
Abstract
Objective
To assess associations between bone marrow infiltration patterns and localization in magnetic resonance imaging (MRI) and baseline clinical/prognostic parameters in multiple myeloma (MM).
Methods
We compared baseline MM parameters, MRI patterns and localization of focal lesions to the mineralized bone in 206 newly diagnosed MM patients.
Results
A high tumour mass (represented by International Staging System stage III) was significantly associated with severe diffuse infiltration (p = 0.015) and a higher number of focal lesions (p = 0.006). Elevated creatinine (p = 0.003), anaemia (p < 0.001) and high LDH (p = 0.001) correlated with severe diffuse infiltration. A salt and pepper diffuse pattern had a favourable prognosis. A higher degree of destruction of mineralized bone (assessed by X-ray or computed tomography) was associated with an increasing number of focal lesions on MRI (p < 0.001). Adverse cytogenetics (del17p/gain1q21/t(4;14)) were associated with diffuse infiltration (p = 0.008). The presence of intraosseous focal lesions exceeding the mineralized bone had a borderline significant impact on prognosis.
Conclusions
Diffuse bone marrow infiltration on MRI correlates with adverse cytogenetics, lowered haemoglobin values and high tumour burden in newly diagnosed MM whereas an increasing number of focal lesions correlates with a higher degree of bone destruction. Focal lesions exceeding the cortical bone did not adversely affect the prognosis.
Key Points
• Diffuse MRI correlates with adverse cytogenetics, lowered haemoglobin and high tumour burden.
• Higher numbers of MRI focal lesions correlate with increasing degree of bone destruction.
• Focal lesions exceeding the cortical bone borderline significantly influence survival.
• Moderate/severe diffuse infiltration and more than 23 focal lesions adversely affect survival.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Magnetic resonance imaging (MRI) is recommended for disease assessment in almost all stages of monoclonal plasma cell disorders [1]. It is able to depict bone marrow infiltration and to distinguish different growth patterns of the disease. The adverse prognostic implications of diffuse infiltration and focal lesions have been demonstrated in asymptomatic as well as symptomatic multiple myeloma (MM) [2–4]. Recently, MRI findings have been included into the revised criteria to define symptomatic MM, and it is recommended to obtain a baseline MRI at any disease stage [5, 6]. In symptomatic MM more than seven focal lesions on axial (ax; MRI of the head, spine and pelvis) MRI are of adverse prognostic significance regarding event-free (EFS) and overall survival (OS) [4, 7].
Recent studies applying axMRI demonstrated a correlation of both clinical and genetic features of MM with MRI findings: Moulopoulos et al. [8, 9] demonstrated that diffuse infiltration in axial MRI correlates with unfavourable cytogenetic aberrations (CAs) as well as advanced stages according to the International Staging System (ISS). Baseline parameters, such as lowered haemoglobin (Hb) value, higher bone marrow plasma cell infiltration (BMPC), higher lactate dehydrogenase levels (LDH) and elevated serum calcium levels correlate with presence of diffuse infiltration [9]. More than seven focal lesions were associated with lowered serum albumin, higher LDH, C-reactive protein (CRP) and serum creatinine [4]. Focal lesions as well as diffuse infiltration on MRI were associated with an increased number of lytic bone lesions detected by X-ray-based metastatic bone survey (MBS) [8].
The current study used whole-body (wb; MRI of the head, spine, pelvis and extremities) MRI to independently (1) analyze the prognostic value of the described focal and diffuse infiltration (including the hitherto poorly investigated diffuse salt and pepper (S&P) infiltration pattern), (2) examine the prognostic value of the localization of focal lesions to the mineralized bone (intraosseous ± exceeding cortical bone), and (3) assess the mutual correlation between diffuse infiltration or the number of focal lesions and unfavourable CA as well as clinical baseline and prognostic parameters.
