
Abstract
The accuracy of panoramic radiography (RX) and ultrasound (US) in the evaluation of both the length of the osteotomic gap and the quality of new bone formation in patients undergoing mandibular distraction osteogenesis (DO) was assessed, verifying the results against intraoperative and histologic findings. In 31 patients, three RX and three US examinations were performed after DO. RX and US findings were each independently compared, at the time of distractor removal, to the direct intraoperative measurement of the osteotomic gap and to the histologic evaluation of the maturity of a resected specimen. No significant differences (P > 0.1) resulted at any step between RX (average length: 18.19 mm) and US (18.29 mm) measurement of the osteotomic gap. In the assessment of the callus maturity the difference between RX and US (P < 0.001) was statistically significant: at the final control the maturity score averaged 0.612 at RX, 3 at US and 3 at histology. RX and US are equally reliable in the measurement of the osteotomic gap, while US is much more accurate than RX in the evaluation of the callus maturity. US-based follow-up might allow a safe shortening of the fixation period.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
First described in 1969 [1], distraction osteogenesis (DO) has rapidly become a well-established technique in the lengthening of underdeveloped long bones, which has eventually been applied to mandibles [2, 3]. Mandibular expansion by means of horizontal or vertical DO allows a minimally invasive approach, short operation time, elimination of bone grafts and simultaneous soft tissue expansion [3–5]. The main disadvantage of mandibular DO is the long duration of treatment [6]: currently used protocols are derived from those designed for long bones [7], where a minimum latency period of 5–7 days, a distraction rate not exceeding 1 mm per day and an average fixation period of 50–60 days after the end of active lengthening are requested [8, 9]. A shorter fixation period might probably be applied to mandibles [10] if reliable means of DO monitoring were available; in particular, if it would be possible to state beyond doubt when the mineralization of the bone regenerate allows a safe removal of the distraction device.
In addition to its cost and radiation exposure [11], panoramic radiography (RX) is not useful in the first period of fixation, being inadequate to image noncalcified structures like bone regenerate before the onset of mineralization [12–17]. Although its expected accuracy is higher than RX’s, computed tomography (CT) is often significantly limited by the metal artifacts arising from the distraction devices; it is more expensive than RX, radiation dose is higher and sedation is necessary in young and uncooperative patients [18, 19].
Ultrasound (US)-based follow-up of DO in limb lengthening was introduced several years ago [11, 13, 20], obtaining both precise measurement of the gap between the bone edges and early detection of foci of ossification within the bone regenerate, and therefore achieving accurate and noninvasive evaluation of the rate and quality of callus formation. In more recent years, some authors successfully applied US to the monitoring of callus in mandibles undergoing lengthening with iliac graft and with vascularized fibula flaps [21, 22] and eventually to mandibles treated with DO [15–17, 21–23].
The purpose of this paper was to assess the accuracy of RX and US in defining both the distance between the bone edges and the rate and quality of callus formation in a series of patients undergoing either horizontal or vertical DO of the mandible, verifying the reliability of the methods against the intraoperative and histologic findings obtained after removal of the surgical devices; in particular, we sought to demonstrate the usefulness of US as the sole means of management in these patients.
Materials and methods
Informed consent was obtained by all patients prior to inclusion in this study, which was approved by research ethics committee board.
Surgical procedure
Between July 2002 and July 2006 31 patients (14 males and 17 females), aged between 18 and 65 (average age: 33.5 years), underwent mandibular DO. The underlying conditions were mandibular hypoplasia (14 cases), atrophy (six cases) and acquired mandibular deformity due to previous surgery (eight cases) or to trauma (three cases).
Osteotomy of the mandibular body was performed in all patients, either along the vertical axis (this approach, named “horizontal distraction” after the direction of new bone growth, was applied in 18 cases: Figs. 1a, 2) or horizontally (“vertical osteotomy”: 13 cases—Figs. 1b, 3), aiming to stimulate sagittal bone apposition. Osteotomies performed in portions of the mandible other than the body (i.e., mandibular ramus) as well as surgical lengthening procedures different from DO (such as elongation by means of iliac bone or fibular grafts) were excluded from this study.

