
Abstract
Objectives
To investigate the role of apparent diffusion coefficient (ADC) as a biomarker reflecting the aggressiveness of upper urinary tract urothelial cell carcinoma (UUT-UCC).
Methods
Thirty-four consecutive patients treated with nephroureterectomy for non-metastatic disease were prospectively enrolled in this study. ADC was compared with clinicopathological variables including Ki-67 labelling index (LI) and cancer-specific survival (CSS).
Results
The overall 3-year CSS rate was 82 % (median follow-up, 36 months). ADC was significantly lower in grade 3 disease than in grades 1–2 disease (P = 0.011) and significantly and inversely correlated with Ki-67 LI (ρ = −0.59, P = 0.0002). Low ADCs (<1.10 × 10−3 mm2/s) were significantly associated with shorter CSS (P = 0.039). Multivariate analysis of preoperative variables identified ADC and MRI-based clinical T stage as independent indicators of shorter CSS; the patients were stratified into high-risk (8 patients with low ADC and at least clinical T3) and low-risk (26 patients with high ADC or not more than clinical T2) groups with 3-year CSS rates of 43 % and 93 % (P = 0.0003).
Conclusions
Our preliminary data suggest the potential role of ADC as a quantitative biomarker reflecting the aggressiveness of UUT-UCC. ADC might be useful for preoperative risk stratification of UUT-UCC patients.
Key Points
• Diffusion-weighted MRI offers new information about the aggressiveness of urinary tract cancers.
• The apparent diffusion coefficient acts as a quantitative biomarker for upper urinary tract cancers.
• ADC inversely correlates with immunohistochemical and histological grading of UUT-UCC.
• ADC offers a prognosis for UUT-UCC patients treated with nephroureterectomy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Upper urinary tract urothelial cell carcinoma (UUT-UCC) is a relatively uncommon malignancy, accounting for approximately 5–7 % of all urothelial cancers [1]. However, UUT-UCC is a potentially lethal and aggressive disease; 40 % of patients have muscle-invasive disease at diagnosis, and nearly one half of patients die within 5 years even though they undergo nephroureterectomy, the definitive surgical therapy for the disease [2–4]. Therefore, it is critical to identify high-risk patients and to give them effective adjunctive therapy to improve their oncological outcomes [5]. Meanwhile, recent studies suggest nephron-sparing, conservative surgery including segmental resection and ureteroscopic ablation as viable options for carefully selected, low-risk UUT-UCC patients [6]. Thus, accurate risk stratification, both after and before surgical therapy, is requisite for decision making in the management of UUT-UCC patients.
Pathological parameters obtained through examination of surgical UUT-UCC specimens, including pathological tumour stage, histological grade, lymph node status and lymphovascular invasion, are well-known prognostic factors [6–10]. To date, however, accurate preoperative risk stratification still remains challenging. Although the introduction of flexible ureteroscopy has enabled tumour biopsy and pathological evaluation of UUT-UCC before surgical therapy, ureteroscopic biopsy grading alone is unlikely to be sufficient to characterise the tumour. Recent studies have demonstrated the limited accuracy of ureteroscopic biopsy grading in UUT-UCC patients, especially in patients with low-grade tumours who were diagnosed on the basis of biopsy [11, 12]. Ureteroscopic biopsy is likely to underestimate histological grade with an upgrading rate at approximately 60 % for ureteroscopic biopsy grade 1–2 tumours [12]. Favaretto et al. have suggested the combined use of the information obtained from ureteroscopy and imaging studies to predict locally advanced, non-organ-confined disease [13].
