhanced CT; (c) comparator—no requirements; (d) outcome—inter-reader reliability of major imaging features and LI-RADS categorization; and (e) study design—any type of study including observational studies and clinical trials. Studies were excluded when any of the following criteria were met: (a) case reports, meta-analyses, review articles, letters, comments, and conference abstracts; (b) studies with overlapping patient cohorts and data; (c) studies not related to the field of interest of this study; and (d) studies with insufficient data to determine inter-reader reliability. Studies were independently screened by two reviewers using their titles and abstracts according to the inclusion and exclusion criteria. After exclusion of ineligible studies, we performed a full-text review of the remaining potentially eligible studies. If any disagreement was present between the two reviewers, the studies were re-evaluated at a consensus meeting.
Data extraction
Using predefined data forms, the following data were extracted from the included studies: (a) study characteristics—author, year of publication, publishing country, study design, study type, and subject enrollment method; (b) demographic and clinical characteristics—number of patients, patients’ age, number, and type of lesions, and type of reference standard; (c) CT techniques—number of detectors, multiphase sequence, and slice thickness; (d) methodology of imaging analysis—number of readers, experience of each reader, difference in reader experience, independent review, clarity of blinding to reference standard in the review, and version of LI-RADS used; and (e) study outcomes—inter-reader reliability according to lesion size, major features (arterial-phase hyperenhancement [APHE], nonperipheral washout [WO], and enhancing capsule [EC]), and LI-RADS categorization. To determine inter-reader reliability, the ICCs for continuous variables and κ for categorical variables with standard errors were extracted for each major feature and LI-RADS categorization. Data extraction was performed independently by the two reviewers, and any discrepancies between them were resolved at a consensus meeting.
Quality assessment
Study quality was assessed using the Guidelines for Reporting Reliability and Agreement studies [21]. Important elements included the following seven domains: descriptions of the index test (CT techniques), study subjects (recruitment methods and demographic characteristics), readers (number and experience level), reading process (availability of clinical information and independent review), clarity of the blinding review, statistical analysis, and actual number of subjects and observations. Each category was scored as high quality if it was described in sufficient detail in the article with no potential bias. The study quality was assessed independently by the two reviewers, with any discrepancies between them being resolved at a consensus meeting.
Data synthesis and statistical analysis
To calculate meta-analytic summary estimates, the ICC with standard error was summarized for lesion size, and κ with standard error was summarized for APHE, WO, EC, and LI-RADS categorization from each study. If the original study did not report standard error, it was estimated from the 95% confidence interval (CI). The meta-analytic pooled ICC and κ with 95% CI were calculated using the DerSimonian-Laird random-effects model with or without Knapp and Hartung adjustment [22]. ICC and κ were categorized according to Landis and Koch as follows: < 0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial; and 0.81–1.00, almost perfect reliability [23]. Heterogeneity was assessed using the Cochran Q-test and I2 statistics [24], with I2 > 50% or p < 0.10 in the Cochran Q-test being considered to indicate substantial heterogeneity.
To evaluate the inter-reader reliability of LI-RADS according to the imaging analysis methodology, we performed subgroup analyses according to the following variables: (a) number of readers (two readers vs. more than two readers); (b) average reader experience (≥ 10 years of experience in abdominal/liver imaging vs. < 10 years of experience); and (c) difference in reader experience (all experienced readers vs. multiple readers with inexperienced readers, i.e., < 5 years of post-fellowship experience). In addition, we performed subgroup analysis according to the version of LI-RADS used (v2014, v2017, or v2018).
Meta-regression analysis was performed to explore the causes of study heterogeneity, which included the following covariates: study design (prospective vs. retrospective), study type (cohort vs. case-control), subject enrollment (consecutive vs. selective), number of CT detectors (≥ 64 channels in all included CT vs. others), dynamic CT sequence (quad-phase including unenhanced, arterial phase, portal venous phase, and delayed or equilibrium phase vs. triple-phase), CT slice thickness (≤ 3 mm vs. others), and clarity of blinding to reference standard during the review (clear vs. unclear).
