
Abstract
The aim of this study was to evaluate the value of use of multidetector CT (MDCT) to predict the need for subsequent surgery in patients with small-bowel obstruction (SBO) due to adhesion. During a 3-year period, 128 patients with an SBO due to adhesion were enrolled in this prospective study. Initially, all patients were treated conservatively. Surgery was performed in patients who developed signs of strangulation or did not improve, despite a conservative treatment for at least 5 days. Of the 128 patients, 37 patients eventually underwent surgery. Two radiologists interpreted MDCT findings regarded as predictive indicators for subsequent surgery in consensus. The findings included degree of SBO, presence of transition zone, and an abnormal vascular course. These findings were statistically compared between the group operated on and the group not operated on. A higher degree of SBO, an abnormal vascular course, and the presence of transition zone were more frequently seen in the group of patients operated on (p < 0.001). Sensitivities, specificities, positive and negative predictive values, and risks for the use of MDCT to predict the need for surgery were 100%, 46.1%, 43%, 100%, and 1.9 (1.5 ≤ 95% confidence interval (CI) ≤ 2.2) for a high-grade obstruction; 100%, 23%, 34.5%, 100%, and 1.3 (1.2 ≤ 95% CI ≤ 1.5) for the presence of a transition zone; and 70.2%, 90.1%, 74.2%, 88.1%, and 7.1 (3.7 ≤ 95% CI ≤ 13.7) for the presence of an abnormal course of the mesenteric vessels, respectively. The presence of a high degree of SBO and an abnormal vascular course around transition zone are useful indicators on MDCT to predict the need for surgery in patients with an SBO due to adhesion.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Small-bowel obstruction (SBO) is a common surgical condition accounting for as many as 12–16% of surgical admissions annually [1–6]. Recently, it has been generally accepted that patients with an SBO should be aggressively resuscitated during a 12- to 24-h period, except when the patient is in frank septic shock [2, 3, 5]. However, there has been a debate on the role of early surgery versus a trial of nonoperative management in patients with an SBO [2, 3, 5, 7–9]. It is difficult to select the proper time for surgery based only on clinical symptoms that do not accurately predict strangulation for patients with an SBO who have equivocal clinical findings [2, 3, 5, 8, 10]. A decision to undergo surgery for an SBO may shorten hospitalization and promote better recovery.
In general, patients with an SBO who have definite clinical and radiological findings of strangulation or perforation usually undergo surgery without hesitation [2, 3, 5, 10, 11]. However, in patients with equivocal findings, a prediction of the need for subsequent surgery is essential to make a treatment plan and to prevent a delay.
The purpose of this study was to prospectively evaluate the role of the use of multidetector computed tomography (MDCT) to predict the need for subsequent surgery in patients with an SBO due to adhesion.
Materials and methods
Patients
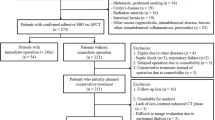
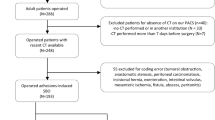
During a 3-year period from March 2005 to March 2008, 136 patients were enrolled in the prospective study. Patients who satisfied all of the following conditions, as seen on MDCT, were enrolled: (1) an SBO was present, (2) the SBO was due to adhesion, which was suggested by the absence of a distinct cause of such as a tumor or hernia, (3) absence of mesenteric torsion showing a so-called whirl sign, because an operation would be considered to represent a source of selection bias, (4) the absence of strangulation or perforation of small bowel. Eight patients dropped out of the study and did not undergo follow-up. Finally, 128 patients were candidates for the analysis. The patients were aged from 12 to 90 years (mean age 55.5 years) and consisted of 55 women and 73 men. Initially, all patients were treated conservatively.
MDCT imaging protocol
CT examinations were performed using a 16-MDCT machine (SOMATOM Sensation, Siemens Medical Solutions, Forchheim, Germany) for 118 patients and a 64-MDCT machine (SOMATOM Sensation 64, Siemens Medical Solutions) for ten. MDCT images were obtained from the diaphragm to the symphysis pubis during a single breath-hold with a detector configuration of 1.5 mm × 16 and a table speed of 24 mm per gantry rotation for 16-MDCT, a detector configuration of 0.6 mm × 32 with a Z-flying spot system and a table speed of 38.4 mm per gantry rotation for 64-MDCT, a pitch of 1, a reconstruction thickness of 5 mm, 120 kVp and variable tube current (90–140 mA s) for both MDCT machines. No oral contrast agent was administered. Single-phase contrast-enhanced images were obtained at 90 or 100 s after the injection of 120 mL of contrast material (Iohexol, Omnipaque 300, Nycomed; Iopromid, Ultravist 300, Schering) at a rate of 3 mL/s.