Materials and methods
Subjects
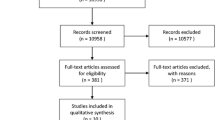
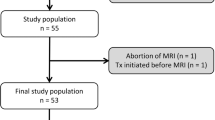
The wbMRI studies of 206 untreated MM patients, which were obtained between June 2004 and March 2010, were retrospectively evaluated. Patients were included if wbMRI had been performed within 0–100 days prior to initiation of systemic treatment (median 13 days, range 0–92 days). Baseline characteristics are shown in Supplemental Table 1. At least one high-dose melphalan therapy and subsequent autologous stem cell transplantation was performed in 160 patients, while the other 46 were transplant-ineligible. Maintenance therapy was performed in 83 patients with interferon (17 patients), thalidomide (47 patients) or bortezomib (19 patients), respectively. This retrospective data analysis was approved by the institutional ethics committee. Parts of the cohort have already been published [7].
Imaging protocol and analysis
Whole-body MRI was performed without the administration of contrast agent on two similar 1.5 Tesla MRI units (Magnetom Avanto, Siemens Healthcare, Erlangen, Germany, duration of MRI scan: approximately 30–45 minutes) and included coronal T1w and short-tau inversion recovery T2w (STIR) sequences from the vertex to the mid-calves as well as sagittal T1w and T2*w (in phase) sequences covering the vertebrae from the atlas to the coccygeal bone. The STIR sequence provides T2w, fat-suppressed images. All MRI scans were read by two experienced investigators in consensus reading as reported previously [3, 10–12].
Focal lesions were defined as circumscribed areas (>5 mm in diameter) with decreased signal intensity in T1w images and increased signal intensity in T2w images [12, 13].
Diffuse bone marrow infiltration in the axial skeleton was assessed according to the criteria proposed by Stäbler and Baur et al. [7, 13] as follows:
A diffuse infiltration pattern (general T1w hypointensity) was subcategorized into moderate (hyperintensity in T1w compared to the intervertebral disc) or severe (T1 shows the same low signal intensity as the intervertebral disc). Furthermore, an S&P pattern (T1w mixed hyper- and hypointense, STIR hypointense) and minimal infiltration pattern (appearing as ‘normal’, fatty-converted bone marrow, with high signal intensity in T1w and low signal intensity in T2w STIR images, called minimal diffuse infiltration, because a minor infiltration of plasma cells is very likely and cannot be ruled out) were defined. If both diffuse and focal involvement were present, both patterns were assessed separately.
Cytogenetic analyses
As previously described, cytogenetic analyses identifying adverse CA (deletion 17p, translocation t(4;14) and gain 1q21 > 3 copies) were performed according to local standards using interphase in-situ hybridization (iFISH) [14].
Statistical analyses
Association between categorical and continuous parameters was tested using Mann-Whitney-Wilcoxon test (two groups) and Kruskal-Wallis test (multiple groups). Fisher’s exact test was used to test the association between categorical parameters. Spearman’s rho was used to assess the correlation between continuous parameters.
Progression-free survival (PFS) was defined as time from MRI to progression or death from any cause, whichever occurred first. OS was defined as the time from MRI to death from any cause. Patients without event were censored at last follow-up. Distribution of event times was estimated by the Kaplan-Meier method. The log- rank test was used to compare survival curves, stratified by transplant-eligibility.
All tests were two-sided. P-values below 0.05 were considered statistically significant. All analyses were performed using the R 3.1 software package (R Core Team, http://www.R-project.org/).
Results
Baseline MRI findings
Minimal diffuse infiltration (normal appearing, fatty-converted bone marrow) was present in 25.2 % (52 patients), moderate diffuse infiltration in 37.9 % (78 patients), severe diffuse infiltration in 27.7 % (57 patients) and S&P diffuse infiltration in 9.2 % (19 patients) of patients.