Intraoperative photographs after fixation to the mandible, across a horizontal (a) and a vertical (b) osteotomy, of extraosseous distraction devices

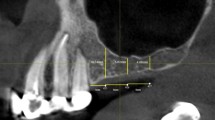
Follow-up transverse sonographic scans at times T0 (a), T1 (b) and T2 (c) after horizontal distraction demonstrate the ongoing mineralization of the bone regenerate visible between long arrows (a) and calipers (b, c). At time T2 a new cortical layer is clearly seen at US (short arrow in c); in the radiogram obtained at the same time (d) little if any mineralization can be detected within the osteotomic gap

Follow-up sagittal sonographic scans at times T0 (a), T1 (b) and T2 (c) after vertical distraction demonstrate the progressive increase in echogenicity of the bone regenerate visible between calipers (a, c) and arrows (b); at time T2 the appearance of the callus is much more similar to the adjacent normal bone at US (c) than it is at RX (d)
After osteotomy, an extraosseous distraction device was fixed to the mandible across the corticotomy with two or three 2-mm-diameter screws on each side. Following a latency period of 7 days, distraction was performed for 12–45 days at a rate of 0.5–1 mm per day (0.25–0.5 mm twice a day), achieving a final lengthening of 8–28 mm (average: 18.2). In the subsequent neutral fixation period lasting 50–70 days no distraction was performed; the distraction device was surgically removed at the end of this period, i.e., when the mineralization process was judged to be complete at US. At surgery, the distance between the osteotomic segments was directly measured, while the maturity of bone regenerate was determined at histologic examination of a surgically removed specimen on the basis of a four-point scale (0: presence of soft tissue only; 1: scattered bony islands; 2: mineralization of more than 50% of bone regenerate; 3: complete mineralization).
Imaging-based follow-up
All patients underwent both RX and US follow-up at the first day after suspension of active lengthening (time T0), at mid-term (T1) of the period of neutral fixation scheduled preoperatively on the basis of the expected callus length (between 25 and 35 days after T0) and (time T2) as early as it was considered possible – should the mineralization of the bone regenerate be judged complete – to remove the distraction device (50–70 days after surgery). RX was performed by means of a digital panoramic radiography (Orthophos; Sirona Dental Systems, Bensheim, Germany). The US study was performed with a linear transducer (frequency range: 4–8 MHz; frequency used: 8 MHz) on a digital last-generation scanner (Sequoia Systems; Acuson, Mountain View, Calif., USA); US scans were always conducted perpendicular to the osteotomic rim. At each control the distance across the osteotomy was measured with both modalities keeping 1-mm approximation; the state of bone regeneration was evaluated on the same four-point scale used at histology.
All US examinations were independently performed, within the same day, by two operators (C.B. and S.M., both of them radiologists with 10 years of experience with sonography and RX), blinded to each other and to the surgical and histologic findings, who recorded the osteotomic gap length and the maturity of the bone regenerate at the end of each examination. The same two operators, in a different session, independently reviewed the radiographs of all patients. In case of discrepancy between the two observers with both imaging modalities, a final judgement was reached by consensus.
Analysis of the results
RX and US were each independently compared with the result of intraoperative measurement to determine their accuracy in the evaluation of the distance across the osteotomy. In the assessment of the maturity of the bone regenerate, the score achieved at the histologic examination of the resected callus specimen was considered the “gold standard”. The statistical significance of the differences between the performances of RX and US was evaluated by means of paired Student’s t-test.
Results
Measurement of the distance across the osteotomy
As shown in Table 1, no statistically significant differences emerged, at any step of the follow-up, between RX and US measurement of the osteotomic gap; the space left between the bony edges, as it was evaluated at surgical exploration, was correctly defined by both methods and the ongoing mineralization of the bone regenerate did not affect the measurement. A consensus was not necessary in any case, since the measurements made by both observers with both methods never differed by more than 1 mm.
Assessment of the maturity of the bone regenerate
Both at times T1 and T2 the maturity score of the bone regenerate measured by US was higher than the corresponding figure obtained with RX (Table 2); in particular, RX detected no mineralization in any patient at time T1, while at time T2 12 patients scored zero and 19 patients scored 1. The difference between the RX and US results was highly significant at statistical analysis at both times (Table 2). The two observers agreed in the assignment of the sonographic maturity score to all patients, while in three cases a consensus was necessary in the radiographic evaluation because of a one-point difference.
Discussion
From a theoretical point of view, no obstacle exists to the ultrasonographic evaluation of both the length of the gap across the osteotomy and the degree of mineralization of the bone callus, which are the most important parameters in the evaluation of the bone regenerate in healing distraction wounds. Before the development of a new cortical layer, the US beam is not reflected and can easily penetrate into the distraction gap. In such an echolucent window, new bone apposition can be identified as small echogenic islands appearing during the first week of neutral fixation in the inner portion of the osteotomy, progressively increasing in volume and coalescing and finally leading to a sharp decrease in ultrasound beam penetration depth [24]. The final event of bone regeneration is the formation of an outer cortical layer, which requires 30–80 days of neutral fixation [24] and is demonstrated at US by the onset of a beam-reflecting hyperechoic surface, not distinguishable—except for its margins—from the adjacent native bone; in the posterior acoustic shadowing, no artifactual reverberation echoes are detected, which allows differentiation of the new bony surface from oral gas.