Image analysis
Two radiologists interpreted the MDCT findings regarded as predictive indicators for subsequent surgery in consensus. The findings included the degree of obstruction (complete, incomplete high, incomplete low), the presence of the transition zone, and the presence of an abnormal course of the mesenteric vessels around the transition zone. The findings were defined as follows.
-
1.
Degrees of obstruction
-
a.
Complete obstruction was defined as a discrepancy of the luminal diameter between the proximal and distal small bowel adjacent to the transitional zone of more than three times with collapse of the distal small bowel and colon.
-
b.
Incomplete high-grade obstruction was defined as a discrepancy of the luminal diameter between the proximal and distal small bowel adjacent to the transitional zone of more than three times with a small amount of passage of air or fluid into the distal small bowel. There was no or little passage of air or fluid into the ascending colon.
-
c.
Incomplete low-grade obstruction was defined as a discrepancy of the luminal diameter between the proximal and distal small bowel adjacent to the transitional zone of less than three times with the passage of air or fluid into the distal small bowel and the ascending colon [12, 13]. The use of discrepancy of more or less than three times was our own criterion.
-
a.
-
2.
Presence of the transition zone
The transition zone was defined as the point of change in the calibre of the intestinal lumen from a distended segment proximal to the site of the obstruction to a segment that was decreased in calibre or collapsed distal to the obstruction [4, 6, 12, 13]. The presence of transition zone was recorded as “yes” or “no”.
-
3.
Presence of mesenteric vessels with an abnormal course
The mesenteric vascular course was considered unusual if there were vessels converging to one area around the transition zone. We separately recorded a “mesenteric torsion” that was seen with a so-called whirl sign, i.e., where both mesenteric vessels and bowel loops are twisted together and the bowel loops in the whirl show luminal narrowing with a “beak” appearance. Patients with this type of mesenteric torsion were not enrolled in this study as its detection might increase the chance of subsequent surgery representing a source of bias [2, 4–6, 11, 14–17]. Strangulation was considered when the MDCT images showed poor or no contrast enhancement of the bowel wall. In this study, patients with strangulation were not enrolled to minimize selection bias, as radiological strangulation for an SBO is already generally accepted as a sufficient criterion for the patient to be a surgical candidate [1, 2, 4–7, 11, 13, 15, 16, 18].
Clinical indications for surgery
In this study, the clinical indications for surgery were decided by the following indications.
-
1.
Appearance of clinical and radiological findings of bowel perforation demonstrated during conservative treatment.
-
2.
Development of classic signs of strangulation, including one or more of the following: localized tenderness, fever (>38.5°C), tachycardia (>100 beats/min), or leukocytosis (>10,000 WBC/µL) during conservative treatment.
-
3.
Absence of symptomatic improvement or aggravation of obstructive symptoms despite conservative treatment for at least 5 days [2, 3, 5, 19].
Statistical analysis
Each finding was compared statistically between the group of patients that underwent surgery (operated on) and the group of patients that did not undergo surgery (not operated on). MDCT criteria for determining the need for subsequent surgery in patients with an SBO were complete or incomplete high-grade obstruction, the presence of the transition zone, or an abnormal course of vascular structures. Sensitivities, specificities, positive predictive values (PPVs), negative predictive values (NPVs), and risks for the MDCT criteria for the need for surgery in patients with an SBO were calculated.
The χ 2 or Fisher’s exact test was used to determine whether each variable differed significantly between the groups operated on and not operated on. Statistically significant differences were defined as having p values less than 0.05 and all statistical analyses were performed by using SPSS software (SPSS for Windows, version 12.0, SPSS, Chicago, IL USA).