At least one focal lesion was found in 79.6 % (164 patients) whereas 20.4 % (42 patients) of patients had no focal lesions. Among the patients with at least one focal lesion, 97.6 % (160/164 patients) presented with intraosseous focal lesions, 57.9 % (95/164 patients) with intraosseous focal lesions exceeding the cortical bone (extracortical) and 7.3 % (12/164 patients) with soft tissue (extramedullary) lesions. Notably, in our cohort of symptomatic MM patients soft tissue lesions/extramedullary disease (EMD) always appeared in the presence of other intraosseous focal lesions. Frequencies and co-incidences of focal lesion types are shown in Supplemental Table 2.
There was no correlation between the diffuse infiltration and number of focal lesions (p = 0.38) or a grouped diffuse infiltration according to prognosis (minimal/S&P and moderate/severe) and the number of focal lesions (p = 0.38). Representative images and clinical courses for S&P diffuse infiltration and EMD are presented in Fig. 1.

Representative images of salt and pepper diffuse infiltration and extramedullary myeloma disease. T1w (A) and T2w (B) images of a salt and pepper diffuse infiltration of the vertebra from a 69-year-old male patient. He received an upfront therapy including a bortezomib-based induction therapy and high-dose melphalan with autologous blood stem cell transplantation. Since then, he has remained in complete remission for almost 6 years now. T1w (C) and T2w (D) images of a histologically confirmed extramedullary myeloma disease at the left kidney (red arrows) from a 65-year-old male patient. He was initially diagnosed with multiple myeloma growing primarily outside the bone marrow (lymph nodes at the kidney/stomach, left testicle and next to the left the tibia). The first-line treatment included an induction therapy and subsequent high-dose therapy with autologous stem cell transplantation. He progressed for only 3 months after the initial therapy and died due to therapy-refractory disease only 2 months later
Survival analyses of MRI focal and diffuse infiltration patterns
Median follow-up was 64.8 months, last updated in August 2014, and there were 163 PFS and 77 OS events. Kaplan Meier estimates for minimal, moderate, severe and S&P diffuse infiltration were significantly different for both PFS and OS (Fig. 2A and B; PFS: p = 0.002 and OS: p = 0.05). The S&P diffuse infiltration had the best OS prognosis (Fig. 2B).

Kaplan Meier Plots of diffuse and focal MRI patterns. (A, B) Progression-free survival (PFS) and overall survival (OS) for the different diffuse magnetic resonance imaging (MRI) patterns: salt and pepper (S&P), minimal, moderate and severe. (C, D) PFS and OS for the focal MRI lesions grouped in quartiles. Log-rank p values <0.05 were considered statistically significant
As previously reported, an increasing number of focal lesions was associated with an adverse prognosis, but there was no unique cut-off number of focal lesions to define patients with a poor prognosis [4, 7]. Dividing the total focal lesion number into three groups depending on quartiles (<Q1, Q1-3 and > Q3) led to significant PFS and OS differences (Fig. 2C and D; PFS: p < 0.001 and OS: p = 0.04).
The presence of at least one intraosseous focal lesion had no influence on either PFS or OS (Fig. 3A and B). Similarly, the presence of at least one focal lesion exceeding the cortical bone had a borderline significant influence on PFS and OS (p = 0.10 and p = 0.08, Fig. 3C and D). The presence of primary EMD without connection to the mineralized bone resulted in a significantly shortened PFS (p < 0.001) and OS, though the results for OS did not reach statistical significance (P = 0.14, Fig. 3E and F).

Kaplan Meier Plots of focal lesions according to their relation to the mineralized bone. (A, B) Progression-free survival (PFS) and overall survival (OS) for intraosseous focal lesions (FL, 0 vs. ≥1 FL) detected by magnetic resonance imaging (MRI). (C, D) PFS and OS for focal lesions exceeding the cortical bone (0 vs. ≥1 FL). (E + F) PFS and OS for extramedullary/soft tissue lesions (equivalent to extramedullary disease, 0 vs. ≥1 lesion). Log-rank p values <0.05 were considered statistically significant
Association of MRI diffuse infiltration patterns with baseline clinical and prognostic variables
Categorical (ISS, CRAB criteria (calcium elevation, renal failure, anaemia, bone disease, according to Durie et al. [15]), CA, grouped patterns of osteolyses and LDH above the level of the normal, >ULN) and continuous (BMPC, beta-2-microglobulin (b2MG), Hb, LDH and creatinine) variables were associated with the different diffuse infiltration patterns. The results are shown in Table 1. P values for any overall difference between the investigated parameters and diffuse bone marrow infiltration are depicted in Table 1, whereas p values for specific comparisons between distinct diffuse patterns are stated in the following text.