Application of functional imaging techniques would be another approach to characterising the tumour. Diffusion-weighted magnetic resonance imaging (DW-MRI) is a functional imaging technique that reveals physiological information by quantifying the diffusion of water molecules in tissues [14, 15]. This imaging sequence is a non-invasive technique that does not involve the use of a contrast agent or radiation exposure. The extent of the water molecule diffusion can be quantified as the apparent diffusion coefficient (ADC). Malignant tissues with a lower ADC tend to demonstrate higher signal intensity than the surrounding tissue on a DW-MRI image. This imaging sequence is increasingly used for both detection and qualitative assessment of tumour characteristics, including prediction of the therapeutic response [16]. Recently, the prognostic role of the ADC has been emerging among patients with lymphoma, glioblastoma, head and neck cancer, and non-small cell lung cancer [17–21].
Since the publication of our first report demonstrating the feasibility of DW-MRI for detecting UUT-UCC [22], several studies have confirmed the diagnostic performance of DW-MRI in this disease [23–26]. DW-MRI exhibited excellent diagnostic accuracy for UUT-UCC in combination with T1- and T2-weighted (T1W and T2W) MRI; the sensitivity ranges from 92 to 98 % and the specificity ranges from 81 to 96 %, despite unconvincing diagnostic performance for flat carcinoma in situ (CIS) [23, 26]. ADCs of bladder urothelial cancer (BUC) and UUT-UCC tissues were significantly lower than those of the surrounding normal tissues, accounting for the high signal of the tumour [26, 27]. In BUC, several investigators including us demonstrated a significant and inverse correlation between ADC and histological grade [28–31]. However, this correlation is controversial in the series of UUT-UCC; some reported the presence of significant inverse correlation [23, 26], whereas others did not [24, 32].
In the current prospective study, we investigated the potential associations of ADC with survival after nephroureterectomy and clinicopathological parameters including proliferative potential, which is assessed by evaluating Ki-67 labelling index (LI), in UUT-UCC patients. Our preliminary results suggest that the ADC is a quantitative biomarker reflecting the aggressiveness of UUT-UCC and that the ADC may be useful for preoperative risk stratification of UUT-UCC patients.
Materials and methods
Patients
At a single academic centre between January 2007 and September 2010, multi-sequence MRI including DW-MRI was prospectively performed before any intervention in 52 consecutive patients who were clinically diagnosed with UUT-UCC on the basis of urine cytology, ultrasound and/or CT findings. Fourteen patients were excluded from the study: 5 with metastatic disease, 4 who did not undergo nephroureterectomy, 4 who received neoadjuvant therapy before nephroureterectomy and 1 who received adjuvant therapy. Thus, 38 patients treated with nephroureterectomy alone for non-metastatic UUT-UCC were included in the analysis. An institutional review board approved this study, and written informed consent was obtained from each participant.
MRI
Magnetic resonance imaging was performed using 1.5-T MR system (Intera Achieva; Philips, Best, Netherlands) with a four-channel sensitivity-encoding body coil without breath-holding sequences. The maximal gradient strength was 33 mT/m, and the slew rate was 160 T/m/s. The imaging parameters for DW-MRI with a single shot spin-echo planar imaging sequence were set as follows: repetition time, 5,000 ms; echo time, 65 ms; matrix, 128 × 126/256 × 256 zip; field of view, 35 cm; slice thickness, 5 mm; interslice gap, 0.5 mm; slice number, 24; number of excitations, 8; bandwidth, 1,880 Hz per pixel; 3 different diffusion gradient b values (b = 0, 400 or 800 s/mm2); number of motion probing direction gradients, 3; number of averages, 9; fat suppression, spectral attenuated inversion recovery; and total acquisition time, approximately 3 min 40 s. The MRI protocols in this study consisted of routine T1W- and T2W-MRI and DW-MRI (Figs. 1a and 2a).

