
Abstract
Objective
To identify demographic determinants of peripheral nerve diffusion tensor imaging (DTI) and to establish normal values for fractional anisotropy (FA), axial diffusivity (AD), radial diffusivity (RD), and mean diffusivity (MD).
Methods
Sixty subjects were examined at 3 Tesla by single-shot DTI. FA, AD, RD, and MD were collected for the sciatic, tibial, median, ulnar, and radial nerve and were correlated with demographic variables.
Results
Mean FA of all nerves declined with increasing age (r = −0.77), which could be explained by RD increasing (r = 0.56) and AD declining (r = −0.40) with age. Moreover, FA was inversely associated with height (r = −0.28), weight (r = −0.38) and BMI (r = −0.35). Although FA tended to be lower in men than women (p = 0.052), this difference became completely negligible after adjustment to body weight. A multiple linear regression model for FA was calculated with age and weight as predictors (defined by backward variable selection), yielding an R 2 = 0.71 and providing a correction formula to adjust FA for age and weight.
Conclusion
Peripheral nerve DTI parameters depend on demographic variables. The most important determinants age and weight should be considered in all studies employing peripheral nerve DTI.
Key points
• Peripheral nerve diffusion tensor imaging (DTI) parameters depend on demographic variables.
• Fractional anisotropy (FA) declines with increasing age and weight.
• Gender does not systematically affect peripheral nerve DTI.
• The formula presented here allows adjustment of FA for demographic variables.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Magnetic resonance neurography (MRN) is the imaging of peripheral nerves by dedicated MRI sequences [1, 2]. Beyond a purely morphologic representation, MRN may provide quantitative measures of microstructural integrity by diffusion tensor imaging (DTI) [3,4,5,6,7,8,9,10,11,12].
Having been introduced by Basser et al. [13, 14] in the 1990s, DTI is a quantitative MRI technique that uses magnetic gradients in multiple orientations to measure both the direction and magnitude of proton diffusion. Physiologically, diffusion in nerves is highly anisotropic, since diffusivity is largest in the fibre direction (referred to as axial diffusivity, AD), while numerous parallel cell membranes impede diffusivity orthogonal to the fibre direction (referred to as radial diffusivity, RD) [15,16,17]. The degree of diffusion anisotropy is commonly described by the readout parameter ‘fractional anisotropy’ (FA), a dimensionless quantity with the extremes 0 (equal diffusion in all directions) and 1 (diffusion in only one direction). FA is regarded as a general measure of nerve fibre integrity [13, 17], reflecting nerve pathology in various diseases when decreased [4, 18,19,20,21].
Evidence from histology [22, 23] and electrophysiology [24, 25] implies that ageing causes axonal loss and demyelination of peripheral nerves. Additionally, anthropometric measures such as weight and BMI are associated with nerve calibre [26]. Thus, changes in demographic variables might also modulate DTI readout parameters, and a decline of FA with age has been reported in control groups of some studies [4, 27]. While an approach to the mathematical description of this decline of FA has been undertaken in one study of 26 volunteers for the lower leg, reliable data from larger cohorts or multiple nerves is still missing [28]. Moreover, the effect of other demographic variables on DTI parameters has not been investigated so far.
We therefore conducted this study in 60 healthy individuals covering a large spectrum of age, examining multiple nerves of both upper and lower extremity to establish normal values and to identify demographic determinants of peripheral nerve DTI.
Methods
Subjects
This study was approved by the institutional ethics committee, and written informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki. A total of 30 male and 30 female healthy volunteers, distributed evenly in all decades between 20 and 80 years (five men and five women of each decade), were recruited for this prospective study.
Inclusion criteria were age between 20 and 80 years; exclusion criteria were any known neurologic (e.g. disc herniation, polyneuropathy, stroke) and systemic (e.g. diabetes mellitus, vasculitis) diseases and general contraindications for MRI.
The demographic variables age, sex, body weight, body mass index (BMI), and body height of each participant were registered as baseline characteristics.
Magnetic resonance neurography
All subjects were examined at 3.0 Tesla in a Magnetom TIM-TRIO (Siemens Healthcare, Erlangen, Germany) as previously described [11].