Although in a limited number of papers, US has been successfully used in the follow-up of limb lengthening: both the length of the gap between the fragments and formation and maturity of bone regenerate have been reliably assessed [11, 13, 18, 20, 25]. In very few studies, a positive correlation between US and histologic findings was demonstrated [20, 26]; in particular, in a model based upon experimental tibial fractures in dogs, mineralized bone was detected at histology in the areas of high echogenicity, while iso- or hypoechoic portions contained fibrous tissue [26]. To our knowledge there are no published papers in which a quantitative or semiquantitative sonographic evaluation of the callus mineralization, compared with histology, was obtained.
In one experimental study on porcine mandibular distraction wounds [24] and in the published papers on human mandibular DO [16, 17, 22–24], US proved accurate in the measurement of the gap across the osteotomy and in the evaluation of callus formation; in one study in which a correlation between the two imaging modalities was made, US detected bone formation much earlier than RX [16]. In the sole available correlation study between surgical findings and prior US and RX data [15], US exactly predicted intraoperative mandibular stability scores in 14/18 cases versus 3/18 cases correctly judged by RX, the latter modality underestimating stability in 14/18 cases; however, histologic confirmation was not obtained.
In our experience, US accuracy was as high as that of RX in the determination of the distance across the osteotomy (Table 1), which can be easily forecast on the basis of the sharp difference both in echolucency and in radiographic density between normal mandibular bone and regenerate, until the end of treatment; the absence of radiation exposure and the lower cost make US preferable.
On the other hand, obtaining reliable information about the progress of mineralization of bone regenerate is crucial in the management of the patients treated with mandibular DO. According to the time thought to be necessary to achieve maturity of a callus of given length, the duration of the fixation period is empirically chosen; if histologic maturation is completed earlier, however, any prolongation of the fixation period is unnecessary and the distraction device can be safely removed. Our data, supported by histology, suggest a highly significant advantage of US over RX (Table 2). Although its high atomic number usually makes calcium easily detectable at radiography, a minimum thickness of calcified material is needed in order to identify both bony islands within the osteotomic gap and outer cortical layer at RX; this latency is probably slightly increased by the digital panoramic radiographies currently used.
The main aim of this study was to obtain histologic confirmation of the ability of US to grade the ongoing mineralization of bone regenerate in mandibular DO; therefore, a significant reduction of the length of the neutral fixation period in comparison with the protocols used in limb lengthening [8–10] was not achieved. However, in this series the callus mineralization assessed by US was the only criterion directing the removal of the distractor, which in 6/31 patients—whose sonographic maturity score at time T1 was 2—resulted in shortening of the interval between T1 and T2 and eventually, after scoring 3 at time T2, in distractor removal earlier than initially scheduled.
Some limitations can be found in this study. Although the agreement between the two observers was definitely high, the maturity score was assigned to each patient on the basis of a subjective assessment. Since the degree of mineralization assessed with US was used to decide when to remove the distraction device and obtain the histologic specimen, a verification bias was introduced. Moreover, since we chose to include only those patients in whom DO of the mandibular body was performed, our series is limited to 31 subjects. Finally, we did not use X-ray-based techniques different from digital panoramic radiography (e.g., conventional tomography or CT) to evaluate roentgenographic signs of bone maturation.
In conclusion, this study demonstrates the feasibility of US-based management of mandibular DO, with US being as accurate as RX in the measurement of the osteotomic gap and much more reliable than RX in the assessment of the maturity of the bone regenerate. US-based follow-up will reasonably result in anticipation of distractor removal in a percentage of patients.