Diffusion-weighted (DW)-MRI, apparent diffusion coefficient (ADC) map and histogram of the ADC within a region of interest (ROI) of a 76-year-old man with renal pelvic cancer. a Tumour shows homogeneously high signal intensity (white arrowhead) using DW-MRI with a b value of 800 s/mm2. b An ROI was positioned not extending over the tumour on the ADC map. c Histogram for distribution of the ADC of each pixel within the ROI shows a single prominent peak

Diffusion-weighted (DW)-MRI, apparent diffusion coefficient (ADC) map and histogram of the ADC within a region of interest (ROI) of a 64-year-old woman with renal pelvic cancer. a Tumour shows homogeneously high signal intensity (white arrowhead) using DW-MRI with a b value of 800 s/mm2. b An ROI was positioned not extending over the tumour on the ADC map. c Histogram for distribution of the ADC of each pixel within the ROI shows two peaks
Image analysis
The ADC was calculated using the following formula: ADC = −ln (S/S 0)/(b − b 0), where S 0 and S are the signal intensities, obtained with two different diffusion gradient values (b 0 and b = 400 and 800 s/mm2, respectively). The ADC maps were reconstructed at a workstation (View Forum R4.1, Philips Healthcare), and the ADC of the lesion corresponding to the tumour was calculated to quantitatively analyse the degree of diffusion. A region of interest (ROI) was manually drawn to maximally cover the index tumor on the transverse ADC map at the slice that showed maximal tumour diameter (Figs. 1b and 2b). The ADC of each pixel in the ROI was quantified. The distribution of each pixel’s ADC was charted using a histogram (Figs. 1c and 2c), and the mean and standard deviation (SD) of the ADCs within the ROI were calculated. In this study, the ADC of a tumour represented the mean ADC within the ROI. In a patient with multiple tumours, the ADCs were calculated for the index tumour, which was defined as the tumour with the highest clinical T stage.
T staging and histological grading
T stage was determined according to the 2002 TNM system [33]. For the clinical T stage, UUT-UCC was classified into organ-confined (not more than clinical T2) or locally advanced (at least clinical T3) disease on the basis of T1W- and T2W-MRI findings according to the criteria reported previously [13]. Briefly, tumours radiologically confined within the muscle layer of the upper urinary tract were classified as not more than clinical T2 disease, whereas those extending into the renal sinus fat, renal parenchyma, perirenal fat or periureteral tissues were classified as at least clinical T3 disease. Tumour histological grading was evaluated according to the 1973 World Health Organisation classification [34].
Immunohistochemistry
Paraffin-embedded tissue sections obtained from nephroureterectomy were subjected to immunostaining for Ki-67 in each patient. Immunostaining was performed as previously described [16]. Briefly, after inhibition of endogenous peroxidase, the slides were autoclaved and incubated with Ki-67 antibody (clone MIB-1, Dako, Denmark). After incubation with a horseradish peroxidase-labelled secondary antibody (HISTOFINE Simple Stain MAX PO, Nichirei, Japan), colour was developed using 3,3-diaminobenzidine (Nichirei). The sections were counterstained with haematoxylin. Negative controls were included by replacing the primary antibody with phosphate-buffered saline. The Ki-67 LI was calculated as the percentage of tumour cells that were positive for nuclear Ki-67 expression when more than 1,000 tumour cells (×400 magnification) were counted by one of the authors (S.K.), who was blinded to the clinicopathological data.
Follow-up
Patients were followed essentially every 3 months over the first 2 years, every 6 months over the next 3 years, and annually thereafter. Basically, evaluations included complete blood counts, blood chemistry, urinalysis, urine cytology, cystoscopy and CT of the chest, abdomen and pelvis. The median follow-up period was 33 months (range, 7–65 months).
Statistical analysis
Differences between groups were assessed using the Wilcoxon test for continuous variables. Concordance between clinical and pathological T staging was calculated using kappa statistics. Correlations between the mean ADC and the Ki-67 LI were analysed using the Spearman’s rank correlation test. Martingale residual analysis was performed to evaluate the functional form of mean ADC to be used in a Cox proportional hazards model.