The examination protocol consisted of three slabs of a single shot echo planar imaging (EPI) DTI sequence at (1) the mid upper arm, (2) the mid-thigh and, (3) the proximal calf of one randomly selected side. Slab 1 was acquired in prone position and with a 16-channel receive-only multipurpose flex coil in prone position (Variety, Noras MRI Products, Hoechberg, Germany). Slabs 2 and 3 were acquired in supine position and with a 15-channel transmit-receive knee coil (Siemens Healthcare).
The sequence parameters are described in Table 1. For DTI, we used a spin-echo EPI sequence from the advanced diffusion work-in-progress package (ASP511 E) developed by Siemens. The total acquisition time including survey scans and positioning averaged about 30 min.
Image postprocessing
Segmentation was conducted by V.S. and M.K. using a freehand ROI in OsiriX, Pixmeo Sarl, Bernex, Switzerland, with 1 and 3 years of experience in peripheral nerve imaging, respectively (Fig. 1). In preliminary assessments, no significant differences between the two operators were found. Since tibial and peroneal portions of the sciatic nerve at thigh level are separated by a variable amount of ‘paraneurial’ [29] fatty connective tissue, we restricted analysis to the tibial portion of the sciatic nerve to confine measurement to true nervous tissue. The scalar DTI parameters fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD) and axial diffusivity (AD) were obtained using the plugin DTI map for OsiriX with a noise threshold of 10. All values were averaged from the central four slices of the slab for each nerve. Nerves with insufficient image quality for accurate segmentation in the b = 0 image or with insufficient image quality of the FA map were excluded from the analysis (16 of 300 nerves). Mean values were calculated for each subject as an average of all analysed nerves.

Representative images of nerve segmentation and decline of FA with increasing age. a b = 0 images and FA maps of the sciatic nerve at the thigh of a 31-year-old and a 67-year-old participant. In all our analyses, segmentation was conducted in the b = 0 image, which allows morphologic depiction of nerves. Hereafter, segmentation masks were copied into the parameter maps. Please note that the tibial portion (yellow mask) and the peroneal portion (short arrow) of the sciatic nerve are clearly distinguishable. Analysis was restricted to the tibial portion of the sciatic nerve. In greyscale FA maps, higher values of fractional anisotropy are displayed by brighter levels of grey. b Colour FA maps of the upper arm of a 25-year-old and a 70-year-old participant showing the ulnar (u), median (m), and radial (r) nerve exemplary demonstrate the decline of FA with increasing age. In colour FA maps, the absolute FA value is coded by brightness, while the prevailing direction of diffusion is coded by colour (blue = z-axis = nerve course; green = y-axis (up/down); red = x-axis (left/right))
Statistical analysis
Statistical analysis was conducted using SPSS Version 24, IBM, Armonk, USA and Prism Version 7, GraphPad Software, La Jolla, USA. All measurement results are reported as mean ± standard deviation (SD).
A p value of 0.05 or less was regarded as statistically significant. Bidirectional t tests were applied to compare metric variables between men and women without and with adjustment of DTI parameters to a body weight of 70 kg by simple linear regression. Correlation of DTI parameters with demographic variables and intercorrelation of demographic variables were described by Pearson coefficients. Multiple testing was performed.
A multiple regression model was calculated to describe FA as the dependent variable. Predictors were selected out of the independent variables age, weight, BMI, height and sex using backward variable selection with a predefined threshold of a p value of 0.05. We evaluated our model fit using a 10-fold cross-validation approach using the (predictive) R 2 as loss function. We therefore divided our data set into ten subsets. We then estimated our model where one of the subsets was omitted. This was repeated ten times so that every subset was omitted once. The omitted data sets were then used to calculate the (predictive) R 2.
Results
The demographical details of the study cohort are presented in Table 2. No significant association was found for age and weight (r = 0.03, p = 0.81), age and height (r = −0.04, p = 0.74) or age and BMI (r = 0.1, p = 0.46). Weight, height and BMI, but not age, differed significantly between the sexes. Nerve-specific values of the scalar DTI parameters FA, MD, RD and AD are displayed in Table 3.
Mean FA, defined as an average of all analysed nerves, was weakly inversely associated with height (r = −0.28, p = 0.03), weight (r = −0.38, p = 0.003) and BMI (r = −0.35, p = 0.007) (Fig. 2).