Minimal diffuse infiltration served as a reference since it reflects signal intensity similar to normal, fatty-converted bone marrow in the MRI. ISS stage III was more frequent among the severe diffuse infiltration (p = 0.015) and S&P patterns, though this was not statistically significant (p = 0.13). Higher b2MG (mg/l) values and BMPC (%) were associated with moderate and severe diffuse infiltration (b2MG: p = 0.01 and p < 0.0001; BMPC: p = 0.04 and p = 0.0002), respectively. S&P was associated with higher b2MG (p = 0.04), but not with an increased BMPC (p = 0.2). Anaemia (haemoglobin < 10 g/dl or >2 g/dl below the lower limit of normal) as well as a lower haemoglobin (g/dl) value significantly correlated with moderate and severe diffuse infiltration (anaemia: p = 0.046 and p = 0.0005; haemoglobin: p = 0.001 and p = <0.001). S&P was also associated with a lowered haemoglobin value (p = 0.02). Renal impairment (defined as creatinine >2 mg/dl) was associated with a severe and S&P pattern (p = 0.06 and p = 0.02, respectively). Accordingly, higher creatinine values (mg/dl) were associated with severe diffuse infiltration (p = 0.003) and reached borderline statistical significance for S&P (p = 0.06). An LDH > ULN (%) was more frequently observed in severe diffuse infiltration and S&P (p = 0.001 and p = 0.03), respectively.
Patients with severe diffuse infiltration were more likely to carry any adverse CA (severe diffuse infiltration 60.8 % vs. minimal diffuse infiltration 32.6 %, p = 0.008). Adverse CAs were also observed more frequently in moderate diffuse infiltration and S&P, though the results did not reach statistical significance (moderate diffuse infiltration 51.5 %, p = 0.055 and S&P 52.9 %, p = 0.16). In detail, deletion 17p was most frequent in S&P (S&P 29.4 % vs. minimal diffuse infiltration 2.2 %, p = 0.004) whereas translocation t(4;14) was not observed in S&P. Gain 1q21 was more frequent in severe diffuse infiltration (severe diffuse infiltration 51.0 % vs. minimal diffuse infiltration 25.5 %, p = 0.01). Frequencies of cytogenetic aberrations for each diffuse infiltration pattern are shown in Table 1.
Association of MRI number of focal lesions with baseline clinical and prognostic variables
A quantitative analysis of focal lesions in correlation with baseline variables was performed. The number of focal lesions was associated with the above-described categorical and continuous variables (Table 2).
The median number of focal lesions was significantly higher in patients with ISS stage III (p = 0.006). Accordingly, there was a significant positive, weak correlation between the number of focal lesions and b2MG values (mg/l, r = 0.19, p = 0.01). Renal impairment was associated with an increased number of focal lesions (vs. no renal impairment, p = 0.005) as well as with higher creatinine levels (r = 0.19, p = 0.01). Bone destruction (at least one lytic lesion) and the degree of bone destruction detected by MBS (no: no osteolyses; minor: up to two osteolyses; major: three or more osteolyses or pathological fractures) were also associated with an increased number of focal lesions (CRAB ‘bone disease’-positive vs. CRAB ‘bone disease’-negative p = 0.006 and MBS osteolyses categories ‘no’ vs. ‘major’ p = <0.0001).
There was no correlation between the number of focal lesions and any adverse CAs (Table 2).