References
Ilizarov GA, Soibel’man LM (1969) Some clinical and experimental data on the bloodless lengthening of lower extremities. Eksp Khir Anesteziol 14:27–32
McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH (1992) Lengthening the human mandible by gradual distraction. Plast Reconstr Surg 89:1–8
McTavish J, Marucci DD, Bonar SF, Walsh WR, Poole MD (2000) Does the sheep mandible relapse following lengthening by distraction osteogenesis? J Oral Maxillofac Surg 58:251–257
Troulis MJ, Perrott DH, Kaban LB (1999) Endoscopic mandibular osteotomy, and placement and activation of a semiburied distractor. J Oral Maxillofac Surg 57:1110–1113
Castano FJ, Troulis MJ, Glowacki J, Kaban LB, Yates KE (2001) Proliferation of masseter myocytes after distraction osteogenesis of the porcine mandible. J Oral Maxillofac Surg 59:302–307
Tavakoli K, Walsh WR, Bonar F, Smart R, Wulf S, Poole MD (1998) The role of latency in mandibular osteodistraction. J Craniomaxillofac Surg 26:209–219
Ilizarov GA (1989) The tension-stress effect on the genesis and growth of tissues. Part II: the influence of the rate and frequency of distraction. Clin Orthop 238:263–285
Padwa BL, Kearns GJ, Todd R, Troulis MJ, Mulliken JB, Kaban LB (1999) Simultaneous maxillary and mandibular distraction osteogenesis: a technique and case report. Int J Oral Maxillofac Surg 28:2–8
Mofid MM, Manson PM, Robertson BC, Tufaro AP, Elias JJ, Vanderkolk CA (2001) Craniofacial distraction osteogenesis: a review of 3278 cases. Plast Reconstr Surg 108:1103–1114
Troulis MJ, Glowacki J, Perrott DH, Kaban LB (2000) Effects of latency and rate on bone formation in a porcine mandibular distraction model. J Oral Maxillofac Surg 58:507–513
Maffulli N, Hughes TH, Fixsen JA (1992) Ultrasonographic monitoring of limb lengthening. J Bone Joint Surg 74:130–132
Nicholls PJ, Berg E, Bliven FE, Kling JM (1979) X-ray diagnosis of healing fractures in rabbits. Clin Orthop 142:234–236
Derbyshire ND, Simpson AH (1992) A role for ultrasound in limb lengthening. Br J Radiol 65:576–580
Malde HM, Hemmadi SS, Chadda D, Parihar ML, Bhosale PB, Kedar RP (1993) The role of skeletal sonography in limb lengthening procedures. J Postgrad Med 39:127–129
Troulis MJ, Coppe C, O’Neill MJ, Kaban LB (2003) Ultrasound: assessment of the distraction osteogenesis wound in patients undergoing mandibular lengthening. J Oral Maxillofac Surg 61:1144–1149
Juenger TH, Klingmueller V, Howaldt HP (1999) Application of ultrasound in callus distraction of the hypoplastic mandible: an additional method for the follow-up. J Craniomaxillofac Surg 27:160–167
Nocini PF, Albanese M, Wangerin K, Fior A, Trevisiol L, Kretschmer W (2002) Distraction osteogenesis of the mandible: evaluation of callus distraction by B-scan ultrasonography. J Craniomaxillofac Surg 30:286–291
Hughes TH, Maffulli N, Green V, Fixsen JA (1994) Imaging in bone lengthening. Clin Orthop 308:50–53
Smith SW, Sachdeva RC, Cope JB (1999) Evaluation of the consolidation period during osteodistraction using computed tomography. Am J Orthod Dentofac Orthop 116:254–263
Young JW, Kostrubiak IS, Resnik CS, Paley D (1990) Sonographic evaluation of bone production at the distraction site in Ilizarov limb-lengthening procedures. AJR Am J Roentgenol 154:125–128
Friedrich RE, Hellner D, Plambeck K, Schmelzle R (1997) Application of B-scan ultrasonography for analysis of callus distraction in vascularized fibular grafts of the mandible: a report of three patients. J Oral Maxillofac Surg 55:635–640
Nocini PF, Wangerin K, Albanese M, Kretschmer W, Cortelazzi R (2000) Vertical distraction of a free vascularized fibula flap in a reconstructed hemimandible: case report. J Craniomaxillofac Surg 28:20–24
Hirai T, Manders EK, Nagamoto K, Saggers GC (1996) Ultrasonic observation of facial bone fractures: report of cases. J Oral Maxillofac Surg 54:776–779
Thurmueller P, Troulis MJ, O’Neill MJ, Kaban LB (2002) Use of ultrasound to assess healing of a mandibular distraction wound. J Oral Maxillofac Surg 60:1038–1044
Blane CE, Herzenberg JE, Di Pietro MA (1991) Radiographic imaging for Ilizarov lengthening in children. Pediatr Radiol 21:117–120
Moed BR, Kim EC, Van Holsbeeck M, Schaffler MB, Subramanian S, Bouffard JA, Craig JG (1998) Ultrasound for the early diagnosis of tibial fracture healing after static interlocked nailing without reaming: histologic correlation using a canine model. J Orthop Trauma 12:200–205
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bruno, C., Minniti, S., Buttura-da-Prato, E. et al. Gray-scale ultrasonography in the evaluation of bone callus in distraction osteogenesis of the mandible: initial findings. Eur Radiol 18, 1012–1017 (2008). https://doi.org/10.1007/s00330-008-0856-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-008-0856-6