Cancer-specific survival (CSS) was estimated and analysed using the Kaplan–Meier method and log-rank test. The prognostic role of ADC was investigated by examining associations of ADC with CSS. Factors related to CSS were analysed using the Cox proportional hazards model, wherein age was divided into two groups at the median of the patients. Tumour location was categorised into renal pelvis or ureter. A cut-off ADC was determined to separate CSS curves of the low and high ADC groups most significantly. Ki-67 LI was classified into high and low groups according to a previously reported cut-off value of 30 % [35]. The CSS duration was defined as the interval from the date of UUT-UCC diagnosis to the date of last follow-up or cancer-specific death. These statistical analyses were performed using JMP 7.0 statistical software (SAS Institute, Cary, NC, USA) and the R statistical package 2.15.0 (The R Foundation for Statistical Computing, 2012, Vienna, Austria), and P values less than 0.05 were considered statistically significant.
Results
Patient and tumour characteristics
Of the 38 patients, 26 (68 %) and 12 patients (32 %) were diagnosed as having not more than clinical T2 and at least clinical T3 disease, respectively. In 4 patients with not more than clinical T2 disease, cancerous lesions did not form a mass and were pathologically diagnosed as primary CIS on the basis of nephroureterectomy specimens. These 4 patients were excluded from the analysis because it was not possible to position an ROI to measure the ADC. The patient and tumour characteristics of the 34 eligible patients are described in Table 1. In all of the patients, histopathological diagnosis was urothelial carcinoma. Of the 17 patients with pathological T3–4 disease, 6 patients were understaged as having not more than clinical T2 disease, whereas 1 of the 17 patients with pathological Ta-2 was overstaged as having at least clinical T3 disease. The concordance between clinical and pathological T staging was moderate (κ = 0.69). The surgical margin was negative in all of the patients. Regional lymph node dissection was performed in 14 patients and no metastasis was found histologically.
Characteristics of the ADC in UUT-UCC
In most cases, UUT-UCC appeared as a homogeneous mass with high signal intensity in DW-MRI. Homogeneity of ADC values was assessed on histograms. We objectively evaluated homogeneity of ADC in UUT-UCC. Histogram analyses of intratumoral ADC showed a single prominent peak in 28 patients (82 %, Fig. 1c) and two or more peaks in 6 patients (18 %, Fig. 2c). The mean UUT-UCC ADC ranged from 0.67 × 10−3 to 1.59 × 10−3 mm2/s (median, 0.98 × 10−3 mm2/s) and the ADC SD for each UUT-UCC ranged from 0.04 × 10−3 to 0.41 × 10−3 mm2/s (median, 0.13 × 10−3 mm2/s).
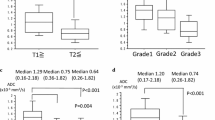
Of age, gender, tumour location, clinical and pathological T stage, and histological grade, the ADC was significantly associated with the histological grade (Table 2); the ADC was significantly lower in grade 3 disease than grades 1–2 disease (median, 0.90 × 10−3 mm2/s vs. 1.20 × 10−3 mm2/s; P = 0.011).
Association between ADC and tumour proliferative activity
We evaluated the association between the ADC and UUT-UCC proliferative activity. The Ki-67 LI of UUT-UCC ranged from 4.1 to 44.2 % (median, 28.7 %) and 14 (41 %) and 20 (59 %) patients were classified into high and low Ki-67 LI groups, respectively. The ADC was significantly lower in the high Ki-67 LI group (median, 0.86 × 10−3 mm2/s) than in the low Ki-67 LI group (median, 1.29 × 10−3 mm2/s; P = 0.0009: Table 2). As shown in Fig. 3, the ADC was significantly and inversely correlated with the Ki-67 LI (ρ = −0.59, P = 0.0002).