Funnel plots and rank tests were used to assess the presence of any publication bias. R version 3.6.3 with the “metafor” package was used to perform the analyses.
Results
Literature search
The systematic literature search initially identified 263 articles (Fig. 1). After removing 109 duplicate articles, 154 articles were screened by their titles and abstracts, and 99 articles were excluded. Full-text reviews were performed for 55 potentially eligible articles, and 43 articles were excluded. Finally, 12 original articles with a total of 2285 lesions were included in this study [9,10,11,12,13, 25,26,27,28,29,30,31].

Flow diagram of the study selection process. LI-RADS, Liver Imaging Reporting and Data System
Characteristics of the included studies
The detailed characteristics of the included studies are summarized in Table 1. Eleven studies were retrospective [9,10,11,12,13, 26,27,28,29,30,31], and one study was prospective [25]. Eleven studies were cohort studies [9,10,11,12,13, 25,26,27,28, 30, 31], and one was a case-control study [29]. All of the included studies were analyzed independently by the readers. Six studies used histopathology for the reference standard [11,12,13, 26, 29, 30], four used a combination of histopathology and clinical follow-up [10, 25, 27, 31], and two did not use a reference standard because they focused on inter-reader reliability rather than diagnostic accuracy [9, 28]. The readers in 10 studies were blinded to the reference standard [10,11,12,13, 25,26,27, 29,30,31], whereas the other two studies were unclear on blinding [9, 28].
Imaging analysis methodologies of the included studies
The imaging analysis methodologies of each study are summarized in Table 2. Nine studies used two readers [10,11,12, 25, 27,28,29,30,31], and three studies used more than two [9, 13, 26]. The experience level of the readers was variable, ranging from trainees to 23 years of experience in liver imaging. Of the 12 included studies, eight stated the experience of each reader [10,11,12, 25, 26, 28, 30, 31], with the average reader experience being 10.8 years in abdominal/liver imaging. Three studies included both experienced readers and inexperienced readers [12, 13, 31]. Nine studies used LI-RADS v2014 [9, 13, 25,26,27,28,29,30,31], two studies used v2017 [10, 31], and one study used v2018 [12].
Study quality
All included studies showed a quality score of five or more for the seven criteria evaluated. Description of the index test was lacking in two studies [9, 29], and readers’ experience levels were not reported in two studies [27, 29]. In addition, the presence of blinding during the review was unclear in two studies [9, 28]. Further details on the study quality are provided in Supplementary Figure 1.
Meta-analytic pooled inter-reader reliability of LI-RADS
The meta-analytic pooled estimates of inter-reader reliability of LI-RADS are summarized in Fig. 2. For lesion size, the ICCs ranged from 0.74 to 0.99, and the meta-analytic pooled ICC was 0.99 (95% CI, 0.96−1.00), which was close to perfect reliability. Among the three major features, the highest meta-analytic pooled κ was shown by APHE (0.69; 95% CI, 0.58–0.81), followed by WO (0.67; 95% CI, 0.53–0.82). All three major features showed substantial inter-reader reliability. The κ for the LI-RADS categorization ranged from 0.44 to 0.90, with a meta-analytic pooled κ of 0.70 (95% CI, 0.59–0.82), showing substantial inter-reader reliability.