Results
Thirty-seven of the 128 patients underwent surgery. The interval between the onset of symptoms and surgery was 0–22 days (mean time 5.5 days). No patients developed a bowel perforation during conservative treatment. Twenty-six patients underwent surgery due to a sudden onset of continuous abdominal pain and leukocytosis during conservative treatment for less than 5 days. Eleven of the 37 patients had aggravated symptoms despite conservative treatment for more than 5 days. None of the patients who underwent surgery underwent follow-up CT before surgery. Segmental resection of the small bowel was performed for 16 of the 37 patients and adhesiolysis was performed for 21 patients. Pathological examination of the surgical specimens demonstrated the presence of a transmural infarct in 10 of the 16 patients who underwent segmental resection of the small bowel. Microperforation was demonstrated in six of the ten patients. There was no evidence of bowel perforation or strangulation as seen on MDCT for these patients. However, there were high degrees of SBO (complete and incomplete high grade) and an abnormal course of the mesenteric vessels on MDCT for all of the patients.
In the group of patients operated on (n = 37), 22 patients had a complete and 15 had an incomplete high-grade SBO as depicted on MDCT (Figs. 1 and 2). In the group of patients not operated on (n = 91), six patients had a complete SBO (Fig. 3), 43 patients had an incomplete high-grade SBO, and 42 patients had an incomplete low-grade SBO. The presence of the transition zone as seen on MDCT was determined for all of the patients in the group operated on, but for only 46 patients in the group not operated on. An abnormal course of the mesenteric vessels was present in 26 patients as seen on MDCT in the group of patients operated on and nine patients in the group not operated on (Table 1). A high-grade obstruction, the presence of the transition zone, and an abnormal course of the mesenteric vessels were more common in the group of patients operated on than in the group not operated on, which was statistically significant (p < 0.001).

A 65-year-old man with small bowel-obstruction. a,b Contiguous axial MDCT images show the complete degree of obstruction with the transition zone (black arrows) and an abnormal course of mesenteric vessels (white arrows). The patient underwent surgery on the fifth day of admission because of leukocytosis and progressing abdominal pain despite the conservative treatment. Double arrows luminal diameter, C colon

A 46-year-old woman with small-bowel obstruction. a–d Contiguous axial MDCT images show the incomplete high-grade obstruction. Small amount of fluid passed into the distal bowel (arrowheads). An abnormal course of mesenteric vessels (black arrows) is present around the transition zone (white arrows). The patient did not improve on conservative treatment and underwent small-bowel resection. Double arrows luminal diameter

A 43-year-old woman with small-bowel obstruction. a,b Contiguous axial MDCT images show complete degree of obstruction. There is no passage into the small bowel (black arrow) distal to the transition zone (white arrows). An abnormal course of mesenteric vessels is not present around the transition zone. Thickening of bowel wall adjacent to the transition zone (arrowheads) and peritoneal effusion (dots) are also present. The patient was treated conservatively and improved clinically. Follow-up abdominal radiograph (not shown) demonstrated improvement of the small-bowel obstruction. Double arrows luminal diameter
The sensitivities, specificities, PPVs, NPVs, and risks of MDCT for predicting the need for subsequent surgery in patients with an SBO were 100%, 46.1%, 43%, 100%, and 1.9 (1.5 ≤ 95% confidence interval (CI) ≤ 2.2) for a high-grade obstruction; 100%, 23%, 34.5%, 100%, and 1.3 (1.2 ≤ 95% CI ≤ 1.5) for the presence of the transition zone ; and 70.2%, 90.1%, 74.2%, 88.1%, and 7.1 (3.7 ≤ 95% CI ≤ 13.7) for the presence of an abnormal course of the mesenteric vessels, respectively (Table 2).