Correlation between the ADC and Ki-67 labelling index (LI). a T2W-MRI, DW-MRI, ADC map and Ki-67 immunostaining of upper urinary tract urothelial cell carcinoma (UUT-UCC) in the low (upper panels) and high (lower panels) ADC groups. The cut-off ADC was set at 1.1 × 10−3 mm2/s. Both tumours show similar signal intensity on T2W-MRI. The DW-MRI signal, the ADC of these tumours and Ki-67 LI are different in these tumours. Original magnification for Ki-67 immunostaining, x200. b ADC inversely correlated with Ki-67 LI. Open and closed circles indicate patients with Ta-2 and T3-4 tumours, respectively
Cancer-specific survival
Six patients (15 %) died of UUT-UCC during follow-up. The median time to cancer-specific death was 21 months (range, 16–33 months). The median follow-up period for survivors was 36 months (range, 7–65 months). The overall 3-year CSS rate was 82 %.
Cancer-specific survival was significantly shorter in patients in the high Ki-67 LI group than in those in the low Ki-67 LI group (3-year CSS rate, 61 % vs. 100 %, respectively; P = 0.0080).
Role of ADC as a preoperative prognostic biomarker
The ADC was fitted to a Cox regression model without the covariate of interest, and the functional shape was checked using a smoothed Martingale residual plot. The Martingale residual analysis revealed that the prognostic effect of the ADC on CSS fitted a linear model. There was no abrupt increase in the hazard ratio for CSS. At the cut-off ADC determined at 1.10 × 10−3 mm2/s, 20 (59 %) and 14 patients (41 %) were classified into the low and high ADC groups, respectively. Patients in the low ADC group showed significantly higher Ki-67 LI than those in the high ADC group (P = 0.0008). In the low ADC group there was more grade 3 disease and patients were older than in the high ADC group, although the difference was not statistically significant (P = 0.071 and 0.082, respectively; Table 3). As shown in Fig. 4a, CSS curves were stratified according to the ADC; the 3-year CSS rate was 69 % for the low ADC group and 100 % for the high ADC group (P = 0.039).

Kaplan–Meier analysis in UUT-UCC patients treated with nephroureterectomy. a Cancer-specific survival (CSS) curves stratified by ADC at the cut-off value of 1.1 × 10−3 mm2/s. b CSS curves stratified by the ADC combined with clinical T stage. The number of patients at risk is shown on the horizontal axis at 0 and 36 months
On univariate analysis, the ADC and clinical T stage were identified as significant prognostic factors among preoperative variables that included age, sex, tumour location, clinical T stage, and ADC (P = 0.013 and 0.024, respectively; Table 4). Multivariate analysis revealed that a low ADC (<1.10 × 10−3 mm2/s) and at least clinical T3 disease were significant and independent risk factors for cancer-specific death with respective hazard ratios (HR) of 8.5 × 106 (P = 0.017) and 8.1 (P = 0.031), respectively (Table 4). When these two preoperative risk factors were combined, the 34 patients were stratified into high-risk (low ADC and clinical T3–4, n = 8) and low-risk (high ADC or clinical Ta-2, n = 26) groups for CSS; patients in the high-risk group had a 3-year CSS of 43 %, whereas those in the low-risk group had a 3-year CSS of 93 % (P = 0.0003, Fig. 4b).
Discussion
The current study demonstrated significant and inverse correlations of ADC with Ki-67 LI as well as histological grade in UUT-UCC. Although the results were preliminary, we demonstrated that the patients with UUT-UCC of lower ADC value are at higher risk of cancer-specific death after nephroureterectomy. These results suggest that ADC is a quantitative biomarker reflecting the aggressiveness of UUT-UCC. In this study, UUT-UCC patients were stratified into high-risk and low-risk groups according to a combination of ADC and MRI-based clinical T stage. Although confirmatory studies are mandatory, ADC might be useful for preoperative risk stratification of UUT-UCC.
Malignant tumours have higher cellularity and tissue disorganisation compared with normal tissue, which is believed to be the underlying mechanism for the low ADC observed in malignant tumours compared with normal tissue. However, some recent reports including ours have shown that the functional and biological properties of malignant tumours play an important role in the restricted diffusion of water molecules [15, 16, 26, 29]. We have shown that ADC is inversely correlated with histological grade in BUC and UUT-UCC [26, 29], T stage in BUC [29] and Ki-67 LI in muscle-invasive BUC [16]. The present study confirmed the inverse correlation between the ADC and both the Ki-67 LI and histological grade in UUT-UCC, strengthening the proposal that the ADC is a potential biomarker that reflects the tumour proliferative activity and histological grade. Moreover, a lower ADC was associated with a shorter CSS in UUT-UCC patients treated with nephroureterectomy. Overall, ADC is considered to be a quantitative biomarker that reflects the aggressiveness of urothelial carcinomas.