Meta-analytic pooled inter-reader reliability for the CT Liver Imaging Reporting and Data System (LI-RADS). a Lesion size, b arterial-phase hyperenhancement, c nonperipheral washout, d enhancing capsule, and e LI-RADS categorization. ICC, intraclass correlation coefficient
Subgroup analysis according to the imaging analysis methodology
Subgroup analyses of inter-reader reliability for the major features and LI-RADS categorization according to the imaging analysis methodology are summarized in Table 3. Both studies with two readers and those with more than two readers showed moderate to substantial inter-reader reliability for the three major features (κ = 0.64–0.71) and LI-RADS categorization (κ = 0.56–0.64). Regarding the reader experience, the meta-analytic pooled κ for LI-RADS categorization was significantly higher in studies using readers with ≥ 10 years of experience than in those using readers with < 10 years of experience (p = 0.01). Other meta-analytic pooled estimates, including lesion size, APHE, WO, and EC, showed no significant differences in inter-reader reliability between studies with readers with ≥ 10 years of experience and those with < 10 years of experience (p ≥ 0.07). In addition, the meta-analytic pooled κ for APHE and LI-RADS categorization in studies including inexperienced readers (< 5 years of post-fellowship experience) were significantly lower than those in studies where all the readers were experienced (κ = 0.55 vs. 0.76, p = 0.04 and κ = 0.45 vs. 0.79, p = 0.02, respectively). Although studies including inexperienced readers showed lower meta-analytic pooled κ for WO (κ = 0.52 vs. 0.78) and EC (κ = 0.53 vs. 0.72) than studies with only experienced readers, the differences showed only borderline significance (p = 0.06 for both).
Subgroup analysis according to LI-RADS version
All LI-RADS versions including v2014, v2017, and v2018 showed substantial inter-reader reliability for the three major features (Table 4). For the LI-RADS categorization, LI-RADS v2018 had a pooled κ of 0.53, which was lower than that of v2014 (κ = 0.69) or v2017 (κ = 0.79). Regarding the presumed year of reading session, 88% (7/8) studies with LI-RADS v2014 were conducted after 2014, but the study with LI-RADS v2018 was conducted in 2018 (Table 2).
Meta-regression analysis
Substantial study heterogeneity was noted in all five variables of lesion size, APHE, WO, EC, and LI-RADS categorization (I2 ≥ 90.0% and p < 0.001). In the meta-regression analysis, clarity of blinding to the reference standard during review was significantly associated with study heterogeneity (p ≤ 0.04; Supplementary Table 2). Studies with clear clarity of blinding showed substantial inter-reader reliability for APHE (κ = 0.64) and WO (κ = 0.62), but studies with unclear clarity of blinding showed almost perfect reliability (κ = 0.86 for APHE and 0.84 for WO). Regarding the CT technique, the number of detectors in MDCT showed a marginal significance with respect to lesion size (p = 0.05). However, other covariates including study design, study type, subject enrollment, multiphase CT, and slice thickness were not significant factors affecting study heterogeneity.
There was no significant publication bias with respect to lesion size, the three major features, or LI-RADS categorization (p ≥ 0.15, Supplementary Figure 2).
Discussion
In this study, CT LI-RADS demonstrated substantial overall inter-reader reliability for major features and LI-RADS categorization, with meta-analytic pooled κ of 0.65–0.71. Substantial heterogeneity was noted in inter-reader reliability. The imaging analysis methodology varied across the studies, and the inter-reader reliability of CT LI-RADS differed significantly according to the average reader experience (p = 0.01) and the difference in reader experience (p = 0.02).
The meta-analytic κ for CT LI-RADS categorizations found in this study was similar to that in a previous study by Fowler et al (κ = 0.71 vs. 0.73) [9]. Considering the fact that Fowler et al performed a multi-center international study using a large number of readers and a mixture of all LI-RADS category assignments [9], their results would reflect those of clinical practice with minimal potential bias. However, the inter-reader reliabilities for major features found in the current study were lower than those in the previous study (κ = 0.65–0.69 vs. 0.84–0.88). This difference may have been due to differences in reader experience, i.e., the inclusion of inexperienced readers (< 5 years of post-fellowship experience) [12, 13, 31]. In the subgroup analysis of studies including all experienced readers, which excluded three studies that included inexperienced readers [12, 13, 31], the meta-analytic κ for major features was 0.72–0.78. Because the multi-center multi-reader study by Fowler et al was conducted in the year of 2014 and the three studies with inexperienced readers indicating the remained variability of CT LI-RADS were published after this multi-center multi-reader study, it may still be a problem requiring a solution. Therefore, to promote standardization and reproducibility of CT LI-RADS, a well-designed methodology for imaging analysis is necessary, and continuous education and updates for inexperienced readers are important.