Discussion
Juggling early surgery and nonoperative management is challenging in the management of SBO due to adhesion. A number of large, retrospective series have reported success with nonoperative management in patients without signs of strangulation, followed by surgery carried out only in selected patients [2, 3, 5, 8, 10, 19]. However, predictors to clinically discern which patients have early reversible ischemia and clinical indicators of impending strangulation have been found to be inconsistent and unreliable [3, 5, 9, 10, 20]. Therefore, there should be a role of the use of CT in the prediction for the need of subsequent surgery in patients with equivocal symptoms of strangulation. Recent advances in CT technology have allowed CT to have a primary role in the evaluation of an SBO [1–5, 11, 13, 19, 20]. The use of MDCT is highly sensitive to diagnose an SBO and provides valuable information for an SBO including the cause, site, degree, and presence of strangulation [1–4, 6, 13, 21]. However, there has been no reported evaluation of the clinical value of the information acquired with the use of MDCT for decision making regarding surgery in patients with an SBO. Furthermore, most radiological studies have analyzed CT features without correlating the clinical symptoms and signs. In the present study, we attempted to evaluate the role of MDCT in predicting the need for subsequent operation and also its correlation with the clinical background in a prospective manner. In general, patients with complete obstruction are prone to require surgery. In operative series, the substantial risk of strangulation in complete obstruction has been consistently reported as between 20 and 40%, which suggests the need for early surgery [3, 5, 21]. However, patients with incomplete obstruction may be treated with a conservative method, initially under clinical supervision [2, 3, 10]. Our results also showed that a higher degree of SBO was more common in the group of patients operated on, which suggests that a higher degree of obstruction can be an indicator of the need for subsequent surgery in patients with an SBO. However, Mallo et al. have indicated in a review that although the accuracy of CT was good for a complete or high-grade SBO, the diagnostic performance for a complete SBO was problematic because of the lack of a “gold standard” [22]. In the present study, we defined the discrepancy of the luminal diameter between the proximal and distal bowel adjacent to the transition zone as being more than three times in complete and incomplete high-grade SBO to obtain interobserver agreement and a higher diagnostic accuracy.
For the transitional zone, the sensitivity of predicting the need for subsequent surgery was 100%. However, the specificity was low (23%) as MDCT can depict more anatomic details and transition zone, even for a low-grade SBO.
In this study, an abnormal course of mesenteric vessels was suggested as an indicator of the need for subsequent surgery. An unusual course of mesenteric vessels is different from mesenteric torsion in terms of the absence of whirling bowel loops, which may be an earlier step of vascular change for an SBO than mesenteric torsion or bowel strangulation, and can be correlated with early pathophysiology of compromised arterial influx. However, an unusual mesenteric vascular course may be a nonspecific finding, so it should be considered as suspicious when seen on CT of patients with an SBO.
Patients who have been demonstrated to have a transmural infarct or microperforation showed no evidence of strangulation or perforation as seen on MDCT. The lack of a CT finding might be due to the aggravation of vascular compromise during the time interval between imaging and surgery.
This study focused on degrees of SBO, presence of the transition zone, and an abnormal vascular course as predictors of subsequent operation in patients with SBO. Other findings such as peritoneal effusion or bowel wall thickening which may be possible predictors of operation in SBO were not considered in this analysis.
This study has several limitations. First, the clinical conditions of the patients could not be controlled regularly according to the consensual protocol of treatment, which might have an effect on the decision making regarding surgery. Second, the patients in the operated group did not undergo follow-up CT at that time of deciding to undergo surgery and the decision totally depended on the clinical status and the findings on plain radiographs, which might give subjectivity to the decision making regarding surgery. However, there were some problems with performing follow-up CT examinations, such as increasing exposure to radiation and additional medical expenses. Third, as mentioned above there is no current consensus of a gold standard for the degree of obstruction. Fourth, this study included a relatively small number of patients in the group operated on. Fifth, it was not possible to discuss patients in the group not operated on. Finally, this study did not include reconstructed images where the findings of SBO may be better evident.
Conclusion
A higher grade of SBO and the presence of the transition zone as seen on MDCT were highly sensitive for the prediction of the need for subsequent surgery in patients with an SBO. However, the presence of the transition zone was not specific. The presence of converging mesenteric vessels around the transition zone was highly specific for the prediction of the need for surgery. Therefore, a high degree of obstruction and the presence of the mesenteric vessels showing an abnormal course around transition zone may be used as useful findings on MDCT to predict the need for subsequent surgery in patients with an SBO due to adhesion.