Although the results were preliminary, the present study demonstrated that ADC and clinical T stage were independent prognostic indicators of UUT-UCC, and suggested that a subset of patients at high risk may be preoperatively identified by the combined use of these two variables. Because these variables are assessed at the same time in one MRI examination, multi-sequence MRI might be a promising tool for preoperative risk stratification of UUT-UCC patients. Incorporation of histopathological information obtained from a ureteroscopic biopsy into the MRI-based variables might further improve the preoperative risk stratification of UUT-UCC patients.
Although multidetector computed tomography using radiocontrast agents is widely used to evaluate UUT-UCC, it is ideal for minimising the use of potentially nephrotoxic, ionising contrast agents for UUT-UCC patients who often have renal insufficiency because of obstructive uropathy. DW-MRI does not require contrast agents and thus it can be used in patients with renal insufficiency. In addition, DW-MRI requires only a few minutes to complete during a routine MRI examination when performed using the most current clinical MRI systems. DW-MRI can be also applied to various phases of urothelial carcinoma patient management including diagnosis, and predicting and monitoring treatment outcomes [16, 36]. Its methodological simplicity, non-invasiveness and objectivity strengthen the routine clinical use of DW-MRI with the quantitative ADC assessment for urothelial cancer patients.
The present study has some limitations. First, this study has a small sample size with relatively short follow-up periods. To validate the current results, further prospective studies using larger patient cohorts with longer follow-up periods are mandatory. Second, the cut-off ADC proposed in this study is not universally applicable because the ADC depends on the MRI systems and imaging conditions used, which is an intrinsic matter in the ADC measurement. Thus, standardisation of the imaging systems and conditions is required. To begin standardising the ADC, we propose to use the mean ADC calculated on one representative slice as an index parameter of the diffusion environment in the whole UUT-UCC. The single prominent peak histogram pattern in most cases and the relatively small SD for each lesion indicated that the degrees of diffusion were homogeneous in most UUT-UCC tissues. The intratumoral homogeneity of ADC may justify using the mean ADC within an ROI as an index parameter for the diffusion of UUT-UCC tissues. Lack of confirmation of reliability and reproducibility of measuring ADC is another limitation of this study. Intra- and interobserver variability in ADC measurement needs to be evaluated in future studies.
In conclusion, the present preliminary data suggest that the ADC serves as a quantitative biomarker reflecting the aggressiveness of upper urinary tract urothelial cell carcinoma. Although confirmatory studies are mandatory, ADC might be useful for preoperative risk stratification.