In this meta-analysis, reader experience was one of the important factors affecting the inter-reader reliability of CT LI-RADS. The reported effects of reader experience on inter-reader reliability of LI-RADS are conflicting, with Davenport et al showing that experts had higher inter-reader reliability than novices [32], but Fowler et al finding that the inter-reader reliability of LI-RADS was not significantly associated with reader experience [9]. Considering these previous results and this meta-analysis together, reader experience may be one important factor associated with the inter-reader reliability of LI-RADS. In addition, our study showed that LI-RADS v2018 had relatively lower inter-reader reliability for LI-RADS categorization than LI-RADS v2014 or v2017. Because LI-RADS v2018 has recently been updated with a simplified definition of threshold growth and simplified criteria for LR-5 [2], these updates might not yet be familiar to radiologists. Although Fowler et al reported that LI-RADS inter-reader reliability was not significantly affected by LI-RADS familiarity, this previous study evaluated only LI-RADS v2014, and it could be difficult to evaluate the effect of LI-RADS version on inter-reader reliability. Considered together, these results indicate that the familiarity of radiologists with the latest version can also be an important factor influencing inter-reader reliability. To improve the relatively low inter-reader reliability of inexperienced readers and that associated with recently updated versions, education programs including training sets for young radiologists and regular feedback, and a comprehensive manual with both schematic figures and clinical examples to illustrate the features, would be helpful [33, 34].
Generally, as MRI provides multiparametric information from complex MRI sequences, MRI might be expected to have a lower inter-reader reliability for LI-RADS categorization than CT. However, the meta-analytic κ of CT LI-RADS categorizations in this study was very similar to that of MRI LI-RADS categorizations in a previous study (κ = 0.71 vs. 0.70) [14]. In addition, the inter-reader reliability of major features on CT was similar to that on MRI (APHE, κ = 0.69 on CT vs. 0.72 on MRI; WO, κ = 0.67 on CT vs. 0.69 on MRI; and EC, κ = 0.65 on CT vs. 0.66 on MRI) [14]. As LI-RADS uses the same definitions for major imaging features on CT and MRI [2], comparable inter-reader reliability might be expected between CT and MRI.
Our study showed that clarity of blinding to the reference standard during review was a significant factor associated with study heterogeneity, i.e., studies with unclear clarity of blinding to the reference standard showing higher inter-reader reliability for APHE (0.86 vs. 0.64, p = 0.03) and WO (0.84 vs. 0.62, p = 0.04) than those with clear clarity of blinding. Although inter-reader reliability can be evaluated according to the agreement between readers without considering the reference standard, our result suggests that knowledge of the final diagnosis might affect inter-reader reliability. Considering the fact that a recent study of MRI LI-RADS inter-reader reliability reported a similar result [14], further study is needed to evaluate why the clarity of blinding to the reference standard is associated with inter-reader reliability.
This study has some limitations. First, study heterogeneity and variations in imaging analysis methodologies were noted. To explore the causes of the variations, we robustly performed subgroup analyses and meta-regression analyses. Second, we could not include 10 articles because of insufficient data for determining inter-reader reliability. As the meta-analysis of inter-reader reliability required the standard variance as well as the ICC or κ from each study, studies that provided only the ICC or κ without standard variance were excluded. Third, although a recent meta-analysis reported that the inter-reader reliability of MRI LI-RADS, i.e., the pooled kappa value of LI-RADS categorization was 0.70 [14], our study provides additional information in that it reports the inter-reader reliability of CT LI-RADS and differences in it according to imaging analysis methodology, which were not covered in the previous study.