Influences of anthropometric measures and gender on nerve FA. Mean fractional anisotropy (FA), averaged over all analysed nerves, was inversely associated with a body height, b body weight and c BMI. d Mean fractional anisotropy (FA), averaged over all analysed nerves, of men tended to be decreased compared to women, slightly missing statistical significance. The difference became completely negligible after adjustment to a predefined body weight of 70 kg by simple linear regression. r = Pearson coefficient
Mean nerve FA of male subjects (0.52 ± 0.06) tended to be lower than FA of female subjects (0.55 ± 0.06), although this difference was not statistically significant, p = 0.052 (Fig. 2d). When adjusted to a body weight of 70 kg by simple linear regression, the difference became practically negligible (FAmen(70kg) = 0.54 ± 0.06 vs. FAwomen(70kg) = 0.54 ± 0.05; p = 0.95).
Mean values of MD, RD, and AD, did not significantly differ between men and women, independently of whether weight adjustment was performed.
Mean values of FA, MD, RD, and AD did not show any significant differences that could be attributed to the side (left vs. right) that was chosen for the examination.
Mean FA and age showed a strong negative correlation (r = −0.77, p < 0.001). Mean RD and age were positively associated (r = 0.56, p < 0.001), while mean AD and age were negatively associated (r = −0.40, p = 0.002). Mean MD did not correlate significantly with age (r = 0.15, p = 0.24) (Fig. 3).

Correlation of DTI parameters with age. a Fractional anisotropy (FA) was strongly inversely associated with age. b Correlation of mean diffusivity (MD) with age was not statistically significant. c Radial diffusivity (RD) correlated positively with age. d Axial diffusivity (AD) correlated negatively with age. All DTI metrics are mean values, averages over all analysed nerves. r = Pearson coefficient
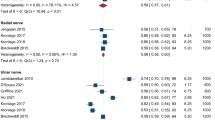
The inverse association of age and FA was not only found for the average value mean FA but also for every single nerve (Fig. 4) with Pearson correlation coefficients ranging from r = −0.47 for the ulnar nerve to r = −0.62 for the radial nerve.

Single nerve analysis: correlation of FA with age. Significant inverse association of fractional anisotropy (FA) with age was found in every analysed nerve. a The sciatic nerve was analysed at mid-thigh. b The tibial nerve was assessed at the proximal third of the lower leg. c Ulnar, d median and e radial nerves were examined at mid upper arm. r = Pearson coefficient
Multiple linear regression model of nerve FA
In light of the associations of nerve FA both with age and (to a lesser extent) with weight, BMI and height described above, we computed a multiple linear regression model with mean FA as the dependent variable. After we applied backward variable selection, age and weight remained as predictors in the model, yielding an R 2 of 0.71. Using a 10-fold cross-validation approach, we obtained a (predictive) R 2 of 0.67. The multiple linear regression model can be described by the formula \( \mathrm{FA}=0.755-\frac{0.0026}{\mathrm{years}}\times \mathrm{age}-\frac{0.0012}{\mathrm{kg}}\times \mathrm{weight} \). The standardized coefficients beta were −0.755 for age and −0.351 for weight.
The formula of this model can be rewritten to adjust any measured DTI parameter FAmeasured, obtained in an individual with a weightmeasured and an agemeasured, to a parameter FAadjusted corresponding to the arbitrarily definable parameters weightto adjust to and ageto adjust to:
Discussion
We here present the results of peripheral nerve DTI in a cohort of 60 healthy volunteers over six decades of life. In addition to the collection of normal values for multiple nerves of both upper and lower extremity, we describe the effects of demographic variables on DTI metrics and propose a correction formula for adjustment of nerve FA.
We identified age as the most important demographic determinant for FA. A strong negative correlation between age and FA was not only found for average values but also in single-nerve analysis for every assessed nerve. Our findings confirm those reported in smaller cohorts for the median nerve at the wrist [4, 5, 27] and the tibial nerve at the lower leg [28]. In contrast to Tanitame et al. [28], who, on the basis of analysis of 26 healthy subjects, proposed FA to be constant below an age of 45 years and to decline only above that age, graphic analysis of our data suggests no such two phases but a linear decline throughout the whole adult lifetime.