Discussion
The current analysis investigated the associations of baseline clinical and prognostic parameters with different MRI patterns as well as the orientation of focal lesions detected on MRI to the mineralized bone in a cohort of 206 symptomatic MM patients.
Both diffuse infiltration and focal lesions on MRI are distinct MM infiltration patterns associated with differentially pronounced clinical/prognostic parameters and an independent adverse prognostic impact on PFS and OS. Higher numbers of focal lesions on MRI are associated with more extensive destruction of mineralized bone as detected by MBS. Moderate and severe diffuse infiltration correlated with a higher degree of BMPC, lower Hb values and adverse CAs. A high tumour burden, as represented by advanced ISS stage or renal impairment, is associated with both severe diffuse infiltration and a higher number of focal lesions. The S&P pattern, which was found in a small subgroup of patients, is associated with a favourable prognosis despite being correlated with advanced ISS stages and adverse CAs. The association of focal lesions with the mineralized bone (only intraosseous focal lesions or intraosseous focal lesions exceeding the cortical bone) had a borderline significant impact on PFS and OS, while the presence of EMD had.
The previously described adverse impact of diffuse infiltration pattern on PFS as well as OS could be confirmed in our cohort [4, 8, 16]. In addition to the recent qualitative approach we included a grading of diffuse infiltration according to the characteristics suggested by Baur and Staebler [7, 13].
Several studies have demonstrated that bone marrow plasma cell infiltration as well as cellularity are increased in patients with diffuse infiltration [9, 12, 16, 17]. Along with an increased BMPC, lowered Hb levels, increased b2MG and LDH (>ULN) are associated with a diffuse infiltration pattern. Consequently, symptomatic MM patients more often present advanced ISS stages since their BMPC is high [9, 17, 18]. The current study supported these observations and additionally identified a mutual correlation between severe but not moderate diffuse infiltration and renal impairment at diagnosis. In another study, increased destruction of mineralized bone was associated with diffuse infiltration [16]; however, in the present analysis these results could not be confirmed (Table 1). Furthermore, the addition of novel agents improved the outcome of patients with diffuse infiltration [8]. Any adverse CAs as well as gain1q21 were found more frequently among patients with a diffuse infiltration pattern. Together, these factors might partially explain the poor prognosis associated with moderate and severe diffuse infiltration detected by MRI [7, 8].
The S&P pattern has to be discriminated from the variegated and moderate/severe diffuse infiltration patterns [8, 19]. Patients with a S&P pattern, representing a small proportion in our cohort (9.2 %), had a favourable PFS and OS. However, some baseline variables associated with S&P were unfavourable, such as elevated b2MG, ISS stage III, renal impairment and lowered Hb values. Furthermore, the CA deletion 17p occurred in 29.4 % (five of 17 with iFISH analysis) and an LDH (>ULN) in 26.3 % of patients with S&P. This is of particular interest, since a recent analysis from Moreau et al. [20] identified patients with an ISS stage III deletion 17p or translocation t(4;14), and LDH (>ULN) at high risk of early progression-related death. These counterintuitive findings might be explained by the small number of patients with S&P. Further analyses of this rare infiltration pattern might yield interesting findings, since it represents a patchy mixture of normal and infiltrated bone marrow, which is supposed to leave islands of normal hematopoietic or fatty bone marrow right next to plasma cell infiltrates.
More than seven focal lesions in axMRI has been demonstrated to be a reasonable cutoff point for symptomatic transplant-eligible MM to identify patients with unfavourable EFS and OS [4, 7]. This cutoff point was confirmed in our cohort of transplant-eligible MM patients when counting axial focal lesions and applying a subdivision of focal lesions into quartiles. However, our data suggest that a continuously increasing number of focal lesions is associated with an adverse prognosis rather than a distinct number of focal lesions in axMRI or wbMRI [7].
Whether a whole-body MRI or an axial MRI is sufficient in routine clinical practice has to be determined in prospective studies. A retrospective analysis, however, demonstrated that a significant number of focal lesions in the extra-axial skeleton are missed if only axMRI is performed [11].