In conclusion, CT LI-RADS demonstrated substantial inter-reader reliability for major features and LI-RADS categorizations. The imaging analysis methodology varied across studies, and the inter-reader reliability of CT LI-RADS differed significantly according to the average reader experience and the difference in reader experience. Therefore, the reported results for inter-reader reliability of CT LI-RADS in the literature should be understood with consideration of the imaging analysis methodology.
Change history
04 May 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00330-021-07949-z
Abbreviations
- APHE:
-
Arterial-phase hyperenhancement
- CI:
-
Confidence interval
- EC:
-
Enhancing capsule
- HCC:
-
Hepatocellular carcinoma
- ICC:
-
Intraclass correlation coefficient
- LI-RADS:
-
Liver Imaging Reporting and Data System
- WO:
-
Nonperipheral washout
References
Mitchell DG, Bruix J, Sherman M, Sirlin CB (2015) LI-RADS (Liver Imaging Reporting and Data System): summary, discussion, and consensus of the LI-RADS Management Working Group and future directions. Hepatology 61:1056–1065
American College of Radiology CT/MRI LI-RADS v2018. Available via https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2018. Accessed May 27, 2019.
Chernyak V, Fowler KJ, Kamaya A et al (2018) Liver Imaging Reporting and Data System (LI-RADS) Version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology 289:816–830
Marrero JA, Kulik LM, Sirlin CB et al (2018) Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 68:723–750
Clavien PA, Lesurtel M, Bossuyt PM et al (2012) Recommendations for liver transplantation for hepatocellular carcinoma: an international consensus conference report. Lancet Oncol 13:e11–e22
Kim DH, Choi SH, Park SH et al (2019) Meta-analysis of the accuracy of Liver Imaging Reporting and Data System category 4 or 5 for diagnosing hepatocellular carcinoma. Gut 68:1719–1721
Lee SM, Lee JM, Ahn SJ, Kang HJ, Yang HK, Yoon JH (2019) LI-RADS Version 2017 versus Version 2018: diagnosis of hepatocellular carcinoma on gadoxetate disodium-enhanced MRI. Radiology 292:655–663
van der Pol CB, Lim CS, Sirlin CB et al (2019) Accuracy of the Liver Imaging Reporting and Data System in computed tomography and magnetic resonance image analysis of hepatocellular carcinoma or overall malignancy-a systematic review. Gastroenterology 156:976–986
Fowler KJ, Tang A, Santillan C et al (2018) Interreader reliability of LI-RADS Version 2014 algorithm and imaging features for diagnosis of hepatocellular carcinoma: a large international multireader study. Radiology 286:173–185
Alhasan A, Cerny M, Olivie D et al (2019) LI-RADS for CT diagnosis of hepatocellular carcinoma: performance of major and ancillary features. Abdom Radiol (NY) 44:517–528
Kim SS, Hwang JA, Shin HC et al (2019) LI-RADS v2017 categorisation of HCC using CT: Does moderate to severe fatty liver affect accuracy? Eur Radiol 29:186–194
Ludwig DR, Fraum TJ, Cannella R et al (2019) Expanding the Liver Imaging Reporting and Data System (LI-RADS) v2018 diagnostic population: performance and reliability of LI-RADS for distinguishing hepatocellular carcinoma (HCC) from non-HCC primary liver carcinoma in patients who do not meet strict LI-RADS high-risk criteria. HPB (Oxford) 21:1697–1706
Sevim S, Dicle O, Gezer NS, Baris MM, Altay C, Akin IB (2019) How high is the inter-observer reproducibility in the LIRADS reporting system? Pol J Radiol 84:e464–e469
Kang JH, Choi SH, Lee JS et al (2020) Interreader agreement of Liver Imaging Reporting and Data System on MRI: a systematic review and meta-analysis. J Magn Reson Imaging 52:795–804
Brady A, Laoide RO, McCarthy P, McDermott R (2012) Discrepancy and error in radiology: concepts, causes and consequences. Ulster Med J 81:3–9
Brady AP (2017) Error and discrepancy in radiology: inevitable or avoidable? Insights Imaging 8:171–182