FA is the most commonly used DTI readout parameter and regarded as a general biomarker of nerve tissue integrity [16]. Its decrease can be caused both by a decrease of diffusion in fibre orientation (AD) or an increase of diffusion perpendicular to fibre orientation (RD) [15]. Three of the previous studies [4, 27, 28] that described an age-related decline of FA did not specifically assess RD and AD. Hiltunen et al. reported a decrease of both RD and AD in older compared to young controls at certain locations in the carpal tunnel [5]. In contrast to these results, we found that both a reduction of AD and an increase of RD contributed to the observed decrease of FA with advancing age. What might be the reason behind this phenomenon on a histological basis? Decrease of AD is commonly regarded as a marker of axonal neuropathy, whereas increase of RD might reflect myelin sheath damage [3, 30,31,32]. This model is simplified, since diffusion may additionally be modulated by other factors such as oedema [33], but it might still partially explain why both RD increases and AD declines with age. Histologic studies describe a loss of the number of myelinated fibres and in peripheral nerves that is partially compensated by an increase in fibres with thinner myelin sheaths [22, 23, 34]. Electrophysiological studies report both a reduction of the compound muscle action potential and an increase of nerve conduction velocity with increasing age, which is interpreted as a combined axonal and demyelinating damage [35,36,37,38]. Thus, reduction of FA, increase of RD and decrease of AD with age might well reflect this combination of subclinical fibre loss and demyelination.
Since FA was not only associated with age but also to a lesser extent with weight, BMI and height, we computed a multiple linear regression model, which was best with the two predictors age and weight, and proposed a correction formula to adjust FA to age and weight. This formula might be applied and validated in further studies, to correct for differences in demographic variables between study groups, if matching with regards to age and body weight is not feasible.
Another major aim of our study was to determine the influence of sex on DTI parameters. FA tended to be lower in men than in women, albeit slightly missing statistical significance. When adjusting FA to a predefined body weight, the sex-related difference became completely negligible. Our findings are in line with those of Guggenberger et al. [4] and Tanitame et al. [28], who also did not report statistically significant differences in nerve FA, and imply that sex-matching is no longer necessary in future studies of nerve DTI.
A limitation of our study is that DTI metrics, as with all functional imaging parameters, might be influenced by the technical setup and sequence specifications. Until now, differences between certain DTI techniques and hardware systems have been assessed in a few studies [39,40,41], which found that absolute values of readout parameters are generally comparable, with FA as the most stable of the scalar readout parameters reported here [40]. While the absolute values of DTI metrics reported here may have orienting character, the described relationships between demographic variables and DTI metrics are expected to be also valid in different technical setups. Still, further studies that specifically address comparability of DTI in peripheral nerves are needed. Moreover, we suggest a prospective validation of the multiple linear regression model proposed here in different cohorts. Another limitation of our study is that multiple testing was performed. Therefore, the reported p values should be interpreted descriptively.
In conclusion, the findings of peripheral nerve DTI in 60 healthy volunteers presented here provide robust evidence of a linear decline of peripheral nerve FA with increasing age throughout adult lifetime in all analysed nerves. Moreover, FA was moderately inversely associated with weight, BMI and height, while sex-specific differences in FA values were negligible, particularly after normalization to body weight. We propose a correction formula, to adjust FA to age and body weight, that may be used in future studies of peripheral nerve DTI.