A higher number of focal lesions might correlate with a higher overall tumour burden. Our results demonstrated that a higher focal lesion number is associated with ISS stage III, higher b2MG values and renal impairment. Accordingly, more than seven focal lesions are associated with lowered serum albumin, higher LDH, C-reactive protein and creatinine values [4, 7]. Another study demonstrated that a higher number of osteolyses was associated with a focal infiltration pattern which we also observed in our recent cohort [8]. It seems reasonable that almost every osteolysis in MM is preceded by focal lesions in MRI if its size is detectable. As reported previously, there was no mutual correlation between adverse CAs, a higher BMPC or lowered Hb values and the number of focal lesions [4, 8]. The fact that neither the presence nor the number of focal lesions was correlated with any adverse CAs in FISH analysis might be another suggestion that cells in and outside focal lesions are genetically different, as described by the Little Rock group recently [21]. Furthermore, angiogenesis appears to be an important underlying pathomechanism in both focal and diffuse infiltration patterns [16, 22, 23].
Limitations of the present analysis are that the evaluation of the diffuse infiltration is limited by the experience of the investigating radiologist. However, the description suggested by the Munich group allows a rather reproducible assessment [13]. The presence of severe diffuse infiltration might limit the identification of focal lesions and therefore the number of focal lesions in these patients may be miscalculated. Furthermore, assessment of diffuse infiltration can be compromised by a delayed fatty conversion of the bone marrow in middle-aged patients as well as reactive changes, e.g. inflammatory processes. Furthermore, categorizing bone marrow infiltration in T1w images and comparing signal intensity with the intervertebral disc might be misleading in cases of degenerative disc disease. Nevertheless, this represents a widely used strategy. Certainly, diffusion-weighted imaging and dynamic contrast enhanced MRI may add additional information to the hitherto applied morphological MRI sequences [23–27], and should be offered to MM patients within prospective imaging studies. However, these techniques are not broadly available in routine clinical practice and are not incorporated in the recent guidelines on MM treatment as compared to morphological MRI sequences [6, 26].
In conclusion, wbMRI is a valuable tool for the assessment of tumour mass, and for prognosis and localization of infiltration of monoclonal plasma cells in patients with symptomatic MM inside and outside the skeleton. An increasing number of focal lesions as well as moderate/severe diffuse infiltration is associated with an adverse prognosis. Focal lesions exceeding the cortical bone have a borderline significant impact on PFS and OS. Baseline disease characteristics and biological features of MM are differentially pronounced in the evaluable MRI patterns: A diffuse infiltration pattern is associated with a poor prognosis and features of advanced disease as well as surrogates of high tumour burden. Moreover, diffuse infiltration is associated with adverse CA. In contrast, a S&P pattern is associated with a favourable prognosis despite its association with unfavourable CAs (namely deletion17p) and adverse disease features.