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283:2008–2012
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Tang A, Hallouch O, Chernyak V, Kamaya A, Sirlin CB (2018) Epidemiology of hepatocellular carcinoma: target population for surveillance and diagnosis. Abdom Radiol (NY) 43:13–25
Kottner J, Audige L, Brorson S et al (2011) Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. J Clin Epidemiol 64:96–106
IntHout J, Ioannidis JP, Borm GF (2014) The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res Methodol 14:25
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Basha MAA, AlAzzazy MZ, Ahmed AF et al (2018) Does a combined CT and MRI protocol enhance the diagnostic efficacy of LI-RADS in the categorization of hepatic observations? A prospective comparative study. Eur Radiol 28:2592–2603
Cha DI, Jang KM, Kim SH, Kang TW, Song KD (2017) Liver Imaging Reporting and Data System on CT and gadoxetic acid-enhanced MRI with diffusion-weighted imaging. Eur Radiol 27:4394–4405
Chen N, Motosugi U, Morisaka H et al (2016) Added value of a gadoxetic acid-enhanced hepatocyte-phase image to the LI-RADS system for diagnosing hepatocellular carcinoma. Magn Reson Med Sci 15:49–59
Chernyak V, Flusberg M, Law A, Kobi M, Paroder V, Rozenblit AM (2018) Liver Imaging Reporting and Data System: discordance between computed tomography and gadoxetate-enhanced magnetic resonance imaging for detection of hepatocellular carcinoma major features. J Comput Assist Tomogr 42:155–161
Ehman EC, Behr SC, Umetsu SE et al (2016) Rate of observation and inter-observer agreement for LI-RADS major features at CT and MRI in 184 pathology proven hepatocellular carcinomas. Abdom Radiol (NY) 41:963–969
Joo I, Lee JM, Lee DH, Ahn SJ, Lee ES, Han JK (2017) Liver imaging reporting and data system v2014 categorization of hepatocellular carcinoma on gadoxetic acid-enhanced MRI: comparison with multiphasic multidetector computed tomography. J Magn Reson Imaging 45:731–740
Zhang YD, Zhu FP, Xu X et al (2016) Classifying CT/MR findings in patients with suspicion of hepatocellular carcinoma: comparison of liver imaging reporting and data system and criteria-free Likert scale reporting models. J Magn Reson Imaging 43:373–383
Davenport MS, Khalatbari S, Liu PS et al (2014) Repeatability of diagnostic features and scoring systems for hepatocellular carcinoma by using MR imaging. Radiology 272:132–142
Chernyak V, Sirlin CB (2020) Editorial for “Interreader Agreement of Liver Imaging Reporting and Data System on MRI: A Systematic Review and Meta Analysis”. J Magn Reson Imaging 52:805–806
Curci NE, Gartland P, Shankar PR et al (2018) Long-distance longitudinal prostate MRI quality assurance: from startup to 12 months. Abdom Radiol (NY) 43:2505–2512
Funding
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (grant number: NRF-2019R1G1A1099743).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Sang Hyun Choi.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors has significant statistical expertise (Ji Sung Lee).
Informed consent
Written informed consent was not required for this study because this is a meta-analysis.
Ethical approval
Institutional Review Board approval was not required because this is a meta-analysis.
Methodology
-
Systematic Review and Meta-analysis
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The Figure parts 2b and 2c were interchanged.
Supplementary Information
ESM 1
(DOCX 207 kb)
Rights and permissions
About this article

Cite this article
Kang, J.H., Choi, S.H., Lee, J.S. et al. Inter-reader reliability of CT Liver Imaging Reporting and Data System according to imaging analysis methodology: a systematic review and meta-analysis. Eur Radiol 31, 6856–6867 (2021). https://doi.org/10.1007/s00330-021-07815-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-021-07815-y