References
Delabrousse E, Destrumelle N, Brunelle S, Clair C, Mantion G, Kastler B (2003) CT of small bowel obstruction in adults. Abdom Imaging 28:257–266
Maglinte DD, Heitkamp DE, Howard TJ, Kelvin FM, Lappas JC (2003) Current concepts in imaging of small bowel obstruction. Radiol Clin North Am 41:263–283, vi
Hayanga AJ, Bass-Wilkins K, Bulkley GB (2005) Current management of small-bowel obstruction. Adv Surg 39:1–33
Scaglione M, Romano S, Pinto F, Flagiello F, Farina R, Acampora C, Romano L (2004) Helical CT diagnosis of small bowel obstruction in the acute clinical setting. Eur J Radiol 50:15–22
Kim JH, Ha HK, Kim JK, Eun HW, Park KB, Kim BS, Kim TK, Kim JC, Auh YH (2004) Usefulness of known computed tomography and clinical criteria for diagnosing strangulation in small-bowel obstruction: analysis of true and false interpretation groups in computed tomography. World J Surg 28:63–68
Burkill G, Bell J, Healy J (2001) Small bowel obstruction: the role of computed tomography in its diagnosis and management with reference to other imaging modalities. Eur Radiol 11:1405–1422
Zalcman M, Sy M, Donckier V, Closset J, Gansbeke DV (2000) Helical CT signs in the diagnosis of intestinal ischemia in small-bowel obstruction. AJR Am J Roentgenol 175:1601–1607
Shih SC, Jeng KS, Lin SC, Kao CR, Chou SY, Wang HY, Chang WH, Chu CH, Wang TE (2003) Adhesive small bowel obstruction: how long can patients tolerate conservative treatment? World J Gastroenterol 9:603–605
Frager D, Medwid SW, Baer JW, Mollinelli B, Friedman M (1994) CT of small-bowel obstruction: value in establishing the diagnosis and determining the degree and cause. AJR Am J Roentgenol 162:37–41
Markogiannakis H, Messaris E, Dardamanis D, Pararas N, Tzertzemelis D, Giannopoulos P, Larentzakis A, Lagoudianakis E, Manouras A, Bramis I (2007) Acute mechanical bowel obstruction: clinical presentation, etiology, management and outcome. World J Gastroenterol 13:432–437
Burkill GJ, Bell JR, Healy JC (2001) The utility of computed tomography in acute small bowel obstruction. Clin Radiol 56:350–359
Maglinte DD, Gage SN, Harmon BH, Kelvin FM, Hage JP, Chua GT, Ng AC, Graffis RF, Chernish SM (1993) Obstruction of the small intestine: accuracy and role of CT in diagnosis. Radiology 188:61–64
Furukawa A, Yamasaki M, Furuichi K, Yokoyama K, Nagata T, Takahashi M, Murata K, Sakamoto T (2001) Helical CT in the diagnosis of small bowel obstruction. Radiographics 21:341–355
Balthazar EJ, Birnbaum BA, Megibow AJ, Gordon RB, Whelan CA, Hulnick DH (1992) Closed-loop and strangulating intestinal obstruction: CT signs. Radiology 185:769–775
Ha HK, Kim JS, Lee MS, Lee HJ, Jeong YK, Kim PN, Lee MG, Kim KW, Kim MY, Auh YH (1997) Differentiation of simple and strangulated small-bowel obstructions: usefulness of known CT criteria. Radiology 204:507–512
Boudiaf M, Soyer P, Terem C, Pelage JP, Maissiat E, Rymer R (2001) Ct evaluation of small bowel obstruction. Radiographics 21:613–624
Balthazar EJ, Liebeskind ME, Macari M (1997) Intestinal ischemia in patients in whom small bowel obstruction is suspected: evaluation of accuracy, limitations, and clinical implications of CT in diagnosis. Radiology 205:519–522
Sheedy SP, Earnest FT, Fletcher JG, Fidler JL, Hoskin TL (2006) CT of small-bowel ischemia associated with obstruction in emergency department patients: diagnostic performance evaluation. Radiology 241:729–736
Taourel PG, Fabre JM, Pradel JA, Seneterre EJ, Megibow AJ, Bruel JM (1995) Value of CT in the diagnosis and management of patients with suspected acute small-bowel obstruction. AJR Am J Roentgenol 165:1187–1192
Donckier V, Closset J, Van Gansbeke D, Zalcman M, Sy M, Houben JJ, Lambilliotte JP (1998) Contribution of computed tomography to decision making in the management of adhesive small bowel obstruction. Br J Surg 85:1071–1074
Sarr MG, Bulkley GB, Zuidema GD (1983) Preoperative recognition of intestinal strangulation obstruction. Prospective evaluation of diagnostic capability. Am J Surg 145:176–182
Mallo RD, Salem L, Lalani T, Flum DR (2005) Computed tomography diagnosis of ischemia and complete obstruction in small bowel obstruction: a systematic review. J Gastrointest Surg 9:690–694
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hwang, JY., Lee, J.K., Lee, J.E. et al. Value of multidetector CT in decision making regarding surgery in patients with small-bowel obstruction due to adhesion. Eur Radiol 19, 2425–2431 (2009). https://doi.org/10.1007/s00330-009-1424-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-009-1424-4