Abbreviations
- ax:
-
Axial
- b2MG:
-
Beta-2-microglobulin
- BMPC:
-
Bone marrow plasma cell infiltration
- CA:
-
Cytogenetic aberrations
- CRAB:
-
Calcium elevation, renal failure, anaemia, bone disease
- CRP:
-
C-reactive protein
- DCE:
-
Dynamic contrast enhanced
- DWI:
-
Diffusion-weighted imaging
- EFS:
-
Event-free survival
- EMD:
-
Soft tissue lesions/extramedullary disease
- Hb:
-
Haemoglobin
- ISS:
-
International Staging System
- iFISH:
-
Interphase in-situ hybridization
- LCD:
-
Light chain disease
- LDH:
-
Lactate dehydrogenase levels
- MBS:
-
X-ray-based metastatic bone survey
- MRI:
-
Magnetic resonance imaging
- MM:
-
Multiple myeloma
- OS:
-
Overall survival
- PFS:
-
Progression-free survival
- S&P:
-
Salt and pepper
- STIR:
-
Short-tau inversion recovery
- wb:
-
Whole-body
- >ULN:
-
Above the level of normal
References
Dimopoulos MA, Hillengass J, Usmani S et al (2015) Role of magnetic resonance imaging in the management of patients with multiple myeloma: a consensus statement. J Clin Oncol 33:657–664
Hillengass J, Weber M-A, Kilk K et al (2014) Prognostic significance of whole-body MRI in patients with monoclonal gammopathy of undetermined significance. Leukemia 28:174–178
Hillengass J, Fechtner K, Weber M-A et al (2010) Prognostic significance of focal lesions in whole-body magnetic resonance imaging in patients with asymptomatic multiple myeloma. J Clin Oncol 28:1606–1610
Walker R, Barlogie B, Haessler J et al (2007) Magnetic resonance imaging in multiple myeloma: diagnostic and clinical implications. JCO 25:1121–1128
Dimopoulos M, Terpos E, Comenzo RL et al (2009) International myeloma working group consensus statement and guidelines regarding the current role of imaging techniques in the diagnosis and monitoring of multiple Myeloma. Leukemia 23:1545–1556
Rajkumar SV, Dimopoulos MA, Palumbo A et al (2014) International myeloma working group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 15:e538–e548
Mai EK, Hielscher T, Kloth JK et al (2015) A magnetic resonance imaging-based prognostic scoring system to predict outcome in transplant-eligible patients with multiple myeloma. Haematologica 100:818–825
Moulopoulos LA, Dimopoulos MA, Kastritis E et al (2012) Diffuse pattern of bone marrow involvement on magnetic resonance imaging is associated with high risk cytogenetics and poor outcome in newly diagnosed, symptomatic patients with multiple myeloma: a single center experience on 228 patients. Am J Hematol 87:861–864
Moulopoulos LA, Gika D, Anagnostopoulos A et al (2005) Prognostic significance of magnetic resonance imaging of bone marrow in previously untreated patients with multiple myeloma. Ann Oncol 16:1824–1828
Hillengass J, Ayyaz S, Kilk K et al (2012) Changes in magnetic resonance imaging before and after autologous stem cell transplantation correlate with response and survival in multiple myeloma. Haematologica 97:1757–1760
Bäuerle T, Hillengass J, Fechtner K et al (2009) Multiple myeloma and monoclonal gammopathy of undetermined significance: importance of whole-body versus spinal MR imaging. Radiology 252:477–485
Kloth JK, Hillengass J, Listl K et al (2014) Appearance of monoclonal plasma cell diseases in whole-body magnetic resonance imaging and correlation with parameters of disease activity. Int J Cancer. doi:10.1002/ijc.28877
Stäbler A, Baur A, Bartl R et al (1996) Contrast enhancement and quantitative signal analysis in MR imaging of multiple myeloma: assessment of focal and diffuse growth patterns in marrow correlated with biopsies and survival rates. Am J Roentgenol 167:1029–1036
Neben K, Lokhorst HM, Jauch A et al (2012) Administration of bortezomib before and after autologous stem cell transplantation improves outcome in multiple myeloma patients with deletion 17p. Blood 119:940–948
Durie BGM, Harousseau J-L, Miguel JS et al (2006) International uniform response criteria for multiple myeloma. Leukemia 20:1467–1473
Moulopoulos LA, Dimopoulos MA, Christoulas D et al (2010) Diffuse MRI marrow pattern correlates with increased angiogenesis, advanced disease features and poor prognosis in newly diagnosed myeloma treated with novel agents. Leukemia 24:1206–1212
Lecouvet FE, Vande Berg BC, Michaux L et al (1998) Stage III multiple myeloma: clinical and prognostic value of spinal bone marrow MR imaging. Radiology 209:653–660