References
Filler AG, Howe FA, Hayes CE et al (1993) Magnetic resonance neurography. Lancet 341:659–661
Pham M, Baumer T, Bendszus M (2014) Peripheral nerves and plexus: imaging by MR-neurography and high-resolution ultrasound. Curr Opin Neurol 27:370–379
Heckel A, Weiler M, Xia A et al (2015) Peripheral nerve diffusion tensor imaging: assessment of axon and myelin sheath integrity. PLoS One 10:e0130833
Guggenberger R, Markovic D, Eppenberger P et al (2012) Assessment of median nerve with MR neurography by using diffusion-tensor imaging: normative and pathologic diffusion values. Radiology 265:194–203
Hiltunen J, Kirveskari E, Numminen J et al (2012) Pre- and post-operative diffusion tensor imaging of the median nerve in carpal tunnel syndrome. Eur Radiol 22:1310–1319
Hiltunen J, Suortti T, Arvela S et al (2005) Diffusion tensor imaging and tractography of distal peripheral nerves at 3 T. Clin Neurophysiol 116:2315–2323
Haakma W, Jongbloed BA, Froeling M et al (2017) MRI shows thickening and altered diffusion in the median and ulnar nerves in multifocal motor neuropathy. Eur Radiol 27:2216–2224
Wu C, Wang G, Zhao Y et al (2017) Assessment of tibial and common peroneal nerves in diabetic peripheral neuropathy by diffusion tensor imaging: a case control study. Eur Radiol 27:3523–3531
Breitenseher JB, Kranz G, Hold A et al (2015) MR neurography of ulnar nerve entrapment at the cubital tunnel: a diffusion tensor imaging study. Eur Radiol 25:1911–1918
Jengojan S, Kovar F, Breitenseher J et al (2015) Acute radial nerve entrapment at the spiral groove: detection by DTI-based neurography. Eur Radiol 25:1678–1683
Kronlage M, Pitarokoili K, Schwarz D et al (2017) Diffusion tensor imaging in chronic inflammatory demyelinating polyneuropathy: diagnostic accuracy and correlation with electrophysiology. Invest Radiol 52:701–707
Chhabra A, Madhuranthakam AJ, Andreisek G (2017) Magnetic resonance neurography: current perspectives and literature review. Eur Radiol. https://doi.org/10.1007/s00330-017-4976-8
Basser PJ, Mattiello J, LeBihan D (1994) MR diffusion tensor spectroscopy and imaging. Biophys J 66:259–267
Basser PJ, Mattiello J, LeBihan D (1994) Estimation of the effective self-diffusion tensor from the NMR spin echo. J Magn Reson B 103:247–254
Mori S, Zhang J (2006) Principles of diffusion tensor imaging and its applications to basic neuroscience research. Neuron 51:527–539
O'Donnell LJ, Westin CF (2011) An introduction to diffusion tensor image analysis. Neurosurg Clin N Am 22:185–196 viii
Hagmann P, Jonasson L, Maeder P et al (2006) Understanding diffusion MR imaging techniques: from scalar diffusion-weighted imaging to diffusion tensor imaging and beyond. Radiographics 26:S205–S223
Kasprian G, Amann G, Panotopoulos J et al (2015) Peripheral nerve tractography in soft tissue tumors: a preliminary 3-tesla diffusion tensor magnetic resonance imaging study. Muscle Nerve 51:338–345
Kakuda T, Fukuda H, Tanitame K et al (2011) Diffusion tensor imaging of peripheral nerve in patients with chronic inflammatory demyelinating polyradiculoneuropathy: a feasibility study. Neuroradiology 53:955–960
Simon NG, Lagopoulos J, Paling S et al (2017) Peripheral nerve diffusion tensor imaging as a measure of disease progression in ALS. J Neurol 264:882–890
Breckwoldt MO, Stock C, Xia A et al (2015) Diffusion tensor imaging adds diagnostic accuracy in magnetic resonance neurography. Invest Radiol 50:498–504
Moriyama H, Amano K, Itoh M et al (2007) Morphometric aspects of peripheral nerves in adults and the elderly. J Peripher Nerv Syst 12:205–209
Ugrenovic S, Jovanovic I, Vasovic L et al (2016) Morphometric analysis of the diameter and g-ratio of the myelinated nerve fibers of the human sciatic nerve during the aging process. Anat Sci Int 91:238–245
Dorfman LJ, Bosley TM (1979) Age-related changes in peripheral and central nerve conduction in man. Neurology 29:38–44
Matsumoto H, Konoma Y, Shimizu T et al (2012) Aging influences central motor conduction less than peripheral motor conduction: a transcranial magnetic stimulation study. Muscle Nerve 46:932–936
Cartwright MS, Passmore LV, Yoon JS et al (2008) Cross-sectional area reference values for nerve ultrasonography. Muscle Nerve 37:566–571
Kabakci N, Gurses B, Firat Z et al (2007) Diffusion tensor imaging and tractography of median nerve: normative diffusion values. AJR Am J Roentgenol 189:923–927