Abbreviations
- ADC:
-
apparent diffusion coefficient
- CSS:
-
cancer-specific survival
- DW-MRI:
-
diffusion-weighted MRI
- UUT-UCC:
-
upper urinary tract urothelial cell carcinoma
References
Schmauz R, Cole P (1974) Epidemiology of cancer of the renal pelvis and ureter. J Natl Cancer Inst 52:1431–1434
Abouassaly R, Alibhai SM, Shah N, Timilshina N, Fleshner N, Finelli A (2010) Troubling outcomes from population-level analysis of surgery for upper tract urothelial carcinoma. Urology 76:895–901
Hall MC, Womack S, Sagalowsky AI, Carmody T, Erickstad MD, Roehrborn CG (1998) Prognostic factors, recurrence, and survival in transitional cell carcinoma of the upper urinary tract: a 30-year experience in 252 patients. Urology 52:594–601
Olgac S, Mazumdar M, Dalbagni G, Reuter VE (2004) Urothelial carcinoma of the renal pelvis: a clinicopathologic study of 130 cases. Am J Surg Pathol 28:1545–1552
Brown GA, Busby JE, Wood CG et al (2006) Nephroureterectomy for treating upper urinary tract transitional cell carcinoma: time to change the treatment paradigm? BJU Int 98:1176–1180
Roupret M, Zigeuner R, Palou J et al (2011) European guidelines for the diagnosis and management of upper urinary tract urothelial cell carcinomas: 2011 update. Eur Urol 59:584–594
Chromecki TF, Bensalah K, Remzi M et al (2011) Prognostic factors for upper urinary tract urothelial carcinoma. Nat Rev Urol 8:440–447
Hong B, Park S, Hong JH, Kim CS, Ro JY, Ahn H (2005) Prognostic value of lymphovascular invasion in transitional cell carcinoma of upper urinary tract. Urology 65:692–696
Kikuchi E, Horiguchi Y, Nakashima J et al (2005) Lymphovascular invasion independently predicts increased disease specific survival in patients with transitional cell carcinoma of the upper urinary tract. J Urol 174:2120–2123, discussion 2124
Saito K, Kawakami S, Fujii Y, Sakura M, Masuda H, Kihara K (2007) Lymphovascular invasion is independently associated with poor prognosis in patients with localized upper urinary tract urothelial carcinoma treated surgically. J Urol 178:2291–2296, discussion 2296
Smith AK, Stephenson AJ, Lane BR et al (2011) Inadequacy of biopsy for diagnosis of upper tract urothelial carcinoma: implications for conservative management. Urology 78:82–86
Wang JK, Tollefson MK, Krambeck AE, Trost LW, Thompson RH (2012) High rate of pathologic upgrading at nephroureterectomy for upper tract urothelial carcinoma. Urology 79:615–619
Favaretto RL, Shariat SF, Savage C et al (2011) Combining imaging and ureteroscopy variables in a preoperative multivariable model for prediction of muscle-invasive and non-organ confined disease in patients with upper tract urothelial carcinoma. BJU Int 109:77–82
Koh DM, Collins DJ (2007) Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol 188:1622–1635
Padhani AR, Liu G, Koh DM et al (2009) Diffusion-weighted magnetic resonance imaging as a cancer biomarker: consensus and recommendations. Neoplasia 11:102–125
Yoshida S, Koga F, Kobayashi S et al (2012) Role of diffusion-weighted magnetic resonance imaging in predicting sensitivity to chemoradiotherapy in muscle-invasive bladder cancer. Int J Radiat Oncol Biol Phys 83:e21–e27
Berrak S, Chawla S, Kim S et al (2011) Diffusion weighted imaging in predicting progression free survival in patients with squamous cell carcinomas of the head and neck treated with induction chemotherapy. Acad Radiol 18:1225–1232
Ohno Y, Koyama H, Yoshikawa T et al (2012) Diffusion-weighted MRI versus 18F-FDG PET/CT: performance as predictors of tumor treatment response and patient survival in patients with non-small cell lung cancer receiving chemoradiotherapy. AJR Am J Roentgenol 198:75–82
Pope WB, Lai A, Mehta R et al (2011) Apparent diffusion coefficient histogram analysis stratifies progression-free survival in newly diagnosed bevacizumab-treated glioblastoma. AJNR Am J Neuroradiol 32:882–889