Ailawadhi S, Abdelhalim AN, Derby L et al (2010) Extent of disease burden determined with magnetic resonance imaging of the bone marrow is predictive of survival outcome in patients with multiple myeloma. Cancer 116:84–92
Baur A, Stäbler A, Nagel D et al (2002) Magnetic resonance imaging as a supplement for the clinical staging system of Durie and Salmon? Cancer 95:1334–1345
Moreau P, Cavo M, Sonneveld P et al (2014) Combination of international scoring system 3, high lactate dehydrogenase, and t(4;14) and/or del(17p) identifies patients with multiple myeloma (MM) treated with front-line autologous stem-cell transplantation at high risk of early MM progression–related death. JCO 32:2173–2180
Waheed S, Mitchell A, Usmani S et al (2013) Standard and novel imaging methods for multiple myeloma: correlates with prognostic laboratory variables including gene expression profiling data. Haematologica 98:71–78
Hillengass J, Wasser K, Delorme S et al (2007) Lumbar bone marrow microcirculation measurements from dynamic contrast-enhanced magnetic resonance imaging is a predictor of event-free survival in progressive multiple myeloma. Clin Cancer Res 13:475–481
Lin C, Luciani A, Belhadj K et al (2010) Multiple myeloma treatment response assessment with whole-body dynamic contrast-enhanced MR imaging. Radiology 254:521–531
Merz M, Moehler TM, Ritsch J et al (2015) Prognostic significance of increased bone marrow microcirculation in newly diagnosed multiple myeloma: results of a prospective DCE-MRI study. Eur Radiol. doi:10.1007/s00330-015-3928-4
Dutoit JC, Vanderkerken MA, Anthonissen J et al (2014) The diagnostic value of SE MRI and DWI of the spine in patients with monoclonal gammopathy of undetermined significance, smouldering myeloma and multiple myeloma. Eur Radiol 24:2754–2765
Dimopoulos MA, Hillengass J, Usmani S et al (2015) Role of magnetic resonance imaging in the management of patients with multiple myeloma: a consensus statement. JCO 33:657–664
Merz M, Ritsch J, Kunz C et al (2015) Dynamic contrast-enhanced magnetic resonance imaging for assessment of antiangiogenic treatment effects in multiple myeloma. Clin Cancer Res 21:106–112
Acknowledgments
The authors thank all participating patients and their families.
The scientific guarantor of this publication is Jens Hillengass, M.D. The authors of this manuscript declare relationships with the following companies outside/unrelated to the submitted work:
Elias Karl Mai reports travel grants from Janssen-Cilag, Celgene, Onyx, and Mundipharma, outside the submitted work; Dirk Hose reports grants from Sanofi, outside the submitted work; Hartmut Goldschmidt reports grants from Janssen-Cilag, grants from Celgene, grants from Novartis, grants from Chugai, personal fees and other support from Janssen-Cilag, personal fees and other support from Celgene, personal fees and other support from Novartis, personal fees and other support from Onyx, personal fees and other support from Millennium, personal fees and other support from Chugai, all outside the submitted work; Jens Hillengass reports grants from Sanofi, outside the submitted work.
This study received funding from the Dietmar-Hopp-Foundation (Germany). One of the authors has significant statistical expertise (Thomas Hielscher). Institutional Review Board approval was obtained: University of Heidelberg (S247/2012). Written informed consent was obtained from all subjects (patients) in this study. Some study subjects or cohorts have been previously reported in: Mai EK, Hielscher T, Kloth JK, et al. (2015) A magnetic resonance imaging-based prognostic scoring system to predict outcome in transplant-eligible patients with multiple myeloma. Haematologica 100:818-825. doi: 10.3324/haematol.2015.124115. Methodology: retrospective, diagnostic or prognostic, experimental, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplemental Table 1
(DOCX 19 kb)
Supplemental Table 2
(DOCX 47 kb)
Rights and permissions
About this article

Cite this article
Mai, E.K., Hielscher, T., Kloth, J.K. et al. Association between magnetic resonance imaging patterns and baseline disease features in multiple myeloma: analyzing surrogates of tumour mass and biology. Eur Radiol 26, 3939–3948 (2016). https://doi.org/10.1007/s00330-015-4195-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-015-4195-0