Tanitame K, Iwakado Y, Akiyama Y et al (2012) Effect of age on the fractional anisotropy (FA) value of peripheral nerves and clinical significance of the age-corrected FA value for evaluating polyneuropathies. Neuroradiology 54:815–821
Franco CD (2012) Connective tissues associated with peripheral nerves. Reg Anesth Pain Med 37:363–365
Song SK, Sun SW, Ramsbottom MJ et al (2002) Dysmyelination revealed through MRI as increased radial (but unchanged axial) diffusion of water. Neuroimage 17:1429–1436
Song SK, Sun SW, Ju WK et al (2003) Diffusion tensor imaging detects and differentiates axon and myelin degeneration in mouse optic nerve after retinal ischemia. Neuroimage 20:1714–1722
Mac Donald CL, Dikranian K, Bayly P et al (2007) Diffusion tensor imaging reliably detects experimental traumatic axonal injury and indicates approximate time of injury. J Neurosci 27:11869–11876
Lin M, He H, Schifitto G, Zhong J (2016) Simulation of changes in diffusion related to different pathologies at cellular level after traumatic brain injury. Magn Reson Med 76:290–300
Jacobs JM, Love S (1985) Qualitative and quantitative morphology of human sural nerve at different ages. Brain 108:897–924
Stetson DS, Albers JW, Silverstein BA, Wolfe RA (1992) Effects of age, sex, and anthropometric factors on nerve conduction measures. Muscle Nerve 15:1095–1104
Rivner MH, Swift TR, Malik K (2001) Influence of age and height on nerve conduction. Muscle Nerve 24:1134–1141
Kurokawa K, Mimori Y, Tanaka E et al (1999) Age-related change in peripheral nerve conduction: compound muscle action potential duration and dispersion. Gerontology 45:168–173
Awang MS, Abdullah JM, Abdullah MR et al (2006) Nerve conduction study among healthy malays. The influence of age, height and body mass index on median, ulnar, common peroneal and sural nerves. Malays J Med Sci 13:19–23
Filli L, Piccirelli M, Kenkel D et al (2016) Accelerated magnetic resonance diffusion tensor imaging of the median nerve using simultaneous multi-slice echo planar imaging with blipped CAIPIRINHA. Eur Radiol 26:1921–1928
Fox RJ, Sakaie K, Lee JC et al (2012) A validation study of multicenter diffusion tensor imaging: reliability of fractional anisotropy and diffusivity values. AJNR Am J Neuroradiol 33:695–700
Manoliu A, Ho M, Nanz D et al (2016) Diffusion tensor imaging of lumbar nerve roots: comparison between fast readout-segmented and selective-excitation acquisitions. Invest Radiol 51:499–504
Acknowledgements
We are grateful to Thorsten Feiweier from Siemens Healthcare for providing the work-in-progress package which included the DTI sequence that we used for imaging. This study was supported by the Deutsche Forschungsgemeinschaft (SFB 1118).
Funding
S.H. and M.B. were supported by a grant from the German Research Foundation (SFB 1118).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Dr. Moritz Kronlage.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors (Dr. Lorenz Uhlmann) has significant statistical expertise.
Informed consent
Written informed consent was obtained from all subjects (patients) in this study.
Ethical approval
Institutional review board approval was obtained.
Study subjects or cohorts overlap
Normal values of nerve calibre and T2 relaxometry in the same cohort were published separately in Kronlage M, Schwehr V, Schwarz D et al (2017) Normal Values and Demographic Determinants of Nerve Caliber and T2 Relaxometry in 60 healthy individuals. Clin Neuroradiol. [Epub ahead of print] Eighteen of 60 subjects were used in a control group for
1. Kronlage M, Pitarokoili K, Schwarz D et al (2017) Diffusion tensor imaging in chronic inflammatory demyelinating polyneuropathy: diagnostic accuracy and correlation with electrophysiology. Invest Radiol 52:701–7
2. Kronlage M, Baumer P, Pitarokoili K et al (2017) Large coverage MR neurography in CIDP: diagnostic accuracy and electrophysiological correlation. J Neurol 264:1434–43
Methodology
• prospective
• cross-sectional study/observational
• performed at one institution
Rights and permissions
About this article

Cite this article
Kronlage, M., Schwehr, V., Schwarz, D. et al. Peripheral nerve diffusion tensor imaging (DTI): normal values and demographic determinants in a cohort of 60 healthy individuals. Eur Radiol 28, 1801–1808 (2018). https://doi.org/10.1007/s00330-017-5134-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-017-5134-z