Srinivasan A, Chenevert TL, Dwamena BA et al (2012) Utility of pretreatment mean apparent diffusion coefficient and apparent diffusion coefficient histograms in prediction of outcome to chemoradiation in head and neck squamous cell carcinoma. J Comput Assist Tomogr 36:131–137
Wieduwilt MJ, Valles F, Issa S et al (2012) Immunochemotherapy with intensive consolidation for primary CNS lymphoma: a pilot study and prognostic assessment by diffusion-weighted MRI. Clin Cancer Res 18:1146–1155
Yoshida S, Masuda H, Ishii C, Saito K, Kawakami S, Kihara K (2008) Initial experience of functional imaging of upper urinary tract neoplasm by diffusion-weighted magnetic resonance imaging. Int J Urol 15:140–143
Akita H, Jinzaki M, Kikuchi E et al (2011) Preoperative T categorization and prediction of histopathologic grading of urothelial carcinoma in renal pelvis using diffusion-weighted MRI. AJR Am J Roentgenol 197:1130–1136
Nishizawa S, Imai S, Okaneya T, Nakayama T, Kamigaito T, Minagawa T (2010) Diffusion weighted imaging in the detection of upper urinary tract urothelial tumors. Int Braz J Urol 36:18–28
Takeuchi M, Suzuki T, Sasaki S et al (2012) Clinicopathologic significance of high signal intensity on diffusion-weighted MR imaging in the ureter, urethra, prostate and bone of patients with bladder cancer. Acad Radiol 19:827–833
Yoshida S, Masuda H, Ishii C et al (2011) Usefulness of diffusion-weighted MRI in diagnosis of upper urinary tract cancer. AJR Am J Roentgenol 196:110–116
Matsuki M, Inada Y, Tatsugami F, Tanikake M, Narabayashi I, Katsuoka Y (2007) Diffusion-weighted MR imaging for urinary bladder carcinoma: initial results. Eur Radiol 17:201–204
Daggulli M, Onur MR, Firdolas F, Onur R, Kocakoc E, Orhan I (2011) Role of diffusion MRI and apparent diffusion coefficient measurement in the diagnosis, staging and pathological classification of bladder tumors. Urol Int 87:346–352
Kobayashi S, Koga F, Yoshida S et al (2011) Diagnostic performance of diffusion-weighted magnetic resonance imaging in bladder cancer: potential utility of apparent diffusion coefficient values as a biomarker to predict clinical aggressiveness. Eur Radiol 21:2178–2186
Takeuchi M, Sasaki S, Ito M et al (2009) Urinary bladder cancer: diffusion-weighted MR imaging–accuracy for diagnosing T stage and estimating histologic grade. Radiology 251:112–121
Avcu S, Koseoglu MN, Ceylan K, Bulut MD, Unal O (2011) The value of diffusion-weighted MRI in the diagnosis of malignant and benign urinary bladder lesions. Br J Radiol 84:875–882
Sufana Iancu A, Colin P, Puech P et al (2012) Significance of ADC value for detection and characterization of urothelial carcinoma of upper urinary tract using diffusion-weighted MRI. World J Urol. doi:10.1007/s00345-012-0945-7
Sobin LHWC (2002) TNM classification of malignant tumours, 6th edn. Wiley-Liss, New York
WHO (1988) International histological classification of tumours, 2nd edn. Springer, Berlin
Kamai T, Takagi K, Asami H, Ito Y, Arai K, Yoshida KI (2000) Prognostic significance of p27Kip1 and Ki-67 expression in carcinoma of the renal pelvis and ureter. BJU Int 86:14–19
Yoshida S, Koga F, Kawakami S et al (2010) Initial experience of diffusion-weighted magnetic resonance imaging to assess therapeutic response to induction chemoradiotherapy against muscle-invasive bladder cancer. Urology 75:387–391
Conflict of interest
None of the authors has any potential conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Soichiro Yoshida and Shuichiro Kobayashi contributed equally to this article.
Of the 52 patients included in this study, 40 were included in our analysis of the diagnostic ability of DW-MRI to detect upper urinary tract cancer reported elsewhere (AJR Am J Roentgenol 196:110–116 2011).
Rights and permissions
About this article
Cite this article
Yoshida, S., Kobayashi, S., Koga, F. et al. Apparent diffusion coefficient as a prognostic biomarker of upper urinary tract cancer: a preliminary report. Eur Radiol 23, 2206–2214 (2013). https://doi.org/10.1007/s00330-013-2805-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-013-2805-2